Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
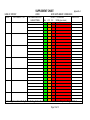
Adults and Community Division NUTRITIONAL GUIDELINES Specific to Community Hospitals (In-patient services) Summary of Guidelines The overall aim of this guideline is to improve the nutritional care of patients by identifying patients at risk of malnutrition and providing nutritional support Method of Approval : Divisional Managers Meeting Originating Department : Community Nutrition & Dietetic Department Date of Issue : November 2009 Review Date : November 2011 Impact Assessment Date : June 2009 Page 1 of 31 Contents Page 1. Introduction 3 2. Background 3 3. Statement of Purpose 4 4. Nutritional Screening 4 5. Weighing the Patient and obtaining the Patient‟s height: Calculation of body mass index (BMI) 4 6. Provision of Food and Drink 5 7. Dietitian Support 5 8. Nurses Responsibilities 6 9. Rehabilitation Assistants Responsibilities 6 10. Housekeepers‟ Responsibilities 7 11. Discharge of Patients 7 12. Documentation 7 13. Training 8 14. Monitoring 8 13. References 9 Appendices 1-10 11 - 31 Page 2 of 31 NUTRITIONAL GUIDELINES 1. Introduction The aim of this guideline is to improve the nutritional care of patients provided within South Birmingham Community Hospitals. Good nutritional care requires a multi-disciplinary, evidenced-based approach focusing on assessment and identification of the “at risk” patient. 2. Background A number of studies have demonstrated that malnutrition remains an issue and it tends to worsen during hospitalisation. Malnutrition is under-recognised and under-treated (BAPEN, 2008). The nutrition screening survey in the UK in 2008 (BAPEN, 2008) showed that malnutrition is common on admission to community hospitals. McWhirter and Pennington (1994) revealed that two in five adults admitted to hospital were malnourished. Most of them received no nutritional support and lost more weight during their stay. Low body weight and poor nutritional status have been linked to increased complications during illness, delayed postoperative recovery, longer hospital stays and increased morbidity (Green, 1999 and BAPEN, 2008). Only 5% of malnourished hospital patients received nutritional support. Of these, most gained weight, and their nutritional status improved (McWhirter and Pennington, 1994). The evidence suggests that the solution lies in identifying “at risk” patients. "Hungry in Hospital?" a report from the Association of Community Health Councils (1997) highlighted the problem that patients do not receive adequate food or fluids in hospital; their observations included: Patients who were incapable of choosing meals left to complete their menu order. Lack of nursing assistance at mealtimes. Patients who were not given the appropriate cutlery/utensils to eat with. The British Association for Parenteral and Enteral Nutrition (BAPEN) has provided the research and evidence base to demonstrate the link between under-nutrition and ill health. This is provided in the „MUST‟ report (BAPEN, 2003), the cost of disease-related malnutrition in the UK (Elia, 2006) and Combating Malnutrition: Recommendations for Action (Elia, 2008). The Royal College of Nursing (RCN) has signalled its commitment to addressing this issue through its Nutrition Now Campaign (2008), which aims to help nurses at all levels improve the nutrition and hydration of patients. The Hospital Caterers Association (HCA) also highlighted this as an important issue through its 2007 National Service Excellence Day. Staff throughout the country were provided with practice advice and tips on how to make a difference. Key documents have been produced within the last 6 years which provide guidance and recommendations for the implementation of national guidance in food and nutritional care in hospitals. These documents include:10 Key Characteristics of good nutritional care in hospitals (2003) (appendix 10) Improving Nutritional Care (Department of Health, 2007) Essence of Care (Department of Health, 2001) Page 3 of 31 3. Statement of Purpose All patients will receive good quality nutritious food taking account of individual needs, cultural and religious beliefs, served to them by members of staff who understand the important role food plays in the care, recovery and social wellbeing of adults. In addition, patients who require nutritional support and/or specialised dietetic intervention will be identified and treated accordingly with dignity, respect, fairness and sensitivity. 4. Nutritional Screening All patients on admission will be screened using the „MUST‟ (Malnutrition Universal Screening Tool) (appendix 1 & 9). This nutritional screening will be repeated weekly for patients identified as being at risk of malnutrition, (Department of Health, 2003), (NICE 2006), (10 Key Characteristics of good nutritional care in hospitals, 2003). Actions identified from the nutritional screening tool will be implemented by nursing staff. This may include: Implementation of multidisciplinary action plan for patients with small appetites (appendix 3). Referrals to (as appropriate): o Dietitian o Speech and Language Therapist o Dentist o Occupational Therapist o Social Worker 5. Weighing the Patient and obtaining the Patient‟s height: Calculation of BMI All patients should be weighed to monitor body weight changes according to their care plan. All scales should be calibrated annually (BAPEN, 2008 and Department of Health, 2008). It is recommended that all patients should be weighed and a height measurement taken (or estimated) on admission. The patient‟s weight (kg) and height (m) should be recorded on the record of „MUST‟ Nutritional Screening and Action Taken Sheet (Appendix 2). See the „MUST‟ Explanatory Booklet if alternative measurements for body mass index (BMI) or height or alternative considerations are required. It is recommended that ulna length is used if unable to obtain an accurate height measurement and that mid upper arm circumference (MUAC) is used to estimate BMI category if unable to obtain an accurate height or weight measurement. If the patient cannot or declines to be weighed/measured this should be documented on the record of „MUST‟ Nutritional Screening and Action Taken sheet (appendix 2). This should be reattempted as per recommendations on care plan. Calculation of BMI – refer to BMI calculation table included in the „MUST‟ tool. If neither BMI or weight loss can be established, a subjective assessment should be made to assess overall risk of malnutrition and this should be documented on the record of „MUST‟ Nutritional Screening and Action Taken sheet (appendix 2). The patient‟s weight and BMI should be reviewed on a weekly basis for every patient identified “at risk” of malnutrition. Page 4 of 31 6. Provision of Food and Drink This will be in line with the “Better Hospital Food” requirements (Department of Health, 2000) and the 10 Key Characteristics of Good Nutritional Care in Hospitals. The patients will receive the care and assistance they require with eating and drinking, be able to access food and drink at any time in a conducive environment. Ward based areas will operate a protected mealtimes policy, thus reducing inappropriate activity at mealtimes. However, relatives are to be encouraged where assisted feeding is required. Patients should be involved in the planning and monitoring arrangements for food service provision. These include provision of24 hour ward kitchen service Snack boxes (menus available at ward level) Light bites (menus available at ward level) NHS menu, including special diets, cultural & wellbeing diets A minimum of 7 drinks served per day Drinking water available at the patients bedside (water jugs to be refreshed at least 3 times a day) RGN‟s will have overall responsibility for the nutrition of their patients Ward Housekeepers will help patients with their menu‟s and ensuring that individual preferences and therapeutic needs are met Red tray system to be used with patients identified as needing assisted feeding Food textures as recommended by Speech and Language Therapists are provided (see modified texture chart appendix 8) and must be adhered to. Nurses will ensure that appropriate nutritional supplements are provided and use the appropriate drinking vessel as recommended by Speech and Language Therapist (if required) A range of equipment is available to meet individual patient needs and promote independence Staff are to ensure that food is served at the correct temperature Food is available and served in a way that meets cultural and religious needs 7. Dietitian Support A Registered Dietitian will assess the patients who are identified as being at high risk of malnutrition or those requesting specialised Dietitian intervention. The Dietitian will determine and document a nutritional care plan. If the Dietitian feels further review or Dietetic monitoring is necessary they will indicate this on the Dietetic Nutrition Care Plan (appendix 6). Otherwise Dietetic review will be at the request of the ward staff via re-referral to the Dietetic Department. Page 5 of 31 8. Nurses Responsibilities Oversee Nutritional screening using the „MUST‟ screening tool (appendix 1 & 9) ensuring that it takes place for all patients on admission and weekly for patients where there is clinical concern. Implement appropriate nutrition care plans following screening. This could include implementing a “red tray” system for identified patients (Hungry to be Heard, Age Concern, 2006). Oversee the Multidisciplinary Action Plan for Patients with Small Appetites (appendix 3) and Dietetic Nutrition Care Plan sheet (appendix 6) where appropriate. Ensure patients have access to diet and fluids and assist and encourage patients with diet and fluids, including the provision of adaptive aids wherever possible. Work with voluntary sector organisations and community care services to consider how provision for additional assistance with eating can be given to those who need it, for instance by using trained volunteers to help at mealtimes. Oversee the provision of nutritional supplements to patients as directed by the Dietitian and ensure they are evenly spaced between meals. Seek and act on feedback from service users on nutritional issues and their experiences of mealtimes. Prioritise training for staff in nutritional care and assistance with eating and set aside training time for staff to complete the NHS core learning module on nutritional care and assistance with eating and attend training sessions when required. Review discharge procedures to ensure that whatever accommodation an older person is returning to (e.g. own home or sheltered housing) appropriate arrangements are in place to ensure continuity of nutritional care. Communicate discharge plans with Dietitians in a timely way and ensure (where directed by the Dietitian) discharged patients have one week‟s supply of nutritional supplements upon discharge and a nutrition support information discharge pack. 9. Rehabilitation Assistants Responsibilities Liaise with Dietitian/Nursing Staff/Housekeepers and report on the progress of individual nutritional care plans. Implement appropriate nutrition care plans following screening. This could include implementing a “red tray” system for identified patients (Hungry to be Heard, Age Concern, 2006). Oversee the Multidisciplinary Action Plan for Patients with Small Appetites (appendix 3) and Dietetic Nutrition Care Plan sheet (appendix 6) where appropriate. Ensure patients have access to diet and fluids and assist and encourage patients with diet and fluids, including the provision of (and assistance with) adaptive aids wherever possible. Monitor patient‟s nutritional intake and complete food record charts where appropriate (appendix 5). Liaise with housekeepers and nursing staff in order to identify suitable patients for adaptive cutlery and drinking aids and ensure texture and consistency recommendations provided by Speech and Language Therapists are adhered too. Provision of nutritional supplements to patients as directed by the Dietitian and ensuring they are evenly spaced between meals. Documented on the supplement record (appendix 4). Weigh patients weekly and record this on the record of „MUST‟ nutritional screening and action taken sheet (appendix 2). Report any concerns to nursing staff. Seek and act on feedback from service users on nutritional issues and their experiences of mealtimes. Page 6 of 31 Ward Rehabilitation Assistants who have undertaken appropriate training will assist to monitor patients who are at nutritional risk including patients who are referred to the Dietitian using the report on progress/individualised care plan (appendix 6). 10. Housekeepers Responsibilities Responsible for serving drinks and snacks to patients at regular intervals (minimum of 7 per day), providing and encouraging patients with nutritional supplements (as recommended on an individual patient basis if required). Refreshing drinking water jugs (at least three times a day) and highlighting any areas of concern regarding patients‟ fluid intake to nursing staff. Implementing advice from the nutrition care plans (appendix 3 and 6), following the “red tray” system for identified patients and ordering meals for patients (encouraging suitable menu choices). Preparing the environment for mealtimes, food service and portion size control. Liaise with rehabilitation assistants and nursing staff in order to identify suitable patients for adaptive cutlery and drinking aids and ensure texture and consistency recommendations provided by Speech and Language Therapists are adhered too. Seek and act on feedback from service users regarding nutrition issues and the mealtime experience. 11. Discharge of Patients Continuity of nutritional care should be routinely followed through into discharge planning with nutritional information included in the discharge communications for those patients identified as „malnourished‟ (BAPEN, 2008). A Dietitian will input into a discharge plan and arrange appropriate follow-up when informed of discharge arrangements (see appendix 7 – Guidelines for Dietetic follow-up of patients discharged from a Community Hospital). 12. Documentation All wards will have an up to date copy of the Nutrition Manual provided by the Dietetic department. It is the ward‟s responsibility to ensure this is accessible and utilised within the ward. Nutritional scores, patients‟ height and weights will be recorded on the Record of „MUST‟ Nutritional Screening and Action Taken sheet, including date and signature and repeated weekly (appendix 2). Nutritional supplements given will be recorded, timed, dated and signed off on the supplement intake chart (appendix 4). Quantity drunk will also be documented on this chart. Food intake will be documented on a food diary where indicated (appendix 5). Nursing updates regarding food intake will be recorded in the patient records (appendix 6). Enteral feeds will be documented on the fluid balance chart. Nutrition action/comments will be recorded on the Report on progress/Individualised care plan (appendix 6). Page 7 of 31 13. Training All staff to have access to NHS Core Learning unit – Food, Nutrition and Hydration in Health and Social Care E-Learning Training Programme. Nursing staff, rehabilitation assistants and housekeepers to demonstrate completion of the programme through their professional development review (overseen by the line manager). All staff to have access to training on use of the „MUST‟ nutritional screening tool and nursing staff, rehabilitation assistants and housekeepers to demonstrate completion of annual update on using the tool through their professional development review. This training is to be provided by Nutricia personnel and is in association with the Birmingham Community Nutrition and Dietetic Service and forms part of the contractual agreement for the enteral feeding provision. Specific nutritional training will be provided by the Birmingham Community Nutrition and Dietetic Service and via a service level agreement. Nutritional training at the appropriate level will be undertaken during the Rehabilitation Assistant course and be part of Housekeeper training. Two Rehabilitation Assistants per ward will undergo training with the Community Dietetic service and assume the responsibilities of the role of Rehabilitation Assistant (Nutrition). All food handlers will undertake statutory training and updates as required by the relevant legislation (overseen by the line manager). Management level trained to Advanced Food Hygiene Supervisory & Chefs trained to Intermediate Level 3 Production Catering Staff trained to Level 1 14. Monitoring RGN‟s will have overall responsibility for the monitoring of their patients‟ Rehabilitation Assistants will assist nurses to monitor and review patients referred to the Dietitian and re-refer for review when appropriate (see Dietetic nutrition care plan, appendix 6). Rehabilitation Assistants will also monitor all ward patients for nutritional problems and highlight these to nursing staff when they arise. Monitoring and audit will be via the Divisional Nutritional Steering Group. Page 8 of 31 15. References Age Concern (2006). Hungry to be Heard: The Scandal of Malnourished Older People in Hospital. London. www.ageconcern.org.uk/ageConcern/hungry2bheard.asp Association of Community Health Councils (1997). „Hungry in Hospital?‟ London: Association of Community Health Councils for England and Wales British Association for Parenteral and Enteral Nutrition (BAPEN) (2008). Nutrition Screening Survey in the UK in 2008 – Hospitals, Care Homes and Mental Health Units. www.bapen.org.uk Council of Europe Resolution Food and Nutritional Care in Hospitals (2003). 10 Key Characteristics of Good Nutritional Care in Hospitals. www.npsa.nhs.uk Department of Health (2008). Estates and Facilities Alert: Patient Weigh Scales. www.dh.gov.uk Department of Health (2000). The NHS Plan: A Plan for Investment, a Plan for Reform. London. www.dh.gov.uk Department of Health (2001). Better Hospital Food Campaign Department of Health (2001). Essence of Care –„Patient-focused benchmarks for clinical governance‟ London, pp 1-12. www.dh.gov.uk Department of Health (2007). Improving Nutritional Care, London, www.dh.gov.uk Elia M, et al (2006). On behalf of The British Association for Parenteral and Enteral Nutrition (BAPEN), „The Cost of Disease-Related Malnutrition in the UK and Economic Considerations for the Use of Oral Nutritional Supplements (ONS) in Adults‟. Elia M, et al (2008). On behalf of the Malnutrition Advisory Group (MAG) of The British Association for Parenteral and Enteral Nutrition (BAPEN) (2008). Combating Malnutrition: Recommendations for Action. www.bapen.org.uk Green C J (1999). On behalf of the council of the British Association of Parenteral and Enteral Nutrition (BAPEN) „Existence, causes and consequences of disease related malnutrition in the hospital and the community and clinical and financial benefits of nutritional intervention‟ Malnutrition Advisory Group (MAG) of The British Association for Parenteral and Enteral Nutrition (BAPEN) (2003). The Malnutrition Universal Screening Tool („MUST‟). www.bapen.org.uk Malnutrition Advisory Group (MAG) of The British Association for Parenteral and Enteral Nutrition (BAPEN) (2003). The „MUST‟ Explanatory Booklet: A Guide to the “Malnutrition Universal Screening Tool („MUST‟)” for Adults. www.bapen.org.uk McWhirter J P, Pennington C R (1994). „Incidence and recognition of malnutrition in hospital „ BMJ 308:945-948 Page 9 of 31 National Institute for Health and Clinical Excellence (NICE) (2006). Nutrition Support in Adults – Oral Nutrition Support, Enteral Tube Feeding and Parenteral Nutrition, Clinical Guidance 32. www.nice.org.uk Royal College of Nursing (2008). Nutrition Now Campaign, London. www.rcn.org.uk/nutritionnow The British Association for Parenteral and Enteral Nutrition (BAPEN) (2003). The „MUST‟ Report: Nutritional Screening of Adults – A Multidisciplinary Responsibility. www.bapen.org.uk The Hospital Caterers Association (HCA) (2007). National Service Excellence Day: Serving Excellence, Enhancing Patient Mealtimes. www.hospitalcaterers.org Water UK (2005). Wise Up On Water!: Hydration and Healthy Ageing. London. www.water.org.uk Page 10 of 31 Appendix 1 Surname: Ward: First Name: Consultant: Registration No.: Date of Birth: NUTRITION SCREENING TOOL and CARE PLAN Instructions for use: Every patient should have their weight, height and nutritional risk score measured on admission. Follow the 5 „MUST‟ steps and refer to the „MUST‟ Explanatory Booklet if alternative measurements or considerations are required. Repeat the screening weekly in order to identify any changes. Record the total score with the date and patient weight on the Record of „MUST‟ Screening and Action Sheet. Document the action you have taken or “none” if no action indicated, on the Record of „MUST‟ screening and Action Sheet. Follow “Multidisciplinary Action Plan for Patients with Small Appetites” and/or “Dietetic Nutrition Care Plan” after screening, should action need to be taken i.e. a ‟MUST‟ of 1 or more. „MUST‟ scoring and Weight should be taken weekly and recorded in the table. Variations in weight should be highlighted to nursing staff and acted on as appropriate. To refer a patient to the Dietitian: A referral form should be completed and faxed to the Nutrition and Dietetic Dept, Springfields Centre 0121 627 8834. After faxing, the form should be filed in the medical notes for completion by the Dietitian. Do not send any referrals in the post to Springfields. The „Malnutrition Universal Screening Tool‟ („MUST‟) is reproduced here with the kind permission of BAPEN (British Association for Parenteral and Enteral Nutrition). For further information on „MUST‟ see www.bapen.org.uk Page 11 of 31 Appendix 2 RECORD OF „MUST‟ NUTRITIONAL SCREENING AND ACTION TAKEN Record date, score, weight and what action you have taken (see Action Plan at foot of page 2) in the table below. Weight change can be plotted on the graph below. Please use clinical judgement when weighing and nutritionally screening patients and comment in the section in the below table e.g. fluid disturbances, amputations, plaster casts and action taken. Patient height ……..m Date…...... Measured/Recalled/Calculated/Other(state method) ………. DATE: WEIGHT (kg): BMI (kg/m2): Step 1 Score: Step 2 Score: Step 3 Score: Overall „MUST‟ Score: ACTION TAKEN: Comments: SIGNATURE: D Weight increase a (kg) t e Start Weight ………Kg Weight decrease (kg) kg +9 +8 +7 +6 +5 +4 +3 +2 +1 -1 -2 -3 -4 -5 -6 -7 -8 -9 Page 12 of 31 DATE: WEIGHT (kg): BMI (kg/m2): Step 1 Score: Step 2 Score: Step 3 Score: Overall „MUST‟ Score: ACTION TAKEN: Comments: SIGNATURE: D Weight increase a (kg) t e Start Weight ………Kg Weight decrease (kg) Action Plan: SCORE 0 No Risk Identified 1 Medium Risk 2 OR MORE High Risk kg +9 +8 +7 +6 +5 +4 +3 +2 +1 -1 -2 -3 -4 -5 -6 -7 -8 -9 ACTION No action necessary Repeat screening weekly Routine clinical care Observations needed. Commence “Multidisciplinary Action Plan For Patients With Small Appetites” Repeat screening and weigh weekly Refer to Dietitian if patient has complications. Treatment needed. Refer to Dietitian Commence „‟Dietetic Nutrition Care Plan‟‟ with the aim to improve and increase overall nutritional intake. Repeat screening and weigh weekly Page 13 of 31 Appendix 3 MULTIDISCIPLINANRY ACTION PLAN FOR PATIENTS WITH SMALL APPETITES INITIAL ACTIONS FOR PATIENTS SCORING 1 ON „MUST‟ 1. Always ask your patient why they are not eating well, you may be able to find other ways of helping e.g., getting appropriate texture menu, cutlery, helping to cut food, getting dentures reviewed, reassuring patients with memory problems that they do not need to pay money etc. If your patient is not eating full meals regularly and has no other complications* 1. Commence food diary (stop after 3 days if patient eating well) 2. Order high energy meals – inform housekeeper 3. Encourage: with meals milk to drink small snacks between meals 4. Give Build-Up between meals – write out supplement chart for housekeeper 5. Weigh weekly 6. Review in one week - see below *Complications: e.g., dysphagia, pressure sores, uncontrolled diabetes, renal failure, coeliac disease. If your patient has a small appetite and complications* 1. Commence above action (points 1-6) 2. Refer to Dietitian 3. Commence Dietetic Nutrition Care Plan. 4. Refer to Speech Therapist if swallowing difficulties identified 5. Consider medical review. 6. Consider pharmacology review AFTER ONE WEEK Review food chart, weight and re-screen patient using „MUST‟ assessment. If no improvement in intake and/or patient at high risk („MUST‟) score If intake improving and patient at low/medium risk („MUST‟) score 1. Continue above action 2. Refer to the Dietitian 3. Commence Dietetic Nutrition Care Plan. 1. Continue above until appetite fully returned Page 14 of 31 SUPPLEMENT CHART NAME OF PATIENT: DATE SUPPLEMENT TYPE WARD: RECOMMENDED DAILY AMOUNT/TIMES Appendix 4 DATE SUPPLEMENT COMMENCED: ALL QUANTITY CONSUMED >1/2 <1/2 NONE (give reason) Review Supplement Use Weekly/Before Starting Continuation Sheet: SIGNATURE Document on “Report on Progress” Sheet. Page 15 of 31 NOTES ON USING FOOD RECORD CHART Appendix 5 Food diaries help Dietitians to calculate a patient‟s nutrient intake and establish what level of dietetic intervention they require. They are also helpful for all staff involved with a patient to obtain a clear picture of a patient‟s actual food intake where there are concerns. When completing the diary please ensure the following is done: Complete dietary intake as accurately as possible for 3 days. Complete fluid intake as accurately as possible for 3 days using a fluid balance chart. Indicate the level of assistance required for feeding the patient, e.g. Full assistance/Cutting up food/Prompting and encouragement/Independent. State the required texture of diet as indicated by Speech and Language Therapist, e.g. texture A-E. Where nutritional supplements have been prescribed, please state what has been prescribed and what has been consumed. Complete the food diary by entering the relevant code to indicate how much of a meal has been eaten and mark with the appropriate colour code. Add any item of food consumed which is not on the list to the „other‟ section including as much detail as possible. File charts in the patient‟s medical notes once completed. Refer to Multidisciplinary Action Plan For Patients With Small Appetites for more information For each meal recorded, the member of staff who has recorded the food taken should sign in the appropriate box Please use food record continuation sheets if further records needed. Please record food intake using the relevant codes and highlight/mark with colour coding as shown. Community Dietitian…………………………………………………………………... Tel: 0121 627 1627 Ext 51484 Fax: 0121 627 8834 (Internal 53443) Page 16 of 31 FOOD RECORD CHART Name …………………………………….. Ward ……………………………………… Diet texture ……………………………... Level of assistance ……………………... Supplements prescribed ..………………………… Date: Date: A ¾ ½ ¼ M R All of standard portion ¾ of standard portion ½ of standard portion ¼ of standard portion Eaten minimal amount Refused Date: BREAKFAST Cereal/porridge Cooked breakfast Toast and butter Other (please specify) Sign: MID-MORNING Snack (please specify) Supplement Sign: LUNCH Main course Sandwich Soup Pudding Custard Ice cream/mousse Other( please specify) Sign: MID-AFTERNOON Snack (please specify) Supplement Sign: EVENING MEAL Main course Sandwich Soup Pudding Custard Ice cream/mousse Sign: Other(please specify) Page 17 of 31 Appendix 6 DIETETIC NUTRITION CARE PLAN Action for patients scoring 2 or above on „MUST‟ Name: _________________________________________ Date DATE: ______________ Implement Small Appetite Action: 1. Order and encourage high energy meal options 2. Encourage: - Milk to drink if liked - Small snacks between meals - Supper snack Record on food record chart where needed 3. Give Build Up between meals or supplements if specified by Dietitian in plan below. Record on supplement chart 4. Weigh patient weekly Record on „MUST‟ Nutritional Screening and Action Taken Sheet 5. Commence food diary / continue if directed by Dietitian Problems Date of dietetic assessment…………… 1. Dysphagia 5. Pressure sores 2. Poor appetite 6. Wound healing (please specify) 3. Weight loss 7. Other (please specify)……………………….….. 4. Special diet (please specify) Aim of Dietetic Intervention 1. Increase Weight 2a. Prevent Weight Loss 2b. Prevent Significant Weight Loss 3. Reduce Weight 4. Improve Nutritional Intake 5. Facilitate Provision of ……………………………….………………. Diet 6 Educate Patient / Carer re: …………………………………………………Diet 7 Provide Suitable Tube Feeding Regime to…………………….. ……………….… 8 Other………………………………………….….. Action Plan to Fulfill Aims 1. 4. 2. 5. 3. 6. Review by Dietitian at request of ward Report on progress over page other……………………………….. Community Dietitian _______________________________________Tel: 0121 627 1627 Ext. 51484 Page 18 of 31 REPORT ON PROGRESS/ INDIVIDUALISED CARE PLAN To be completed by members of the multidisciplinary team as part of the monitoring process. Date Review of Action Points (document action) Name/signature Criteria for requesting review by Dietitian: Weight change in opposite direction to aim of treatment Refusal/dislike of prescribed supplements Change in dietary intake Significant change in clinical condition Discharge date arranged Prior to Discharge: Review supplement use and current appetite Review MUST score Give patient a “nutrition support discharge pack” if „MUST‟ score is 1 or above Request a review by the Dietitian and inform Dietitian of discharge plans if patient is likely to need Dietetic support in the community. If patient has been discharged by the Dietitian during admission but is likely to need support in the community, please re-refer patient to the Dietitian prior to discharge. Page 19 of 31 Appendix 7 Guidelines for the Dietetic Follow-Up of patients Discharged from a Community Hospital Patients who are identified as at risk of malnutrition („MUST‟ score of one or above) will be given a nutrition support information discharge pack by ward staff on discharge from the Community Hospital, this will include healthy eating and food fortification dietary advice leaflets. Dietetic follow-up of patients requiring dietetic treatment on discharge from a community hospital may be achieved in various ways. By means of: 1. Phone call to patient/carer/nursing home/health professional 2. Follow up appointment at ATS clinic 3. Domiciliary visit The above methods will be used in conjunction with a clinical letter or standard information letter to the patient‟s GP and/or other relevant health professionals. For the majority of patients requiring follow -up this will involve 1 contact per discharge. However, some patients will require further follow-up until their nutritional condition is stable. Patients falling into this latter category will include patients being enterally fed in their own homes, patients who were admitted in a severely malnourished state, have pressure sores, or wounds requiring continued and changing nutritional support. Patients Who Will NOT Receive Dietetic Follow-Up Patients requiring special diets admitted to community hospitals for other medical reasons unaffecting their usual dietetic management. Patients receiving nutritional support while on a ward but by the time of discharge have improved sufficiently not to require prescribed nutritional support on discharge. Patients Who May Need to Receive Dietetic Follow-Up After Hospital Discharge 1. 2. 3. 4. Patients with newly diagnosed conditions requiring dietetic treatment, e.g. newly diagnosed diabetes mellitus. Patients requiring prescribed nutritional support to continue after hospital discharge. Patients discharged on diets where food needs to be of an altered consistency. Patients requiring to be fed via a nasogastric or PEG tube. Page 20 of 31 Appendix 8 Texture Modification – Fluid Texture Description of Fluid Texture Appendix 9 Fluid Example Thin Fluid Still Water Water, tea, coffee without milk, diluted squash, spirits, wine. Naturally Thick Fluid Product leaves a coating on an empty glass. Full cream milk, cream liqueurs, Complan, Build Up (made to instructions), Nutriment, commercial sip feeds. Thickened Fluid Fluid to which a commercial thickener has been added to thicken consistency. Stage 1 = (Single cream consistency) • Can be drunk through a straw. • Can be drunk from a cup if advised or preferred. • Leaves a thin coat on the back of a spoon. Stage 2 = (Double cream consistency) • Cannot be drunk through a straw. • Can be drunk from a cup. • Leaves a thick coat on the back of a spoon. Stage 3 = (Very thick custard consistency) • Cannot be drunk through a straw. • Cannot be drunk from a cup. • Needs to be taken with a spoon. Page 21 of 31 Texture Modification – Food TEXTURES C – E used in community hospitals Texture Description of Food Texture Food Examples A • A smooth, pouring, uniform consistency. • A food that has been pureed and sieved to remove particles. • A thickener may be added to maintain stability. • Cannot be eaten with a fork. • Tinned tomato soup • Thin custard • A smooth, uniform consistency. • A food that has been pureed and sieved to remove particles. • A thickener may be added to maintain stability. • Cannot be eaten with a fork. • Drops rather than pours from a spoon but cannot be piped and layered. • Thicker than A. • Soft whipped cream • Thick custard • A thick, smooth, uniform consistency. • A food that has been pureed and sieved to remove particles. • A thickener may be added to maintain stability. • Mousse • Smooth fromage frais B C • Can be eaten with a fork or spoon. • Will hold its own shape on a plate, and can be moulded, layered and piped. • No chewing required. D • Food that is moist, with some variation in texture. • Has not been pureed or Sieved. • These foods may be served or coated with a thick gravy or sauce. • Foods easily mashed with a fork. • Meat should be prepared as C. • Requires very little chewing. • Flaked fish in thick sauce • Stewed apple and thick custard E • Dishes consisting of soft, moist food. • Foods can be broken into pieces with a fork. • Dishes can be made up of solids and thick sauces or gravies. • Avoid foods which cause a choking hazard (see list of High Risk Foods). • Tender meat casseroles (approx 1.5cm diced pieces) • Sponge and custard Any foods. Include all foods from “High Risk Foods” list. Normal Page 22 of 31 High Risk Foods Stringy, fibrous texture e.g. pineapple, runner beans, celery, lettuce. Vegetable and fruit skins including beans e.g. broad, baked, soya, black eye peas, grapes. Mixed consistency foods e.g. cereals which do not blend with milk, e.g. muesli, mince with thin gravy, soup with lumps. Crunchy foods e.g. toast, flaky pastry, dry biscuits, crisps. Crumbly items, e.g. bread crusts, pie crusts, crumble, dry biscuits. Hard foods, e.g. boiled and chewy sweets and toffees, nuts and seeds. Husks, e.g. sweetcorn and granary bread. Page 23 of 31 Appendix 9 The „Malnutrition Universal Screening Tool‟ („MUST‟) is reproduced here with the kind permission of BAPEN (British Association for Parenteral and Enteral Nutrition). For further information on „MUST‟ see www.bapen.org.uk Page 24 of 31 Page 25 of 31 Page 26 of 31 Page 27 of 31 Page 28 of 31 Page 29 of 31 Appendix 10 Page 30 of 31 Page 31 of 31