Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Mental disorder wikipedia , lookup
Autism therapies wikipedia , lookup
Deinstitutionalisation wikipedia , lookup
Dissociative identity disorder wikipedia , lookup
History of psychiatric institutions wikipedia , lookup
Pyotr Gannushkin wikipedia , lookup
Emergency psychiatry wikipedia , lookup
Mental health professional wikipedia , lookup
Causes of mental disorders wikipedia , lookup
Autism spectrum wikipedia , lookup
History of psychiatry wikipedia , lookup
Diagnostic and Statistical Manual of Mental Disorders wikipedia , lookup
Controversy surrounding psychiatry wikipedia , lookup
Classification of mental disorders wikipedia , lookup
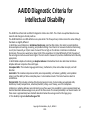
Intellectual disability wikipedia , lookup
History of mental disorders wikipedia , lookup
Asperger syndrome wikipedia , lookup
“MR/DD: Welcome To My World” Dr. Robb Weiss, Psy. D., BCBA-D Chief Psychologist Director Behavioral Health Services San Angelo State Supported Living Center [email protected] Texas Psychological Association 2015 Annual Convention The Future of Psychology Practice in the Era of Health Care Reform Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 2 Saturday 1:00PM-4:00PM 3 hours PD Workshop El Rincon MR/DD: Welcome To My World (W21) This presentation will provide an overview of many aspects of service delivery to individuals diagnosed with intellectual/developmental disabilities. It is an overview of practical psychological/behavioral core concepts, definitions, terms, and resources in the field of ID/DD. It reviews historical information, legal precedent, legislative issues, conceptual information, clinical aspects of assessment, diagnosis, treatment, standards and guidelines, continuum of care, dual diagnosis, relevant organizations, evolution of necessary credentials and knowledge base for working in the field, quality assurance/data collection, policy/regulatory standards, and competencies. Attendees will: Learn fundamental theory and practice in the field of ID/DD Learn to apply concepts in the field of ID/DD Develop specific skills, competencies, and points of view needed by professionals in the field of ID/DD Presenter(s): Robb Weiss, Psy.D., BCBA-D Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 3 Bio Dr. Robb Weiss, Psy. D., BCBA-D is currently the Chief Psychologist and Director Behavioral Health Services at the San Angelo State Supported Living Center in Carlsbad, Texas. He was previously the Chief of Psychology at Central State Hospital (CSH) in Milledgeville, Georgia. It was the largest mental health facility in the state system. In addition, he was the Coordinator of Psychology of the Developmental Disabilities Division and Coordinator of Psychology of Psychiatric Treatment at CSH. He began employment at CSH 07/01/03. He has an extensive curriculum vitae dating back to 1977. He is licensed to practice in Tennessee, Kentucky, Mississippi, Florida, Georgia, and Texas. He is a Board Certified Behavior Analyst-Doctoral Designation (BCBA-D). He graduated from Nova Southeastern University (then called Nova University) with his Doctor of Psychology degree 02/23/87. He bypassed the M.S. in Clinical Psychology degree at Mississippi State University. He has a triple major in his undergraduate studies at the University of South Florida e.g. microbiology, chemistry, and psychology. He obtained an Associate of Arts degree in pre-medical science from Miami Dade Community College (then called Miami Dade Junior College). He is a member of the American Psychological Association, the Texas Psychological Association, and the Psychological Association of Greater West Texas. He is a past member of the following High IQ organizations: ISPE (International Society of Philosophical Enquiry) 99th Percentile, Intertel 99th Percentile, and is a current member of the TNS (Triple Nine Society) 99.9th Percentile. His areas of interest are in Geropsychology and he is credited in a nationwide video and accompanying textbook on providing group therapy in Nursing Homes; and in the field of Intellectual Disabilities/Developmental Disabilities (ID/DD) previously referred to as MR/DD. He is a certified suicide risk assessor with the national QPR organization. He has presented at both the local chapter of the Psychological Association of Greater West Texas, and at the Texas Psychological Association annual convention on “MR/DD: Welcome To My World”. In addition, he has presented at the national level at the Association of Professional Developmental Disabilities Administrators (APDDA) on “Issues Affecting Behavioral Interventions”, and is its’ Approved Continuing Education Coordinator (ACE) for the Behavior Analyst Certification Board (BACB). He is an adjunct professor of psychology at Angelo State University. Finally, he is certified to perform Forensic Competency Evaluations. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 4 Purpose The purpose of the presentation is to provide an “overview” of many aspects of service delivery to individuals diagnosed with intellectual/developmental disabilities. It is an “overview” of practical psychological/behavioral core concepts, definitions, terms, and resources in the field of ID/DD. It is intended for an audience of professionals already in the field of ID/DD and/or those who desire increased competence. It constitutes specialized knowledge for professionals and students and/or refresher for those already in the field. The presentation is a work in progress constantly being updated/revised with new information. It reviews historical information, legal precedent, legislative issues, policy, standards, regulations, conceptual information, clinical aspects of assessment, diagnosis, treatment, standards and guidelines, continuum of care, dual diagnosis, relevant organizations, evolution of necessary credentials and knowledge base for working in the field, quality assurance/data collection, policy/regulatory standards, and competencies. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 5 An Overview of Practical Psychological/Behavioral Core Concepts, Definitions, Terms, and Resources in the field of ID/DD Audience: professionals/students currently in the field of ID/DD who desire a refresher Audience: professionals/students who desire increased competence/specialized knowledge in the field of ID/DD Presentation is a work in progress Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 6 Anachronism Mental Retardation no longer exists Intellectual Disability is the current terminology Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 7 MR Versus ID The construct of intellectual disability (ID) belongs within the general construct of disability that has evolved over the last 2 decades to emphasize an ecological perspective that focuses on the interaction of the person with his or her environment and the recognition that the systematic application of individualized supports can enhance human functioning. The importance of this evolutionary change is that ID is no longer considered entirely an absolute, invariant trait of the person e.g. Mental Retardation, but is a state of functioning. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 8 “You know that you know” “You know that you don’t know” “You don’t know that you know” “You don’t know that you don’t know” -- Albert Einstein Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 9 Insanity “There is nothing that is a more certain sign of insanity than to do the same thing over and over and expect the results to be different.” Albert Einstein Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 10 Faking “Stupid” You can fake “stupid” but you can’t fake “smart” Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 11 Communication “Cannot not communicate”-double negative “Nobody doesn’t like Sara Lee” Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 12 Happy to Welcome……………………... The San Angelo Odyssey By Dr. Robb Weiss, Chief Psychologist 10/10/2012 • • • • • Enlightener Article The largest state mental hospital in Georgia, at one time the largest in the United States, is in the process of closing down after 200 years of existence. I was employed there for the past 7 years as the Coordinator of Developmental Disabilities, Coordinator of Psychiatric Services, and the Chief of Psychology. And so, I found myself in the unsavory position of needing to find new employment. So I buy a 40’ motorhome and hook my car to the back of it. Both my wife and son are each driving a huge U Haul with a car on the back. So the caravan cuts across 5 states in a never-ending nightmare of scenarios, beginning with the motorhome breaking down before we ever leave the state of Georgia, followed by unbelievable scenarios involving having to turn around 58 feet of motorhome-car “train” in the most unbelievable places, and ending with another nightmare scenario even as we enter San Angelo itself. I had only heard of Texas through the TV show Dallas, so I knew for certain that I would meet J.R. Ewing, see the South Fork ranch, and see the glimmering skyscrapers. Well, traveling through Dallas, I thought we would all die on the highway and never quite did see JR or the skyscrapers. From Abilene to San Angelo, I was absolutely dumbstruck by the epic and panoramic view of land like I have never seen before, having grown up in New York and Miami Beach. Suddenly I see the perimeter of a city not unlike the Emerald City in the Land of Oz, in the middle of nowhere. So here we land in San Angelo, Texas, aka “nirvana” to buy the home of our dreams that we first saw on the Internet when we were learning about this place called San Angelo. I’ve found the most incredible bunch of people at this new (to me!) San Angelo State Supported Living Center that I have ever known in my life. Now I’ve gotten my 6th state license that enables me to practice in Texas! I’m truly home now! How’s that for an introduction to your new Chief Psychologist! Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 13 A Little History • • • • • • • SANATORIUM, TEXAS. Sanatorium is in Tom Green County sixteen miles northwest of San Angelo on U.S. Highway 87. It was never an incorporated town, instead, it was a relatively selfsufficient tuberculosis sanatorium. The postmark "Sanatorium, Texas" began with the opening of a post office on the campus in 1919 and disappeared on October 7, 1965, when the post office closed. During the first decade of the twentieth century more than 4,000 deaths a year in Texas were attributed to pulmonary tuberculosis. In 1909 the Texas Senate passed a bill creating a TB colony, but it was defeated in the House. In 1911 both houses passed a bill creating two colonies-one for advanced and one for early cases-dedicated to the treatment and education of people infected with TB. Although plans for the former were abandoned, 330 acres was purchased near Carlsbad for the location of the Anti-Tuberculosis Colony No. 1. The first institution of its kind in Texas, the colony provided the isolation to calm the fears of the public, as well as rest and clean air, the only known cure for TB sufferers. Admission was restricted to patients between the ages of six and sixty for a period not to exceed six months. The fifty-seven-bed facility opened with a barbecue and celebration on July 4, 1912. Bascom Lynn, who commuted from San Angelo, was the first superintendent. In 1913 the facility was renamed the State Tuberculosis Sanatorium, and on January 1, 1914, Governor Oscar B. Colquitt appointed Joseph B. McKnight resident superintendent. Under McKnight's leadership the sanatorium expanded for the next thirty-five years. Attracting employees was difficult because of the fear of TB, low wages, and geographic isolation, therefore, the Sanatorium School for Nurses in Texas was organized in 1915 to train the needed staff. The two-year training focused on TB treatment, and nearly all the students were recovering TB patients. The first class of four graduated in 1917 with a R.T.N. degree (registered tuberculosis nurse). In 1920 administration of the sanatorium passed from the Anti-Tuberculosis Commission to the Board of Control. By the 1930s the facility had treated more than 13,000 patients. From the original four buildings constructed at a cost of $10,000, the facility had grown to thirty-five buildings valued at $1.5 million. In 1930 there were thirteen buildings with 662 patient beds, including 162 beds in the children's Preventorium. The grounds had been expanded to nearly 1,000 acres and included a post office, library, barber shop, dairy, hog farm, butcher shop, bakery, power plant, laundry, printing press with its own newspaper (the Chaser), four water wells, and a school for the children. There were also church services and organized meetings for the Masons, Order of the Eastern Star, bridge club, sewing club, and stamp collectors' club. The complex had grown into a virtually independent community known as Sanatorium. By 1949 Sanatorium had grown to 970 beds with 300 patients on the waiting list. McKnight continued to propose expansions, including a new seventy-five bed dormitory, more employee living quarters, and a twenty-five bed surgery unit to supplement the existing surgical building constructed in 1947–48. Raymond F. Corpe, who was on loan from the United States Public Health Service, had begun to perform thoraco-plastic operations. The 1950s brought dramatic change to the institution. McKnight, who had become synonymous with the battle against TB, retired in 1950. On June 2, 1951, the Texas legislature renamed the institution the McKnight State Sanatorium. The ancillary operations such as the dairy, hog farm, and the Preventorium were systematically closed during the decade. The new superintendent, Dr. Allison, successfully removed the age-limit restrictions and the ban on readmission. But the biggest change was a result of the changing TB treatment. The old treatments, including bed rest and phrenic nerve paralysis, were increasingly replaced by the thoracic surgery program and such drugs as streptomycin and capreomycin. As a result the institution was renamed the McKnight State Tuberculosis Hospital in 1955. The length of stay was reduced from 372 days in 1960 to 311 days in 1961, 254 days in 1962, and 204 days in 1963. In the 1963–64 fiscal year the operating expenses of the hospital totaled $1,417,000. The 290 employees cared for a average of 388 patients at an average patient-per-day cost of $9.98. Changes continued in the 1960s. The nursing school, renamed the State Tuberculosis School of Nursing in 1938, closed in 1961 after graduating 501 nurses. The number of TB beds was reduced to 550 and the length of treatment continued to decline due to new drugs and surgery techniques. Staff now numbered around 100, including a chief thoracic surgeon, five resident physicians, and administrative personnel. After treating approximately 50,000 adult and 5,000 juvenile patients, the McKnight State Tuberculosis Hospital was converted to the San Angelo State School in September 1969. Medical techniques and drugs were now successful in more than 90 percent of TB cases, making Sanatorium and other TB institutions superfluous. The mission of the new institution was to serve the needs of mentally retarded men and women. BIBLIOGRAPHY: San Angelo Standard Times, October 7, 1965. John C. Henderson Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 14 Values The field of ID/DD is laden with values, both individual and cultural. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 15 • • • • • • • • • • • • • • • • • Human Needs Quality of Life/Happiness Addressing each individual’s needs may result in a reduction of challenging behaviors Acceptance, the need for approval Curiosity, the need to learn Eating, the need for food Family, the need for family bonding Honor, the need to behave according to a moral code Idealism, the need to improve society Independence, the need for self-reliance Order, the need for orderliness Physical activity, the need for muscle exercise Power, the need for influence Romance, the need for sex Saving, the need to collect Social Contact, the need for peer companionship Status, the need be an important person Tranquility, the need for safety Vengeance, the need to get even with those who frustrate or offend Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 16 Value-Based Happiness Pay less attention to people’s deficiencies and greater attention to their happiness. Help people with ID experience the activities they most value. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 17 DOJ Settlement Agreement The living centers came under fire in 2008 after reports of a "fight club" at the Corpus Christi facility. Since then, independent monitors under the supervision of a federal judge have visited the Texas centers twice a year. They evaluated the operations against 171 standards of care. Texas has not closed any of its large state-run facilities for people with disabilities since 1995. Texas has more living centers and more residents living in them than any other state. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 18 Sunset Advisory Committee • Call to close 5 SSLCs and Austin State Supported Living Center • Implications • Legislation is dead • Possible implications with DOJ as we are not closing institutions that have been judged to be inadequate for providing services • Not under CRIPA Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 19 Transformation to Recovery • “Patients, consumers, and clients….oh my!” • New Civil Rights Movement • Yale University model Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 20 There is no excuse • There is no excuse……… • Vulnerable population Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 21 Professional Background Active 6 state licenses-TN/KY/MS/FL/GA/TX Former member-Intertel-90th percentile IQ Former member-International Society for Philosophic Enquiry (ISPE)-90th percentile IQ Current member-Triple Nine Society (999)-99.9th percentile IQ Professional background-Mental Health & ID/DD Areas of interest-Geropsychology and ID/DD Doctor of Psychology-Psy. D. Board Certified Behavior Analyst-Doctoral Designation (BCBA-D) Behavior Analyst Certification Board (BACB) Approved Continuing Education (ACE) Coordinator for the Association of Professional Developmental Disabilities Administrators (APDDA) 2013 Certified Risk Assessor-QPR Institute-Eastern Washington University Member American Psychological Association (APA) Member Texas Psychological Association (TPA) Member Psychological Association Greater West Texas (PAGWT) Presentations: “MR/DD: Welcome To My World”-PAGWT (2012) “MR/DD: Welcome To My World”-TPA (2013) “MR/DD: Welcome To My World”-TPA (2015) “Issues Affecting Behavioral Interventions”-Annual Habilitation Therapies Conference (2015) “Issues Affecting Behavioral Interventions”-APDDA (2014) “Cultural Diversity: Judaism”-PAGWT (2014) Adjunct Professor-Angelo State University- Specialty Course-M.S. Counseling Program- “ID/DD: Theory and Practice” (Fall Semester 2014) Adjunct Professor-Angelo State University- Specialty Course-M.S. Counseling Program- “Applied Behavioral Analysis” (Fall Semester 2015) Credentialed to perform Forensic Competency Evaluations Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 22 Resume • College 1970-1987 • Doctor of Psychology-Psy. D. granted 02/23/1987 • South Florida School of Professional Psychology • Florida School of Professional Psychology • Nova University (Nova Southeastern University)-37th largest private university-APA approved Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 23 Nova Atlanta Alumni Association “Spotlight” • • Autobiographical profile http://novaatlantaalumni.blogspot.com/search?updated-max=2007-06-19T16%3A43%3A0005%3A00&max-results=7 NOVA ATLANTA ALUMNI SPOTLIGHT Dr. Robb Weiss, Psy. D. is the Chief of Psychology at Central State Hospital (CSH) in Milledgeville, Georgia. It is the largest mental health facility in the state system. He is also the Coordinator of Psychology of the Developmental Disabilities Division and Coordinator of Psychology of Psychiatric Treatment at CSH. He began employment at CSH 07/01/03. He has an extensive curriculum vitae dating back to 1977. He is licensed to practice in Tennessee, Kentucky, Mississippi, Florida, and Georgia. He graduated from Nova Southeastern University (then called Nova University) with his Doctor of Psychology degree on 02/23/87. He bypassed the M.S. in Clinical Psychology degree at Mississippi State University. He has a triple major in his undergraduate studies at the University of South Florida e.g. microbiology, chemistry, and psychology. He obtained an Associate of Arts degree in pre-medical science from Miami Dade Community College (then called Miami Dade Junior College). He is a member of the American Psychological Association and the Georgia Psychological Association. He is a member of the following High IQ organizations: ISPE (International Society of Philosophical Enquiry) 99th Percentile, Intertel 99th Percentile, and the TNS (Triple Nine Society) 99.9th Percentile. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 24 Definitions • • • • • • • • • • • • ICF/ID Intermediate Care Facility for people with Intellectual Disabilities. These facilities are governed by Federal and State "tags" and monitored by various surveying organizations. For example, in Texas, DADS or The Department of Aging and Disability Services governs the ICF/ID settings. QIDP A person holding at least a Bachelor's Degree in the Human Service Field. The QIDP stands for Qualified Intellectual Disabilities Professional and must have a minimum of one years experience directly working with people who have developmental disabilities. LVN LVN is a Licensed Vocational Nurse. ICF's require many task to be completed by an LVN. For example, an LVN is required to initial dose new medications or take physician orders. Note: There is an alternative to the LVN known as an LPN in some states. This stands for Licensed Practical Nurse and he or she may complete all the task of an LVN. Some states such as Texas have implemented requirements that an R.N. (Registered Nurse) now function in the capacity of the nurse for the ICF/ID. Immediate and Serious Threats Still known among providers as "IJ" or "Immediate Jeopardy" an Immediate and Serious Threat requires prompt action by the facility in question. This is serious problem within an ICF that could result in the ICF's license being revoked. These are initiated in most states by State Surveyors and generally surveyors will not leave the ICF during an Immediate and Serious Threat without a plan and correction in place. If the surveyor does leave the facility before the Immediate and Serious Threat has been resolved, or at least on its way to being resolved, then surveyors generally recommend a 23 Day Termination. 23 Day Termination In many views a 23 Day Termination is as dangerous as an Immediate and Serious Threat. The facility is placed on a time period of 23 days to correct a problem viewed by the state as highly significant and the facility must show progress toward correcting the problem. Because most facilities take action once they have been notified of an Immediate and Serious Threat, the 23 Day Terminations are not usually issued, instead the 90 Day Termination is issued. 90 Day Termination (2567) Most of the time the facility has had a serious issue or Immediate and Serious Threat that has been temporarily fixed or a suitable plan has been put in place while surveyors are on-site. However, the facility still must show significant progress within the time period allowed or there could be a termination of a license just as is found with the 23 Day Termination. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 25 Definitions • • • • • • • • • • • • IDR An IDR is an Informal Dispute Resolution. An IDR is completed when the facility disagrees strongly with a cited deficient practice or a set of cited deficient practice tags. In Texas the surveyor on-site should give the provider information about the IDR process at the exit. POC POC stands for Plan of Correction. Once a survey or state complaint visit is complete, it is not unusual for deficient practices to be cited. Once those cited tags are received by the facility, the facility is required to submit a Plan of Correction and complete that plan of correction within an allotted time frame. LON LON means Level of Need. A LON determines how much money a facility receives to care for an individual. LON changes for less money are typically easier and require less paperwork than an LON for an increase. A facility is required to provide all proof that a person now requires more care and therefore needs a LON change to the state. Annual Staffing An Annual Staffing meeting is required at least once a year for individuals served in an ICF/ID setting. The meeting generally reviews past IPPs, sets up an IPP for the next year, reviews medical conditions, Living Options, and other requirements as outlined by the state and federal regulations. IPP Individual Program Plans are the results of Annual Staffings and other Interim Staffing meetings. An IPP outlines how in the coming year, generally, a facility proposes to assist an individual served in gaining the most independence that he or she can. An IPP is a federal requirements and is done in all states with ICF/ID settings. Data implementation Data or goals are terms used sometimes interchangeable for the documentation taken to prove that an IPP has been implemented. Different facilities use different programs, forms, or word processor programs to ensure they have proof that data has been implemented for individuals served in the facility. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 26 2015 The Olmstead Act • • • • • Originated in Georgia Central State Hospital Milledgeville, Georgia-”Pretty Woman” “Here Comes Honey Boo Boo”-McIntyre, GA Under Title II of the Americans with Disabilities Act, “unnecessary institutional segregation of the disabled constitutes discrimination per se, which cannot be justified by a lack of funding.” Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 27 The Olmstead Act 1. What Olmstead is Not 2. How Olmstead is misused 3. The Olmstead decision supports facility-based (institutional care) for those individuals whose severe impairments require the close care found in such settings 4. Olmstead encourages a continuum of service options for disabled persons-home, community and institutional 5. People with mental retardation, especially individuals with severe and profound mental retardation, and their families have vastly different support requirements than those with physical disabilities. As families age, their abilities to be the primary care givers (and fiscal intermediaries) will also change. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 28 • • • • • “intentional communities” for DD population vs. CMS definitions and rules In an era when 50 percent of Americans don’t even know their own neighbors, living in a small home can be especially isolating for a person with I/DD. Micki Edelsohn, the founder of the Delaware non-profit Homes For Life, built her first group home in 1989 for four men, including her son Robert, 42, who has an intellectual disability due to a birth injury. Since then, she has established 25 similar homes all over the state, as well as several completely integrated apartments that meet the most stringent interpretation of the CMS final rule. Her verdict? “Community integration is a myth,” she told me. “My homes are in nice neighborhoods—do you think the neighbors are asking the residents over for barbecues or to go to the movies? Of course not. There has been no real interaction between the neighbors and the people living in the homes besides the occasional wave.” After building group homes for a quarter of a century, Edelsohn told me, “Before I die, my son will be in an intentional community.” Many parents and providers I spoke to at congregate settings across the country prefer the term intentional community, which likens a place like Misericordia to any planned residential development in which people choose to live together because of certain shared characteristics. That sense of common ground is what’s often lacking when individuals with I/DD live in integrated housing, surrounded by neighbors who don’t understand them. http://www.theatlantic.com/health/archive/2015/05/who-decides-where-autistic-adults-live/393455/ Public/Community antipathy against MR Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 29 Less Restrictive Setting Perhaps it was this population that Supreme Court Justice Ruth Bader Ginsburg was worried about when she carefully crafted her opinion in the 1999 Olmstead case to make it clear that community inclusion might not be right for everyone. Such integrated settings, she wrote, should only be required “when the State’s treatment professionals have determined that community placement is appropriate” and “the transfer from institutional care to a less restrictive setting is not opposed by the affected individual.” In other words, forcing developmentally disabled individuals into dispersed community settings that don’t meet their needs is as much a violation of Olmstead as forcing them into institutions. “Even when living in their own apartments, people can be dehumanized through words or actions and involuntarily segregated by support staff. Physical locations don’t do this, people do.” It would appear that living in “the community” is more restrictive than living in the institutional setting. http://www.theatlantic.com/health/archive/2015/05/who-decides-whereautistic-adults-live/393455/ Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 30 Intentional Community • Planned residential development in which people choose to live together because of certain shared characteristics. • That sense of common ground is what is often lacking when individuals with I/DD live in integrated housing, surrounded by neighbors who don’t understand them. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 31 Choice-Making Among Medicaid HCBS and ICF/MR Recipients in Six States K. Charlie Lakin, Robert Doljanac, Soo-Yong Byun, Roger Stancliffe, Sarah Taub, Giuseppina Chiri, and David Felce (2008) Choice-Making Among Medicaid HCBS and ICF/MR Recipients in Six States. American Journal on Mental Retardation: September 2008, Vol. 113, No. 5, pp. 325-342. Choice in everyday decisions and in support-related decisions was addressed among 2,398 adults with intellectual and developmental disabilities receiving Medicaid Home and Community Based Services (HCBS) and Intermediate Care Facility (ICF/MR) services and living in nonfamily settings in six states. Everyday choice in daily life and in support-related choice was considerably higher on average for HCBS than for ICF/MR recipients, but after controlling for level of intellectual disability, medical care needs, mobility, behavioral and psychiatric conditions, and self-reporting, we found that choice was more strongly associated with living in a congregate setting than whether that setting was HCBS- or ICF/MR-financed. Marked differences in choice were also evident between states. The issue of increased choice, whether in a congregate setting or in a smaller, integrated setting may be one benefit of a cost-benefit analysis-not a reason to rule out congregate settings all together. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 32 Evolution of concept of “disability” • • • • • Historically: Medical model e.g. individual is damaged Currently: Socioecological model e.g. interface between the individual and the supports in the environment Implications are far reaching for transforming psychological practice (from decelerating undesirable target behaviors to modifying environments that fail to foster growth and development and providing a system of supports to ensure success for the individual), policy, society, research, funding, collaboration amongst disciplines, etc. Disabilities have been far too long “marginalized” e.g. “redheaded stepchild” The clinical definition of intellectual disability is predominantly a social construct and does not represent a qualitative distinction between those people who meet the diagnostic criteria and those who do not (many people with IQs below 70 will not warrant a formal diagnosis of intellectual disability because their adaptive behavior is sufficient for them to cope with day-today demands of life (there is very little functional difference between someone with an IQ score of 70 and someone with an IQ score of 75) Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 33 Intellectual Disabilities What are intellectual disabilities? According to the American Association on Intellectual and Developmental Disabilities, intellectual disabilities are characterized by significant limitations in both intellectual functioning (reasoning, learning, problem solving) and in adaptive behavior, which covers a range of everyday social and practical skills. This type of disability originates before the age of 18. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 34 Intellectual Disabilities What are the effects of intellectual disabilities? While the effects and severity of these conditions can vary widely, people with developmental disabilities have problems with major life activities such as language, mobility, learning, self-help, and independent living. Intellectual disabilities in these individuals are often not identified until they enter school. Many people with intellectual disabilities grow up to lead independent lives. The remaining minority of people with intellectual disabilities, those with IQs under 50, have significant limitations in functioning. With early intervention, a functional education, and appropriate supports as an adult, individuals with intellectual disabilities can lead satisfying lives. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 35 Intellectual Disabilities What are the causes of intellectual disabilities? Intellectual disabilities can be caused by any condition that impairs development of the brain before birth, during birth, or in the childhood years. Hundreds of causes of intellectual disabilities have been identified. However, for approximately one-third of those affected, the cause of their disability remains unknown. Causes of intellectual disabilities include: • Pregnancy/delivery problems (drugs, malnutrition, illness, prematurity) • Early childhood diseases and accidents • Exposure to toxins and other environmental health hazards • Genetic anomalies and disorders Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 36 Intellectual Disabilities Can intellectual disabilities be prevented? Significant advances in research over the past 35 years have prevented many intellectual disabilities. For example, every year in the United States, more than 10,000 cases of intellectual disabilities are prevented through newborn screening and dietary treatment, thyroid hormone replacement therapy, use of anti-Rh immune globulin to prevent Rh disease and severe jaundice in newborn infants, and Hib and measles vaccines. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 37 Mental Retardation: What it is not!! • -not something you have or are (blue eyes, short, etc.) • -not a medical or mental disorder Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 38 Mental Retardation • -refers to a particular state of functioning (not an inherent quality) that begins in childhood and in which limitations in intelligence coexist with related limitations in adaptive skills • -describes the “fit” between the capabilities of the individual and the structure and expectations of the individual’s personal and social environment Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 39 Mental Retardation • A condition that affects a person’s ability to learn and function independently • Individuals with mental retardation learn more slowly and with greater difficulty • Individuals with mental retardation can learn, but the rate at which they learn is slower • It is possible there are some things a person with mental retardation may not be able to learn, such as complex problem-solving skills Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 40 Mental Retardation Diagnosed by assessing: person’s ability to learn, think, solve problems, and make sense of the world e.g. intellectual functioning (IQ) Whether the person has the skills needed to take care of him or herself to live independently e.g. adaptive functioning (rating scales comparing what an individual can do with what other individuals of his or her age can typically do Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 41 • • • • • • • • • • • • • • • Mental Retardation: A Clinical Overview Background Historical context Current practices Phenomenology IQ & adaptive behavior Developmental level Aberrant behaviors Pathophysiology Gene X Environment etiologies Abnormal CNS development Learning & environment Neuropsychiatric impairment Treatment Psychosocial/Behavioral Pharmacologic Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 42 Diagnostic criteria for Mental Retardation • Psychometric-Psychological testing before age 18 • Anecdotal-Information that supports deficits before age 18 • DSM-IV-TR • Diagnosis “typically” does not change after age 18 unless based on erroneous diagnosis prior to age 18, however, the diagnosis is fluid. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 43 Diagnosing MR The diagnosis of Mental Retardation requires that the “onset” of the disorder be before age 18 years (DSM-IV-TR). It is not required that the “diagnosis” be made prior to age 18 years. The diagnosis can be made in adulthood if the clinical presentation meets relevant diagnostic criteria. The level of severity may be altered after age 18 though the original level of severity was provided based on information obtained about functioning levels before age 18. If there is sufficient documentation indicating that the onset of significantly sub-average general intellectual functioning was accompanied by significant limitations in adaptive functioning in at least two skill areas prior to age 18 years, then the diagnosis of Mental Retardation can be made (even later in adulthood). This is not a new concept. We can give a MR diagnosis to an adult if there is solid historical evidence of onset of mental retardation prior to age 18, even if the diagnosis was not made prior to age 18. The fact that an MR diagnosis was not made prior to age 18, does not mean that we have missed our opportunity to diagnose that condition and thus facilitate delivery of appropriate services/supports. Any further argument would center around what constitutes “strong historical evidence and sufficient documentation” that would enable us to give a MR diagnosis in adulthood. In the absence of good records review developmental milestones, grades in school, performance at work, anecdotal information provided by third parties and the person him/herself, clinical judgment about IQ/development/ID (IQ scores are quite stable and have predictive validity, interventions can make a difference. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 44 AAIDD The American Association on Intellectual and Developmental Disabilities Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 45 Comparing the APA and the AAIDD Diagnostic Criteria for ID • The APA diagnostic criteria is commonly used to diagnose intellectual disability (ID, formerly mental retardation). As such, the focus leans toward identifying limitations. The AAIDD definition is more often used to develop a rehabilitation plan. It leans toward identifying abilities that facilitate rehabilitation. Diagnosis and rehabilitation are two different but related agendas. The APA definition serves to identify limitations that facilitate diagnosis. In contrast, the AAIDD definition highlights abilities that facilitate rehabilitation. • The APA diagnostic criteria are usually relied upon for that purpose; i.e., diagnosis. In contrast, the AAIDD is relied upon to develop a rehabilitation plan. This plan is called an individualized support plan, or ISP. The ISP identifies the optimal level of support for the person with an ID. This is accomplished by the identifying strengths and functional abilities that can offset deficits. Although limited intellectual and adaptive functioning identify an ID, it is equally important to identify strengths and abilities. Knowledge of these abilities helps to develop the ISP to maximize independent functioning. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 46 AAIDD Diagnostic Criteria for intellectual Disability The AAIDD has refined and modified ID diagnostic criteria since 1921. The criteria are updated based on new research and changes in clinical practices. The AAIDD definition and APA definition are quite similar. The three primary criteria remain the same although the labels are slightly different: 1. AAIDD also uses limitations in intellectual functioning. Like the APA criteria, this refers to mental abilities. Some examples are learning, reasoning, and problem solving. One criterion to measure intellectual functioning is an IQ test. Generally, an IQ test score of around 70 or as high as 75 indicates a limitation in intellectual functioning. These scores would occur about 2.5% of the population. Or stated differently, 97.5% of people of the same age and culture would score higher. The tests used to measure IQ must be standardized and culturally appropriate. 2. AAIDD labels adaptive functioning as adaptive behavior. Standardized tests also determine limitations. Adaptive behavior comprises three skill types. Conceptual skills: This includes language and literacy; mathematics; time and number concepts; and selfdirection. Social skills: This includes interpersonal skills; social responsibility; self-esteem; gullibility; social problem solving; and the ability to follow rules/obey laws. It also includes naïveté. This lack of wariness leads to victimization. Practical skills: This includes activities of daily living (personal care). It also includes occupational skills, healthcare, travel/transportation, schedules/routines, safety, use of money, use of the telephone. Limitations in adaptive behavior are indicated in one of two ways. One possibility is a score approximately two standard deviations below average in any one of the three areas. The second possibility is an overall score in all three areas is approximately two standard deviations below the average score for that age group. 3. This disability originates before the age of 18. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 47 Significant Intellectual Disability A significant intellectual disability has been and continues to be defined as a finding of sub-average intellectual functioning based on a score two standard deviations or more below the mean (IQ<70) on an accepted standardized intelligence test (Wechsler, Stanford-Binet, etc.). “Significant” is two standard deviations from the mean, so that is a consistent standard that will not vary from person to person. The Stanford-Binet provides a lower basal for diagnosing greater severity levels of ID. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 48 • • • • • • • Severity of Mental Retardation Prior to DSM 5 based on IQ level As of DSM 5 based on level of adaptive supports Mild-(50-55)-70 Moderate-(35-40)-(50-55) Severe-(20-25)-(35-40) Profound-below 20 or 25 Don’t confuse this with V62.89 Borderline Intellectual Functioning-IQ in the 71-84 range [coded on Axis II] Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 49 Developmental Disabilities What are developmental disabilities? Developmental disabilities encompass a broad range of conditions that result from cognitive and/or physical impairments. They are identified before the age of 22, and usually last throughout a person’s lifetime. These disabilities include intellectual disabilities, autism spectrum disorders, Down syndrome, language and learning disorders, cerebral palsy, vision impairment, and hearing loss. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 50 Developmental Disabilities How prevalent are developmental disabilities? Developmental disabilities occur in people of all racial, ethnic, educational, and socioeconomic backgrounds. According to the National Association of Councils on Developmental Disabilities, 5.4 million Americans have developmental disabilities. Approximately 17 percent of children under the age of 18 are affected. The most common developmental disorder is intellectual disability. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 51 Developmental Disabilities What are the most common developmental disabilities? The most common developmental disorder is intellectual disability. According to the Centers for Disease Control and Prevention, more than one out of every 100 school children in the United States has some form of intellectual disability. Cerebral palsy is the second most common developmental disorder, followed by autism spectrum disorders. According to First Signs, Inc., other developmental disorders include: Attention-Deficit/ Hyperactivity Disorder (ADHD) Angelman Syndrome Bipolar Disorder Central Auditory Processing Disorder (CAPD) Down Syndrome Expressive Language Disorder Fragile X Syndrome IsoDicentric 15 Landau-Kleffner Syndrome Learning Disabilities (LD) Neural Tube Defects Phenylketonuria (PKU) Prader-Willi Syndrome •Seizure Disorders •Tourette Syndrome Traumatic Brain Injury (TBI) Williams Syndrome Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 52 Developmental Disabilities How are developmental disabilities diagnosed? If you are concerned that a member of your family may have a developmental disability — whether physical or intellectual— contact a respected behavioral healthcare organization and/or healthcare professional. First, the organization should have a qualified professional give your family member standardized intelligence and skills tests. Second, the professional should determine your family member’s strengths and weaknesses in the areas of intellectual and adaptive behavior skills, psychological and emotional considerations, physical health, and environmental factors. Finally, a trained interdisciplinary group of professionals should meet to determine what supports are needed to address each of the areas stated above. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 53 Developmental Disability Developmental Disability means a severe , chronic disability of an individual that: (A) Is attributable to a significant intellectual disability, or any combination of a significant intellectual disability and physical impairments; (B) Is manifested before the individual attains age 22; (C) Is likely to continue indefinitely; (D) Results in substantial functional limitations in three or more of the following areas of major life activities: (i) Self-care; (ii) Receptive and expressive language; (iii) Learning; (iv) Mobility; (v) Self-direction; and (vi) Capacity for independent living; and (E) Reflects the person’s need for a combination and sequence of special, interdisciplinary, or generic services, individualized supports, or other forms of assistance which are of lifelong or extended duration and are individually planned and coordinated. Not a mental disorder Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 54 Autism • CDC estimates half a million children in the US • A brain-based neurobiological disorder caused by abnormalities in the brain that may come with many challenges, but also imparts great gifts • More to do with biology than psychology • Not a mental illness, a result of bad parenting, or a death sentence for fulfilling and productive lives • Most common member of autism spectrum disorders (ASDs)/Pervasive Developmental Disorders (PDD) • Usually diagnosed by age of 3 • Found in every country, every ethnic group, and every socioeconomic class • Diagnosed four times as often in boys than in girls • Early intervention is needed Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 55 Autism WHAT IS AUTISM? Autism is a Spectrum Disorder Autism is a Developmental Diagnosis Characteristics Will Change as the Person Grows Older • Previously coded on Axis I • • • • Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 56 Post Traumatic Stress Disorder (PTSD) in People with Autism • Role of aversives and restraints • May explain newly emerging symptoms • Despite fairly abundant anecdotal evidence, knowledge of the nature, prevalence, and treatment of psychological trauma in the lives of people with severe disabilities is lacking Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 57 Prevalence of Autism Spectrum Disorders • Centers for Disease Control and Prevention • Morbidity and Mortality Weekly Report (MMWR) • Autism and Developmental Disabilities Monitoring (AADM) Network Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 58 Discrete Trial Training (DTT) • Skill Acquisition-Tight stimulus control • Method of providing intervention for individuals diagnosed with Autism • According to Anderson et al. (1996), the discrete trial method has four distinct parts: • (1) the trainer's presentation • (2) the child's response • (3) the consequence • (4) a short pause between the consequence and the next instruction (between interval trials) Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 59 Autism Speaks Autism Speaks funded the largest-ever multinational study of parental age and autism risk. It was found that there was an increased autism risk for children of teen mothers and children whose parents have relatively large gaps between their ages. Additionally, older parents were found to be at a higher risk of having children with autism. While parental age is a risk factor for autism, the study states that it is important to remember that overall, the majority of children born to older or younger parents develop without the illness. Autism Speaks, Science Daily 06/09/2015 Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 60 Debunking myths about autism • ASD is the name for a specific group of behavioural and developmental challenges that affect a child's social behaviour, communication and play. It is caused by rare genetic variants that influence how the brain grows and develops. Since autism is a spectrum disorder, each person's symptoms differ in variety and severity. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 61 Debunking myths about autism • • • • • • • • • • MYTH: There is an autism epidemic. FACT: The prevalence of those diagnosed with ASD has gone up about tenfold since the mid-1980s, but it is important to note the increase is largely associated with changes in the diagnostic criteria and a greater awareness in the medical community of how autism presents at different ages. There is no evidence that there is any environmental factor that might account for the increase in prevalence. MYTH: Vaccines cause ASD. FACT: It is very clear that autism is not caused by vaccines. The initial paper published on this topic has been disproved. This claim has now been recognized as fraudulent and biased by the pursuit of class action lawsuits. In fact, there are several communities where the ingredients that were reported to cause autism have been removed from the vaccine and yet within those communities the diagnosis of autism continues to rise. MYTH: ASD is caused by poor parenting. FACT: This myth comes out of very poor research from the 1950s, which was already being widely refuted by the 1960s. There is absolutely no evidence that poor parenting or poor parent-child relationships cause autism. ASD is caused by genetic factors, possibly combined with environmental factors in utero. MYTH: Only boys can have autism. FACT: The sex ratio in ASD is roughly four boys to every girl. So it is certainly true that girls can have ASD, but they tend to be more severely affected than boys. However, this may be because girls with ASD are not as readily recognized. In fact, some evidence suggests we should be using different diagnostic criteria for girls than for boys to take account of these variations. MYTH: ASD can be cured with diet or other alternative treatments. FACT: We have to be careful here. Whether autism can be "cured" or not is contentious, but there is no question that children with ASD improve the earlier they get the intervention and the more intense that intervention might be. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 62 Debunking myths about autism • • • • • • • • • • MYTH: People with ASD do not feel or like to socialize. FACT: Children with ASD do socialize and feel emotions, but the communication and the expression of those emotions is atypical. Their desire to socialize with people might not be as intense as it is in typically developing children. Nevertheless older children, adolescents and young adults with ASD do enjoy interacting with other children and adolescents and do seek them out. MYTH: ASD gives people savant or genius abilities. FACT: The use of the word "savant" comes from older research suggesting that although there are some people with autism who are non-verbal or have severe cognitive disability, they nevertheless have a fantastic memory, a capacity for drawing, an ability to do elaborate calculations and can read much better than expected. That is certainly true for a tiny minority of people with ASD, but it is better to refer to these as splinter skills rather than "savant" or "genius." The definition of a genius is having an IQ above 120 and, while this is certainly possible for people with ASD, it is much less likely than in the general population MYTH: Autistic children should only attend separate special needs programs. FACT: Children with ASD benefit from interactions with typical children because it improves their social and communication skills and decreases their repetitive play. So the treatment recommendation now is to keep children in the educational mainstream and only withdraw them under exceptional circumstances, for short periods of time. All children with ASD require a special education plan that takes their disability into account. MYTH: You should try to stop an autistic child's repetitive behaviour. FACT: The important issue here is to understand the function of that repetitive behaviour. Sometimes children engage in repetitive behaviour because they are bored, stressed or playing. The key treatment here is to try and modify that repetitive behaviour so that it becomes more developmentally appropriate and more like typical play. In other words, we need to understand why a child engages in repetitive play and then deal with the underlying cause instead of focusing on the behaviour itself. MYTH: Children with autism cannot become independent adults. FACT: The range of outcome possibilities for children with ASD is quite remarkable. Many children with ASD grow up to be adults who live independently, who work, who develop close friendships, even romantic relationships. It is likely that most adults with ASD will always require some kind of support, but this can sometimes be done at a distance. It is also true that there are many individuals with ASD who require full-time, specialized services as adults and those appropriate supports are available through community services. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 63 Discharge versus Transition • Discharge-behavioral criteria • Transition-interface between needs and supports • Continuum of care • Transition planning occurs upon admission • Least restrictive environment [institution may be less restrictive than the group home] Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 64 Intermediate Care Facility for the Mentally Retarded (ICF/MR) ICF/MR Guidelines (Medicaid) ICF/MRs-(incorrect) ICFs/MR-(correct) Think “Attorneys General” rather than “Attorney Generals” • ICF/IID: Intermediate Care Facility for Individuals with Intellectual Disability • • • • Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 65 Outreach • • • • • • • • • • • • Experiencing challenging behaviors at home, school, work site or community-not residential treatment facility Provides a complete set of recommendations to assist families and service providers in decreasing unwanted behaviors and supporting positive behaviors Examples include verbal and physical aggression, elopement, stealing, property destruction, selfinjurious and inappropriate sexual behaviors Founded in best clinical practice and are considerate of personal choice, socially appropriate behavior development, personal growth, and provided agency philosophy Highly specialized teams with behavioral and psychological expertise Observation and assessment in the natural environment Interviews with the individual, teachers, families, service provider staff and other significant parties A review of back and records and medication reviews A treatment package that includes a development of a variety of interventions Presentation of the treatment package to the community team in written and oral formats Maintains regular contact with the team Conducts an onsite follow-up visit Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 66 Intensive Treatment Services • Short-term inpatient treatment to individuals from community settings • Individuals who are experiencing severe behavior problems and are in danger of losing community services • Require adjustments to psychoactive medications in a highly structured setting (not a behavioral holiday-think about the contingencies operating in the residence of origin) • Goal is to stabilize an individual’s behavior/medications and develop treatment recommendations which can be transitioned back to the community setting following the inpatient care • Consider the philosophy, resources and limitations of the community service provider who serves the individual Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 67 System Issues Common System Issues -Not enough funds -Lack of available resources -Staff turnover/shortages -Communication difficulties -Things don’t happen fast enough Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 68 Future of Residential Services • Wolf Wolfensberger • Twenty predictions about the future of residential services in mental retardation-changes imply 1. new model of residential services 2. increasing continuity between residential and non residential services 3. cost-benefit rationales • Will there always be an institution?-I: The impact of epidemiological trends-1. development of nonresidential community services 2. new conceptualizations of residential services 3. increased usage of individual placements 4. provision of specialized group residences 5. decline in incidence of severe and profound retardation • Will there always be an institution?-II: The impact of new service modelsresidential alternatives to institutions- trends-1. development of nonresidential community services 2. new conceptualizations of residential services 3. increased usage of individual placements 4. provision of specialized group residences 5. decline in incidence of severe and profound retardation Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 69 Developmental Disabilities (DD) • Originally not medical but legislative/legal concept • Now defined in functional terms • Autism/Pervasive Developmental Disorder (PDD)/Rett’s Disorder/Asperger’s Disorder [no longer exists in DSM 5] • Coded on Axis I (DSM-IV-TR) Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 70 Axis II Mental Retardation Not a single entity Heterogeneous behavioral syndrome Individualized treatment planning Does not cause….but is the cause of “Normalization principle”-enable people to live in as normal an environment as possible • Not “make them normal” • • • • • • Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 71 Psychiatric Issues • Access to Psychiatric Services -Service providers should have some experience working with individuals with IDD -Service providers should be willing to work with team members on the individual’s behalf to obtain enough information to make accurate diagnosis and assess treatment results -Crisis services are often unavailable due to a lack of experience or understanding of the risks of the IDD population Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 72 Psychiatric Issues • Internal Distress and Overt Behavior -Increase in internal distress likely results in an increase in the intensity and frequency, sometimes duration, of observable challenging behaviors -Regression in coping and impulse control skills -Less inhibited, more difficult to manage behavior -May not understand the symptoms Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 73 Psychiatric Issues • Change in behavior must co-occur with significant changes related to symptoms -Disturbance in sleeping/eating patterns -Report of depression, anxiety, fearfulness -Report of hearing voices or being persecuted -Behavior related to mood or affect (increase in anger, rage, hostility); increase in intensity of the behavior -Other symptoms related to specific diagnostic criteria -The presence of challenging behavior alone is not adequate for diagnosis Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 74 Psychiatric Issues • It is our responsibility to provide the individual and their family with the alternatives and information necessary to make an informed decision on treatment and evaluations for psychiatric issues. Psychiatric services, counseling, and/or behavioral services should be discussed with recommendations based on an assessment by the appropriate treatment provider. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 75 Psychiatric Issues • Issues related to psychiatric services -Ongoing assessment of internal distress (compare affect/mood before and after treatment) -For individuals who may have difficulties describing their experience, ongoing assessment, including behavioral assessment, and consultation with the psychiatrist is helpful to assure the most effective overall treatment -Secondary learning occurs when psychiatric symptoms result in challenging behaviors that are rewarded by the consequences of the behavior. Appropriate behavioral intervention is used to address these challenging behaviors -Increase positive behavior/skills that strengthen the individual’s ability to manage their behavior when experiencing internal distress: coping skills, relaxation skills, assertiveness skills; reporting to staff Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 76 Psychiatric Impairments • Psychiatric impairments rank second, after mobility impairment, in noted secondary disabilities in persons with a developmental disability. The reason behind this phenomenon, it seems, is that people with developmental disabilities are at greater risk due to their physical and cognitive impairments. And due to the nature of their disability, they are more exposed to exploitive, degrading, physically and sexually abusive situations. • Research has shown that people with developmental disabilities are 4-10 times more likely to become victims of crime. Due to their impaired coping and adaptation skills, it is extremely difficult for people with developmental disabilities to effectively cope with trauma, much harder than for the non disabled. • The golden rule taught by the training instructors was “regardless of what sector you are in, when you are working with someone with a developmental disability, you should always consider the possibility that they have a mental health disorder.” It is important to understand the complexities surrounding dual diagnosis, namely: Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 77 Dual Diagnosis/Mental Disorders: Subset with Axis I Psychiatric Disorders Difficulty in diagnosing psychiatric disorders in those with ID/DD (mild/moderate versus severe/profound) [Accurate assessment/accurate diagnosis/accurate treatment] Limited verbal communication, rely on nonverbal communication obtained in natural setting Difficulty correctly labeling emotions/internal states Concrete language/lack of imagination leads clinician to miss significant symptoms Usefulness of interview decreases Recent stressors Sleep/Appetite disturbance Activity level Functioning level Family history of mental illness Rating scales Medical history and physical examination Chart review Direct observations in natural environment Psychological testing Medical evaluations Functional behavioral assessment Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 78 Dual Diagnosis/Mental Disorders: Subset with Axis I Psychiatric Disorders • • • • • • • • • • • • Understanding that many people with developmental disabilities have mental health problems is important for planning treatment, supports, and service provision and can help increase our knowledge about the etiology of these conditions Diagnosing mental health problems in people with developmental disabilities is a complex and challenging process In many ways, the assessment of mental health problems in people with developmental disabilities follows the same principles as the psychiatric assessment of people without developmental disabilities The accuracy of such diagnosis depends on multiple factors intrinsic to both the patient and the assessor Referral pathways are different e.g. very rare for people with developmental disabilities to initiate a mental health referral themselves Usually, they have to rely on family or residential staff to identify the problem, with most common reason for referral being behavioral disturbance Subtle or insidiously developing changes in mood, sleep, or appetite are less likely to be detected Conceptualizing how the presentation might be a synthesis of vulnerability and of precipitating and maintaining factors (biological, psychological, social, and environmental) is a complex task and requires a coordinated multimodal and interdisciplinary approach to assessment In assessing mental health problems in people with developmental disabilities in a comprehensive way, the norm is to gather information from multiple sources Requirement that this process be coordinated and managed by one particular team member who is able to understand and integrate the different strands of information The length of the interview must also be flexible to accommodate people with memory or attention-span problems, and several short sessions may be scheduled The degree of developmental disabilities needs to be considered because people with more severe developmental disabilities are more likely to show atypical signs and symptoms or behavioral problems Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 79 Dual Diagnosis/Mental Disorders: Subset with Axis I Psychiatric Disorders • Definition of Mental Disorder versus normal human emotions e.g. grief/mourning, etc. • Is it Behavioral or Psychiatric-it’s all about behavior • To Medicate or Not to Medicate-behavioral/environmental intervention first/psychoactive medications second • Role/Purpose of Psychiatry-help patients consciously control their brain chemistry through pharmacotherapy and psychotherapy • Approaches to Treating Mental Disorders-teach coping skills/alter environment/teach behaviors that alter brain chemistry • Role of IDT-explore all applicable treatment options, implement via ISP, integrate treatment with psychoactive drugs into ISP, monitor symptoms and outcomes, input into psychiatry clinics • Role of ICF/MR-Active Treatment (acquisition of necessary behaviors, prevent deceleration or regression or loss of functioning) • To diagnose Axis I or not to diagnose Axis I (that is “not” the question)-the issue is the accurate diagnosis (occurs over time and space) Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 80 Mental Health Disorders • People with ID are vulnerable to the same mental health disorders as is everybody else. • Personality disorders and behavior problems, so-called DSM Axis II conditions, are much more prevalent for people with ID versus the general population. • Mental health disorders occur more frequently, last longer, and have more severe consequences for people with ID, and people with a dual diagnosis are underserved. • Posttraumatic Stress Disorder has become a much more frequent diagnosis in both ID and non-ID populations because of the expanding definition of trauma. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 81 Consequences of Dual Diagnosis • Delay personal growth and/or cause significant deterioration in overall adaptive functioning. • Lead to maladaptive social behaviors that cause failure in employment settings. • Cause emotional discomfort and pain. • Create barriers to residential and educational opportunities in community settings. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 82 Diagnostic Guidelines • • • • • • • • • • Establishing a psychiatric diagnosis for a person with developmental disabilities can be particularly difficult, because of certain limitations within the current classification systems Most psychiatric symptoms are described with the use of language-based phenomenology The severity of any cognitive or language deficits is bound to influence the reliability of such diagnoses [DM-ID, modify criteria of existing diagnostic classifications, behavioral correlates of psychiatric symptoms] People with mild developmental disabilities and good verbal skills present similar psychiatric symptoms to those presented by people without developmental disabilities Negative symptoms can be the result of medication, depression, or an understimulating environment Diagnose patterns of behavior, not isolated symptoms Diagnose deteriorations in functioning Side effects from prescribed medications can sometimes mimic or cause psychiatric symptoms; therefore, a medication history, including previous dosing, duration of treatment, effectiveness, and side effects, is always necessary A comprehensive risk assessment estimating the risk to self and/or others, as well as the risk of self-neglect, abuse, and exploitation, should be a routine component of the assessment pathway Do not over diagnose psychiatric disorders [Developmentally appropriate phenomena, such as talking to oneself or imaginary friends should be distinguished from psychotic phenomena, such as auditory hallucinations] Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 83 Abnormal Motives • A need for excessive amounts of attention may instigate or predict persistent conduct problems including challenging behavior. • Although individual with ID receive attention when they behave appropriately, they receive much more attention when they behave inappropriately. • Consequently people who need excessive attention may embrace conduct problems as the only means they have for receiving the amount of attention they desire. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 84 Dual Diagnoses: The Scope of the Challenge Diagnostic Considerations-Examples (not inclusive) -Signs and symptoms of certain psychiatric disorders often present in atypical or unusual ways. System Challenges -Identify and obtain the appropriate psychiatric and psychological services to address the psychiatric disorders. Daily Stressors -Not only contribute but can create psychiatric disorders. A Future Commitment -Need to expand our knowledge about dual diagnosis. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 85 Factors Complicating Psychiatric Diagnoses Barriers to Diagnosis and Treatment 1. Diagnostic overshadowing-overlooking/minimizing signs of mental illness because it is considered less debilitating than mental retardation or because the symptoms of mental illness are attributed to the mental retardation/attribute signs/symptoms to ID Behavioral overshadowing-tendency to identify psychopathology as learned behavior while failing to recognize it is an indicator of mental illness 2. Problems with polypharmacy (medication masking)-sedative effects of certain medications can suppress, or mask, the presence of significant mental health symptoms 3. Communication Deficits 4. Atypical Presentation of Psychiatric Disorders-DM/ID [Episodic presentation-significant mental health symptoms may come and go in an unpredictable manner, and presence of mental disorder may go undetected] 5. Limited life experiences e.g. no spending spree in mania 6. Complications of untreated medical conditions 7. Acquiescence-agreement with all signs/symptoms 8. Imitative or learned behavior-institutional suicidal threats/gestures 9. Lack of behavioral challenges-the good patient 10. Sensory impairments-inability to communicate 11. Division of services-between mental health and mental retardation (no integration of services) 12. Lack of expertise-mental health professionals lack training in mental retardation and vice versa 13. Psychosocial masking-since people with developmental disabilities have limited social experiences, their psychiatric symptoms may be very different than those of the “normal” population, for example, belief that one can drive a car may be mania 14. Cognitive disintegration-cognitive impairment 15. Baseline exaggeration-Onset of psychiatric illness may increase the severity or frequency of chronic maladaptive behavior. This can also influence the diagnosis of mental illness 16. Intellectual Distortion: Due to deficits in abstract thinking, receptive and expressive language skills, emotional symptoms may be difficult to elicit. In fact, emotional symptoms may manifest in behavior. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 86 Factors Complicating Psychiatric Diagnoses Emotional considerations 1. Progressing thru typical developmental milestones, but at a slower pace (treated much younger than chronological age) 2. Limited opportunity to experience and learn from the new challenges 3. Offer an environment that offers age appropriate opportunities (job, home, relationships, self-help responsibilities), while providing developmentally appropriate supports (supervision, coaching, education) 4. Relationship problems Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 87 Factors Complicating Psychiatric Diagnoses Cognitive considerations 1. Expressive Language 2. Receptive Language 3. Short-term memory 4. Long-term retrieval 5. Executive functioning Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 88 Atypical Presentation of Specific Psychiatric Diagnoses • Mood Disorders • Anxiety Disorders-underreported, OCD versus stereotypy, PTSD • Adjustment Disorder • Psychotic Disorders • Personality Disorders • Impulse Control Disorders • Attention Deficit/Hyperactivity Disorder • Sleep Disorders • Dementia Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 89 Medical Contributions to Psychiatric Conditions Common Medical Conditions in Individuals with an Intellectual Disability 1. Gastrointestinal conditions 2. Urological conditions 3. Asthma 4. Sleep apnea 5. Seizures Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 90 Medical Issues and Behavior • Medical issues individuals may have difficulties reporting or describing to staff/nurse/physician: -Headache/Sinus -Acid Reflux/GERD -Insomnia (if staff are unaware they are not sleeping) Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 91 Medical Issues and Behavior • These medical symptoms may result in behavioral outbursts if the individual simply feels bad and is unable to communicate this to staff -Stuffing toilet with toilet paper-diarrhea -Frequent trips to the bathroom-constipation -Unusual behavior focused on one specific part of the body -Sudden, unexplained change in mood and behavior, accompanied by physical symptoms or complaints Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 92 What Do We Do? • Focus on the positive -Build from a person’s strengths and reward any positive behavior and effort. Spend time on “what’s right” with someone instead of talking about “what’s wrong” -Provide positive reinforcement and acceptance as people with thoughts and feelings, before focusing on challenging behavior Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 93 What Do We Do? • Know your individuals -Develop a rapport with the people you work with -Take time to learn their history -Understand their goals, needs and what they want -Develop a rapport with the family when possible Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 94 What Do We Do? • Provide ongoing training and education to support staff -Training and assistance with behavior management strategies such as positive reinforcement -The symptoms/behaviors associated with psychiatric diagnosis -Coping skills, impulse control skills -Welcome questions and concerns of support staff no matter how small the concerns may be at the time Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 95 What Do We Do? • Practice creative problem solving in order to find ways to meet the needs of the individuals you work with -Consider community resources -Take the initiative, reward others who take the initiative to address problems -Be proactive and fix problems before they become big problems -Take a team approach and communicate effectively with team members Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 96 What Do We Do? • Maintain a positive rapport with other professionals who work with the people you work with -Professional support staff, doctors, nurses, and others all have information, observations and experience that is valuable -Be open to consultation with others to the benefit of the individual Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 97 What Do We Do? • Regarding specific individuals -Do a thorough assessment (talk to everyone who works with the individual and get all available information that may be relevant) -Do not disregard information provided as relevant -Collect baseline data -Review the history of the individual -Develop a rapport with family/support staff -Listen to family and support staff, they spend the most time with the individual and have the most information -Meet with the team, or as many of the staff as possible at one time and brainstorm -Be a good detective -Make appropriate referrals for further assessment when indicated Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 98 The Hierarchy 1. Are the behaviors the result of medical conditions? (Would you create a behavior support plan for physical aggression………that is caused by pain from constipation) 2. Are the behaviors the result of psychiatric conditions? (Best practice for medicating diagnosed signs/symptoms) 3. Are the behaviors learned? Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 99 Distinguishing Learned Behavior From Psychiatric or Medical Illness • Symptom/behavior occurs in most or all settings it is more likely due to a psychiatric or medical condition • Symptom/behavior is unresponsive to consistent behavioral interventions and habilitative programming, it is more likely related to a psychiatric or medical condition • Changes in sleep, appetite, sexual, or daily functioning, it is more likely attributable to a psychiatric or medical condition • Autonomic symptoms are more likely related to psychiatric or medical condition • Onset of mental illness, or medical problem, may worsen already existing challenging behaviors-baseline exaggeration • May display usual challenging behavior and simultaneously display other behavior indicative of mental illness Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 100 Psychopharmacology • • • • • • • • • Mental Health supports for individuals with intellectual disability should focus on stimulation of healthy mental development, prevention of psychiatric disorders, and effective treatment of psychiatric disorders One of the most effective treatments for many mental health disorders is the prescription of psychotropic medication Far too many individuals with intellectual disability are given psychotropic medication Inappropriate use of psychotropic medications, primarily the antipsychotic agents, to sedate individuals with intellectual disability Caveat-medication prescribed as a substitute for appropriate treatment or habilitation, for the convenience of staff, or that its use was simply not supported by a relevant diagnosis Many individuals don’t benefit from their psychotropic drug treatment The rate of psychotropic medication usage has stabilized with individuals with intellectual disabilities Medication usage has begun to reflect the prescribing patterns of the general population, albeit as a higher level Persons with intellectual disabilities are one of the most medicated groups in our society Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 101 Guidelines for the Use of Psychotropic Medication • Drugs may have a place in the treatment of mental illness, regardless of whether or not the person treated has an intellectual disability • Guidelines published in Psychotropic Medications and Developmental Disabilities: The International Consensus Handbook (Reiss & Aman, 1998) Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 102 Guideline • Psychotropic medication shall not be used excessively, as punishment, for staff convenience, as a substitute for services, or in quantities that interfere with an individual’s quality of life • Disallow excessively high dosages • Inappropriate long-term use of medication • Not to be used to control someone’s behavior if that behavior is related to the appropriate expression of a personal right or is otherwise reasonable given the person’s situation • Not intended to compensate for insufficient or poorly trained staff, inadequate environmental conditions or untreated medical issues, or to serve as a substitute for appropriate behavioral or educational interventions Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 103 Guideline • Psychotropic medication must be used within a coordinated multidisciplinary care plan designed to improve the individual’s quality of life • Role of a multidisciplinary team makes a significant difference in the rates at which these medications are prescribed e.g. reduction Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 104 Guideline • The use of psychotropic medication must be based on a psychiatric diagnosis or specific behavioralpharmacological hypothesis resulting from a full diagnostic and functional assessment • Prescribed only for a specific diagnosis in the DSM • In response to a documented connection between the cause of unwanted behavior and the medication’s known propensity to act on that cause • [Psychotropic drugs should not be prescribed simply for “behaviors” or “aggression” without a proven cause-and-effect relationship] Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 105 Guideline • Written informed consent must be obtained from the individual, if competent, or the individual’s guardian before the use of any psychotropic medication and must be periodically renewed • Presentation of the risks and benefits of taking or not taking the medication, possible alternatives, and the right to refuse consent or revoke it at a later date • Form that the individual can understand Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 106 Guideline • Specific index behaviors and quality of life outcomes must be objectively defined, quantified, and tracked using recognized empirical measurement methods in order to monitor psychotropic medication efficacy • Index behaviors refer to observable signs or subjective feelings or sensations reported by the individual, by which changes in their condition may be measured • Consistently monitored by reliable documentation systems or through the use of symptom-rating scales • Implemented prior to the use of medication in order to establish a baseline for comparison with subsequent observations Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 107 Guideline • The individual must be monitored for sideeffects on a regular and systematic basis using an accepted methodology which includes a standardized assessment instrument • Scales or checklists designed to assess for side-effects should be used at least every 3 to 6 months, or as clinically indicated Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 108 Guideline • If antipsychotic or other dopamine-blocking drugs are prescribed, the individual must be monitored for tardive dyskinesia on a regular and systematic basis using a standardized assessment instrument • AIMS, DISCUS should be administered at least once every 6 months to assess for tardive dyskinesia • Even when a potential tardive dyskinesia-causing medication is discontinued, assessments should be repeated at one and two months afterwards to detect the possible emergence of withdrawal dyskinesia • In addition, if a person already has tardive dyskinesia but is no longer taking a dopamine-blocker, assessments should be conducted at 6 to 12-month intervals Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 109 Guideline • Psychotropic medication must be reviewed on a regular and systematic basis • It is recommended that at least every 3 months, or within 1 month after a medication or dosage change, the positive and negative effects of psychotropic medication should be formally reviewed • Reviewed by individual, all relevant treatment team members including the psychiatrist or other knowledgeable clinician • Goal-lowest effective dosage and simplest possible drug regimen are utilized • Ensure therapeutic monitoring is in place for medications that require it Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 110 Ensure Efficacy Of Individual’s Medication Regimen • Identify the changes expected as a result of taking of the medication • Identify the time frames by which these changes should occur • Develop a system to evaluate whether changes are occurring as planned (e.g. data tracking systems, rating scales) • Identify one person to collect and summarize relevant data • Present data to the support team and psychiatrist on an ongoing basis • Regularly evaluate the accuracy of initial diagnostic impressions • Regularly evaluate the effectiveness of the medication regimen (i.e., positive and negative effects) • Adjust diagnostic impressions and treatment approaches as indicated by data analysis Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 111 • • • • • • • • American Association of Mental Retardation Specific practices that should be minimized: Long term use of benzodiazepines (e.g. Ativan, Valium) Use of long-acting hypnotics (e.g. Dalmane, Doral) Long-term administration of anticholinergic medications (e.g. benzotropine) Use of anticholinergics in the absence of extrapyramidal side-effects High dosages of antipsychotic medications Employment of phenytoin, phenobarbital, or primidone as psychotropics or anticonvulsants [Medications on the so-called “Beers List” should be avoided whenever possible-outmoded or have replacement options which are much less likely to cause undesirable side-effects] Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 112 Other Considerations • • • • • • • • The right medication for the right length of time One of the primary reasons for treatment failure with psychotropic medication is failure to optimize the dosage or to allow adequate time for the medication to work Another reason for poor therapeutic outcome is increasing a dose too rapidlyoften results in adverse side-effects, which then lead to medication discontinuation or poor adherence to the prescribed regimen It is important to increase all medication dosages slowly and to decrease them slowly as well Recommended to prescribe as few medications as possible and in the lowest effective dosages, thus reducing the risk of drug-to-drug interactions as well as adverse side-effects Unnecessary or ineffective medications should always be discontinued [logic of “If the problem is still occurring with the medications, imagine how bad it would be if they were stopped” is seriously flawed.] The medications are not effective if the individual’s problem persists. Obtain all of a person’s medication from the same pharmacy in order to facilitate screening for drug interactions Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 113 Diagnostic & Statistical Manual-fourth edition-Text Revised (DSM-IV-TR) • According to the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV), Mental Retardation (MR) is characterized “by significantly sub average intellectual functioning (an IQ of approximately 70 or below) with onset before age 18 years and concurrent deficits or impairments in adaptive functioning” (American Psychiatric Association, 1994, p. 37). Subcategories differentiated by IQ scores include (DSM-IV, p. 40) • According to the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV), Pervasive Developmental Disorder is characterized by severe deficits and pervasive impairment in multiple areas of development. These include impairment in reciprocal social interaction, impairment in communication, and the presence of stereotyped behavior, interests, and activities. • Structural, descriptive basis of the diagnostic categories Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 114 DSM-5 New to the DSM-5, is a chapter on Neurodevelopmental Disorders which contains seven disorders that share impairments in a number of developmental areas, including personal, social, academic or occupational functioning. Some of the disorders are more likely to be detected early, such as the more severe variants of intellectual disabilities, autism spectrum disorders (ASD), motor disorders, tic disorders and communication disorders. However, other disorders in this category, like the specific learning disorders (SLD) or attention deficit/ hyperactivity disorder (ADHD) have been called the hidden disabilities because they are not obvious disabilities and often are detected only after significant failure has been experienced by the individual. The DSM-5 has clustered these disorders in the same chapter because the neurodevelopmental disorders frequently co-occur; for example individuals with autism spectrum disorder will often have intellectual disability (intellectual developmental disorder), and many children with attentiondeficit disorder (ADHD), also have a specific learning disorder. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 115 DSM-5: Diagnostic Changes Change in terminology Change in diagnostic classifications Intellectual Developmental Disorder is a disorder that includes both a current intellectual deficit and a deficit in adaptive functioning with onset during the developmental period. All three of the following criteria must be met. A. Intellectual Developmental Disorder is characterized by deficits in general mental abilities such as reasoning, problem-solving, planning, abstract thinking, judgment, academic learning and learning from experience. Intellectual Developmental Disorder requires a current intellectual deficit of approximately 2 or more standard deviations in Intelligence Quotient (IQ) below the population mean for a person’s age and cultural group, which is typically an IQ score of approximately 70 or below, measured on an individualized, standardized, culturally appropriate, psychometrically sound test. AND B. The deficits in general mental abilities impair functioning in comparison to a person’s age and cultural group by limiting and restricting participation and performance in one or more aspects of daily life activities, such as communication, social participation, functioning at school or at work, or personal independence at home or in community settings. The limitations result in the need for ongoing support at school, work, or independent life. Thus, Intellectual Developmental Disorder also requires a significant impairment in adaptive functioning. Typically, adaptive behavior is measured using individualized, standardized, culturally appropriate, psychometrically sound tests. AND C. Onset during the developmental period. Code no longer based on IQ level. [based on level of supports] Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 116 DSM-5: Diagnostic Changes Intellectual disability (intellectual developmental disorder) Diagnostic criteria for intellectual disability (intellectual developmental disorder) stress the need for an assessment of both cognitive capacity (IQ) and adaptive functioning. Severity is determined by adaptive functioning rather than IQ score. Intellectual disability replaces the term “mental retardation with intellectual disability” with a severity scale to reflect function, not I.Q.. The term intellectual developmental disorder was placed in parentheses to reflect the World Health Organization’s classification system, which lists “disorders” in the International Classification of Diseases (ICD) and bases all “disabilities” on the International Classification of Functioning, Disability, and Health (ICF). Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 117 Intellectual disability codes Intellectual disability codes all have a direct conversion code as follows: Severity ICD-9 code ICD-10 code Moderate ID 318.0 F71 Mild ID Severe ID Profound ID Unspecified ID 317 318.1 318.2 319 Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 F70 F72 F73 F79 118 DSM-5: Diagnostic Changes Autism spectrum disorder (ASD) Autism spectrum disorder is a new DSM-5 name. ASD now encompasses the previous DSM-IV autistic disorder (autism), Asperger’s disorder, childhood disintegrative disorder, and pervasive developmental disorder not otherwise specified. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 119 DSM-5: Diagnostic Changes A large controversy has surrounded this decision. Some of the comments have to do with: 1. Some persons fear that Asperger’s [less restrictive] will not meet the criteria for ASD [more restrictive] and they will lose benefits such as education, treatment, etc. 2. Some persons with Asperger’s do not want to be seen in the same light or category as people with autism. 3. Many mental health professionals believe that Asperger’s is different as an illness than autism. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 120 DSM-5: Diagnostic Changes DSM-IV Asperger’s disorder included: 1. Impairment in social interaction (2 of the following): nonverbal behaviors, no peer relationships, lack of shared activities, lack of social reciprocity. 2. No delay in language. 3. No cognitive delay. 4. Repetitive activities of behavior (1 of the following): pattern of activity, rituals, motor mannerisms, fixation on parts of objects. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 121 Autism Spectrum Disorder Neurodevelopmental Disorders [DSM-5 now replaces Rett’s disorder, childhood disintegrative disorder, Asperger’s disorder, and pervasive developmental disorder not otherwise specified with Autism Spectrum Disorder] Autism Spectrum Disorder 299.00 (F84.0)/ICD-10-CM Code Currently or by history With or without accompanying intellectual impairment With or without accompanying language impairment Symptoms change with development and may be masked by compensatory mechanisms Characteristic deficits of social communication, excessively repetitive behaviors, restricted interests, and insistence on sameness Typically recognized during the second year of life Not a degenerative disorder, and it is typical for learning and compensation to continue throughout life Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 122 DSM-5: Diagnostic Changes Autism spectrum disorders (symptoms present in early childhood, 3 levels of severity). Deficits in communication and interaction-include reciprocity, nonverbal interaction, having relationships, repetitive and/or restrictive behaviors; and expanded list of specifiers (for example- intellectual, language impairment, catatonia. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 123 DSM-5 controversy overview Combination of autism spectrum disorders into single category. One of the most publicized changes in the DSM-5 involves grouping all of the subcategories of autism into a single category as autism spectrum disorder (ASD). This move eliminates previously separate diagnoses of autism – including autistic disorder, Asperger’s disorder, childhood disintegrative disorder and pervasive developmental disorder “not otherwise specified” (PDD-NOS). Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 124 DSM-5 controversy overview This merging of categories creates a “sliding scale” for autism, meaning individuals will be diagnosed somewhere along the autism spectrum, given the personal severity of their symptoms. Many parents and health care providers have speculated that this transformation may end up excluding some of those already diagnosed with an autism disorder, like Asperger’s or PDD-NOS. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 125 DSM-5 controversy overview The specificity is going to go up, meaning the false positives are going to be less likely. Dr. Alexandar Kolevzon, associate professor of psychiatry and pediatrics at Mount Sinai Hospital in New York City, stated. “This universe of people with PDD-NOS; it’s possible that some of those patients may no longer meet those criteria. Some of the debate revolves around Asperger’s, but it seems to me that most people diagnosed with Asperger’s will still be on the autism spectrum.” Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 126 DSM-5 controversy overview Over the past decade, the United States has seen a striking increase in the amount of autism diagnoses, with the Centers for Disease Control and Prevention estimating that one in 88 children suffers from an autism spectrum disorder. According to Kolvezon, numerous epidemiological studies have found that the majority of children accounting for this incidence are those with PDD-NOS; a diagnosis given to those with communication issues and pattern of behavior but who do not meet the full criteria for autism or another pervasive developmental disorder. Kolevzon said it’s possible that over-diagnosis of PDD-NOS has led to this increase in autism spectrum disorder cases. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 127 DSM-5 controversy overview “What happens in the community is that the diagnosis of autism spectrum disorder virtually guarantees a whole host of therapies such as speech therapy, occupational therapy, behavioral therapy, and potentially physical therapy.” Kolevzon said “Theoretically it’s possible that community providers and clinicians are incentivized to label kids with PDD-NOS, because it would make it more likely to receive appropriate services.” Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 128 DSM-5 controversy overview The autism spectrum disorder scale will further refine the way providers diagnose autism, Kolevzon said, by recognizing differences from person to person rather than trying to generalize them into one of four categories. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 129 DSM 5 A developmental focus New diagnostic criteria A move toward “dimensional” measures Increased emphasis on culture and gender A new section on areas that need further research • A commitment to more frequent updating • Inclusion of International Classification of Diseases (ICD) codes • • • • • Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 130 DSM 5 For the first time ever, the DSM depends on and incorporates evidence from the neurosciences, genetic studies, twins studies, and overall areas of research that had been largely ignored in previous editions of the DSM. One of the biggest changes in the new edition is a dramatically fresh approach to diagnostics. • New classification system • Newly organized trauma disorders • Changing diagnostics for children & adolescents • Impulse control & anxiety disorders • Revised categories for schizophrenia, mood disorders and more • New diagnoses Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 131 DSM-5 Guidebook for diagnosis, court evaluations, and insurance reimbursement. It also defines what is normal and what is abnormal in our culture, and by implication, where the limits are of personal responsibility. Excludes "science" of mental illness. No biological criteria as part of its description, either from blood work, brain scan, or genetic markers. The manual remains totally dependent on client history and clinical observation. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 132 DSM-5 Guidebook The Essential Companion To The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 133 Autism The American Psychiatric Association released new guidelines for the diagnosis of autism spectrum disorders last year. Research suggests that the new diagnostic criteria could miss thousands of children who have developmental delays without an autism diagnosis. It was found that under the new DSM-V criteria, there were 31% fewer autism spectrum disorders diagnosed, compared to what would have been diagnosed with the DSM-IV. The decline in diagnosis could mean that individuals are missing out on services and support. Honor Whiteman, Medical News Today 02/26/2014 Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 134 Autism Last year, the American Psychological Association issued new guidelines for the diagnosis of autism spectrum disorder. But new research from Columbia University School of Nursing in New York, NY, suggests that these guidelines could leave thousands of children who have developmental delays without autism diagnosis, meaning they will miss out on social services, educational support and medical benefits. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 135 Autism Or . . . . . it could mean that fewer children are being diagnosed who did not need to be diagnosed with autism spectrum, which is a good thing. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 136 Diagnostic Manual for Individuals with Intellectual Disabilities (DM-ID) • • • • • The DM-ID Diagnostic Manual – Intellectual Disability (DM-ID): A Clinical Guide for Diagnosis of Mental Disorders in Persons with Intellectual Disability focuses on issues related to diagnosis in people with Intellectual Disability (ID), the limitations in applying DSM-IV-TR criteria to people with ID, and adaptation of the diagnostic criteria. It has been abridged for clinical usefulness from The Diagnostic Manual – Intellectual Disability (DM-ID): A Textbook of Diagnosis of Mental Disorders in Persons with Intellectual Disability which was developed by the National Association for the Dually Diagnosed (NADD), in association with the American Psychiatric Association (APA), and is a diagnostic manual designed to be an adaptation of the DSM-IV-TR. Grounded in evidence-based methods and supported by the expert-consensus model, the DM-ID(Textbook) offers a broad examination of the topic, including a description of each disorder, a summary of the DSM-IV-TR diagnostic criteria, a review of the research and an evaluation of the strength of evidence supporting the literature conclusions, a discussion of the etiology and pathogenesis of the disorders, and adaptations of the diagnostic criteria for persons with Intellectual Disability (ID). The goal of both volumes is to facilitate a more accurate psychiatric diagnosis of people with ID. Chapters in the DM-ID cover special issues (i.e., assessment and diagnostic procedures and presentations of behavioral phenotypes of genetic disorders) as well as the individual DSM-IV-TR categories. For each disorder, descriptive text and details of how to apply diagnostic criteria, as well as tables of adapted diagnostic criteria, are included. In addition to adapting the DSM-IV-TR diagnostic criteria where appropriate, the DM-ID provides advice about and considerations for assessing and diagnosing individuals with ID and coexisting mental health needs. In some cases, it is not so much that the criteria need to be adapted, as that a different method of eliciting the necessary information must be used. Information is provided in recognizing common behaviors of individuals with intellectual disabilities and in how to differentiate these behaviors from psychiatric disorders. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 137 Diagnostic Manual for Individuals with Intellectual Disabilities (DM-ID) • • • • • The Problem Although psychiatric disorders in persons with ID are common, they are often not appropriately identified. The provision of adequate mental health treatment for people with ID continues to be lacking, in part, because reliable psychiatric diagnosis remains a clinical challenge. Determining an accurate psychiatric diagnosis becomes especially difficult as the level of intellectual functioning declines. Children and adults who have ID coexistent with psychiatric disorders may be one of the most underserved populations in the United States. These individuals may fall through the cracks in service delivery systems when neither the local mental health service system nor the developmental disability service system is willing or able to assume responsibility for their treatment, services, and support. Individuals with ID have been estimated to be 2 to 4 times more likely than those in the general population to experience psychiatric disorders. Researchers have found that as many as one third or more of all people with ID have significant behavioral, mental, or personality disorders requiring mental health services. Often people with ID who exhibit psychiatric problems are denied services or receive inappropriate treatment and services. During the past few decades, there have been important developments in the field of mental health care for people with ID. The National Association for the Dually Diagnosed (NADD) has been instrumental in marshaling national and international attention, providing education and training, and disseminating relevant clinical and policy issues. In spite of these encouraging developments, however, there remain significant obstacles hindering appropriate care and treatment for this underserved population. One key problem is the absence of a diagnostic system appropriate for clinical use with the diverse population of people with ID. As a result, individuals may receive no psychiatric diagnosis even when a mental disorder exists, or they may receive an inaccurate or inappropriate diagnosis. Because treatments, services, and supports are tied directly to the accurate evaluation and diagnosis of people who have ID coexistent with mental disorders, the absence of psychiatric diagnoses is a central issue. Clinicians need a system whereby they can recognize the presence of DSM-IV-TR-documented mental disorders in persons who have limited expressive and receptive language skills. A major potential advantage of the DM-ID is that it may enhance the reliability of psychiatric diagnoses in persons with ID which could ultimately improve treatment outcomes. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 138 Diagnostic Manual for Individuals with Intellectual Disabilities (DM-ID) • • • • • • The Problem (continued) There are a number of factors associated with the difficulty of making an accurate diagnosis in people with ID. The applicability of existing standardized classification systems (such as the DSM-IV-TR) for persons with ID has been critically debated in professional literature. To determine whether a person within the general population has been experiencing psychiatric symptoms, a clinician typically relies on the person’s description of his or her experiences and feelings. Individuals with cognitive impairments experience difficulties in receptive and expressive language to varying degrees. Mild limitations in cognitive and verbal skills make it difficult, and severe limitations may make it impossible, for people with ID to articulate such abstract or global concepts as depressed mood or to communicate subtle differences among emotional or motivational states. Other factors that increase the difficulty in making psychiatric diagnoses include the tendency for some people with ID to attempt to hide their disabilities (to adopt a “cloak of competence”), the tendency not to be forthcoming with respect to self-descriptions, and the tendency for some to try to please the evaluator by answering falsely or in a manner that is inaccurate (“acquiescence bias”). Additionally, the symptoms of diverse psychiatric disorders are often expressed differently in people with ID. Four processes that are common in persons with ID that can influence the diagnostic decision-making process are baseline exaggeration, intellectual distortion, psychosocial masking, and cognitive disintegration. Another diagnostic challenge is diagnostic overshadowing. Having a diagnosis of ID can overshadow coexisting mental disorders and may predispose practitioners to overlook the presence of psychopathology, because unusual or anomalous behavior is attributed by the clinician to being artifacts of developmental or social delay. For example, a person with Profound ID who is very withdrawn and asocial might be less likely to be labeled as depressed than would a person with average intelligence. Accurate diagnosis is important because it provides a sound basis for effective treatment. For many patients and their families diagnostic understanding will reduce confusion and uncertainty. Positive treatment outcome is based on an accurate diagnosis. Just as this is true concerning physical health, it is equally true in psychiatric health. Severe behavioral disturbance in the form of verbal or physical aggression toward others, self-injury (aggression toward self), and property destruction frequently motivates referrals for diagnosis and treatment prescription. Such severe disturbance occurs at a clinically significant rate among people with ID, often threatens the stability of family living or the continuation of community living in a relatively nonrestrictive setting, and can precipitate admission to a public mental health or ID facility. Severe behavioral disturbance of various types occurs among people with Mild to Profound ID. However, it is important to understand that severe behavioral disturbances are not part and parcel of a diagnosis of ID. The presence of clinically significant behavioral disturbances mandates a thorough clinical diagnostic evaluation to determine the presence of comorbid mental disorders that may be responsible for the behavioral disturbance. The extent to which behavioral disturbances represent symptom equivalents for symptoms such as depression and anxiety, especially in individuals with severe and profound ID, has been the subject of considerable debate, which remains to be elucidated by further research Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 139 Diagnostic Manual for Individuals with Intellectual Disabilities (DM-ID) • • • Classification and Diagnosis of Mental Illness The clinician is faced with certain challenges when an individual with ID presents with disturbed or disturbing behavior. There has been controversy found in the literature concerning the issue of reliability in making specific DSM-IV-TR diagnosis in persons with ID, especially those with more severe impairment and intellectual function. Some researchers assert that as intelligence decreases the validity of psychiatric diagnosis for individuals with ID tends to decrease. They explain this as the result of both an increase in nonspecific organic factors and the relative inaccessibility of the individual’s inner life as productive speech decreases with the increased severity of impairment. Despite a general consensus that mental disorders can be diagnosed using standard diagnostic criteria for people with mild ID and reasonably good communicative skills, clinicians generally acknowledge the increased difficulty for individuals with more severe ID and poor verbal skills. In fact, the DSM-IV-TR itself recognizes that some diagnostic criteria need to be modified when they are applied to children, both because the symptom profile of some disorders differs in children (for example, the substitution of “irritable mood” for “depressed mood” in the diagnostic criteria for Major Depressive Episode and Dysthymic Disorder in children) and because some diagnostic criteria do not apply to children (for example, there is no requirement in specific phobia descriptions that children recognize that their fears are excessive or unreasonable). Although criteria set modifications have been proposed for different cultural groups—for the medically ill and for geriatric patients among others, as well as those for children—no other modifications are included in the DSM-IV-TR. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 140 Diagnostic Manual for Individuals with Intellectual Disabilities (DM-ID) • • • • • • • • • 10 years in the making thru NADD Diagnosing Axis I Disorders in individuals diagnosed with different levels of Mental Retardation Central premise is the thesis that a psychiatric diagnosis is a necessary, but not sufficient, basis to justify the use of psychotropic medication in individuals with intellectual disabilities (ID) Mild/Moderate Severe/Profound Companion to DSM Implications of necessity of DM-ID-difficulty in diagnosing Axis I disorders In 2007, NADD, in association with the American Psychiatric Association (APA), published Diagnostic Manual—Intellectual Disability (DM-ID). The DM-ID is a companion to and adaptation of the APA’s Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IVTR) for use with individuals who have an intellectual/developmental (IDD) disability co-occurring with mental illness (MI). The goal of the DM-ID was to provide more accurate psychiatric diagnoses for individuals with IDD/MI. The DM-ID has been very well accepted and is considered the “gold standard” for diagnosing psychiatric disorders in individuals with IDD The DSM is used by mental health professionals to diagnose psychiatric disorders. Among the information it includes is a list of the symptoms (criteria) that must be present in order to diagnose an individual with a particular psychiatric disorder. Generally the mental health professional will determine the presence or absence of these symptoms through what the patient states in terms of feelings, experiences, and symptoms. However, individuals with IDD usually have limited verbal ability and may lack the ability to describe their internal state. Also, various psychiatric disorders manifest differently in individuals with IDD from the way they manifest in non-disabled individuals. The DM-ID describes these differences and provides information about how to make an accurate psychiatric diagnosis in an individual with IDD without needing to rely on the individuals selfreport. The importance of this is that a more accurate psychiatric diagnosis will lead to more appropriate treatment, which will, in turn, lead to improved quality of life for the individual with IDD co-occurring with mental illness. Peer-reviewed, published research clearly indicates the clinical utility of the DM-ID. For further information about the DM-ID you may visit the DM-ID website. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 141 DM-ID-2 • • • • DM-ID-2 NADD has begun work on the revision of its seminal Diagnostic Manual – Intellectual Disability (DM-ID). In 2007, NADD, in association with the American Psychiatric Association (APA), published Diagnostic Manual—Intellectual Disability (DM-ID). The DM-ID is a companion to and adaptation of the APA’s Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) for use with individuals who have an intellectual/developmental (IDD) disability co-occurring with mental illness (MI). The goal of the DM-ID was to provide more accurate psychiatric diagnoses for individuals with IDD/MI. The DM-ID has been very well accepted and is considered the “gold standard” for diagnosing psychiatric disorders in individuals with IDD The DSM is used by mental health professionals to diagnose psychiatric disorders. Among the information it includes is a list of the symptoms (criteria) that must be present in order to diagnose an individual with a particular psychiatric disorder. Generally the mental health professional will determine the presence or absence of these symptoms through what the patient states in terms of feelings, experiences, and symptoms. However, individuals with IDD usually have limited verbal ability and may lack the ability to describe their internal state. Also, various psychiatric disorders manifest differently in individuals with IDD from the way they manifest in non-disabled individuals. The DM-ID describes these differences and provides information about how to make an accurate psychiatric diagnosis in an individual with IDD without needing to rely on the individuals self-report. The importance of this is that a more accurate psychiatric diagnosis will lead to more appropriate treatment, which will, in turn, lead to improved quality of life for the individual with IDD co-occurring with mental illness. Peer-reviewed, published research clearly indicates the clinical utility of the DM-ID. For further information about the DM-ID you may visit the DM-ID website. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 142 DM-ID-2 • The APA will be releasing a revision of the Diagnostic and Statistical Manual in May (DSM-5). With the release of the DSM-5 it becomes important that the DM-ID be revised to correspond the DSM-5 and to incorporate the changes in the DSM-5. There are many changes and revisions planned in this edition. It will be important to incorporate these changes into a future volume of the DM-ID to insure the most accurate psychiatric diagnoses for individuals with IDD. • NADD has embarked on a multi-year project to revise the DM-ID to correspond to the DSM-5. Dr. Robert Fletcher will be Chief Editor, and Dr. Sally-Ann Cooper and Dr. Jarrett Barnhill will be CoEditors. NADD will again use an expert-consensus model, with work groups of 4-8 experts for each of 22 diagnostic categories. The DMID-2 will use the same diagnostic categories identified in the DSM-5. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 143 Psychodynamic Diagnostic Manual (PDM) A collaborative effort American Psychoanalytic Association International Psychoanalytical Association Division of Psychoanalysis (39) of the American Psychological Association • American Academy of Psychoanalysis and Dynamic Psychiatry • National Membership Committee on Psychoanalysis in Clinical Social Work • • • • Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 144 PDM • The Psychodynamic Diagnostic Manual (PDM) is a diagnostic framework that attempts to characterize an individual’s full range of functioning-the depth as well as the surface of emotional, cognitive, and social patterns. It emphasizes individual variations as well as commonalities. We hope that this framework brings about improvements in the diagnosis and treatment of mental disorders and permits a fuller understanding of the functioning of the mind and brain and their development. The goal of the PDM is to complement the DSM and ICD efforts of the past 30 years in cataloguing symptoms by explicating the broad range of mental functioning. • Treatments that focus on isolated symptoms or behaviors (rather than personality, emotional, and interpersonal patterns) are not effective in sustaining even narrowly defined changes. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 145 PDM • Neurodevelopmental Disorders of Relating and Communicating (NDRC) • Type I: Early Symbolic, with Constrictions • Type II: Purposeful Problem Solving, with Constrictions • Type III: Intermittently Engaged and Purposeful • Type IV: Aimless and Unpurposeful Other Neurodevelopmental Disorders (Including Genetic and Metabolic Syndromes) Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 146 National Association for the Dually Diagnosed (NADD) • www.theNADD.org • Positive Identity Development-Dr. Karyn Harvey • Trauma-Informed Behavioral Interventions-Dr. Karyn Harvey • Founded in 1983 as a not-for-profit Association. The catalyst for the founding of NADD arose from the need for an open forum to promote and exchange of ideas, principals & concepts concerning individuals who have the co-existence of ID/D and mental illness. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 147 American Association on Intellectual and Developmental Disabilities (AAIDD) • www.AAIDD.org • Formerly American Association on Mental Retardation (AAMR) changes name to American Association on Intellectual Disabilities (AAIDD)-January 1, 2007 • New name reflects new philosophy • Supports Intensity Scale (SIS) • Positive Behavior Supports Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 148 Positive Behavior Supports (PBS) • Setting the person up to succeed • A PBS framework maintains a focus on individual quality of life (QOL) as the predominate outcome of interest. Challenging behavior becomes a target of treatment intervention then, not because of some inherent value of the behavior, but because of the negative impact a behavior imparts on an individual’s quality of life. In considering this, it follows that the focus of intervention is more often on the environmental context and systemic root of a challenging behavior than on the simple extinction of that behavior. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 149 Behavioral (Health) Assessment and Functional Analysis Behavioral (health) assessment is an analysis aimed at identifying the history, presentation, purpose, and outcome of a particular behavior. Functional analysis (assessment) is one part of the behavioral assessment. The functional analysis focuses on the cause and outcome of the behavior. It is used to identify why a person may be exhibiting a behavior, what needs are being met by the behavior, and what interventions have been effective or ineffective. -Observations of the individual in various environments -A history of the challenging behaviors, including the identified target behavior -Specific definitions of challenging behaviors -Interventions that have been attempted and the effectiveness of those interventions -Outcome of the behavior (how did others respond, etc.) -Hypotheses about the purpose of the target behavior -A method of data collection in order to measure and record the target behavior Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 150 Functional Behavioral Assessment (FBA) Functional behavioral assessment (FBA) is a variation on procedures originally developed to ascertain the purpose or reason for behaviors displayed by individuals with severe cognitive or communication disabilities (e.g., individuals with mental retardation or autism). Because these individuals were unable to fully explain why they were displaying certain inappropriate behaviors, methods were developed to determine why they demonstrated such actions. These investigatory procedures, derived primarily from the orientation and methods of applied behavior analysis were known as "functional behavioral analysis". By gathering data and conducting experiments that evaluated the effects of environmental variables on the behavior, concerned staff members could usually decipher the meaning of the behaviors (i.e., what emotion or message was being communicated through the actions), determine why they were occurring, and develop behavior change programs to help the disabled individual display more appropriate behavior in meeting his or her needs. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 151 Role of the Functional Analysis • It is a systematic way to assess a person’s behavior with the goal of understanding why it occurs. • It assumes that all behaviors occur for reasons and have meaning. • It assumes that behaviors do not occur without specific antecedents or triggers, even if those triggers are not always observable by others. • Identification of the target behavior • Data collection • Hypothesis generation • Plan development • Plan implementation • Data collection • Review of plan effectiveness Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 152 Implementation of PBSPs Relevance to their job duties from the DSP perspective Logistical issues with respect to training, implementation, and documentation New developments in Psychotropic medications and the integration behavioral approaches Support/accountability from supervisors and administration and implementation of a monitoring system to assess efficacy and promote continuous program improvements Conceptual understanding of Positive Behavior Support “Buy in” by Direct Support Professionals based on how the PBSP is presented/taught and the context in which it is taught Perception of the individuals we support-whole human beings versus one dimensional entities (patient, client, etc.)-“In defining quality of life, we must not draw boundaries and relegate everything beyond those boundaries to the ‘abnormal’. Instead, we must do everything in our power to build the kind of broadminded society in which people living with disabilities do not have to consider themselves ‘handicapped’ and can manifest their full potential”-Daisaku Ikeda from On Being Human/Positive Identity Development-Karyn Harvey, Ph. D. Role of staff and their behavioral change vis a vis the PBSP interventions Role of staff and their understanding of the concept of behavior change and the role of the environment on behavior change Reinforcement of staff in the correct implementation of the PBSP Reinforcement of staff in the incorrect or lack of implementation of the PBSP Values/education of Direct Support Professionals that impact the PBSP implementation Bigger picture of the mission/vision of the facility Conceptualization of the ability to “learn” and the implications of the learning Hopefulness or hopelessness about their role and the role of the individual Conceptualization of “mental retardation”, ID, DD Conceptualization of the usage of medications Tainted culture by veteran staff to new staff Engagement in the environment as a first line defense Sate environment Social relevance Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 153 State Policies and Practices in Behavior Supports INTELLECTUAL AND DEVELOPMENTAL DISABILITIES 2013, Vol. 51, No. 6, 433–445 AAIDD DOI: 10.1352/1934-9556-51.6.433 State Policies and Practices in Behavior Supports for Persons With Intellectual and Developmental Disabilities in the United States: A National Survey David A. Rotholz, Charles R. Moseley, and Kinsey B. Carlson Abstract Providing effective behavioral supports to decrease challenging behavior and replace it with appropriate alternative skills is essential to meeting the needs of many individuals with intellectual and developmental disabilities (IDD). It is also necessary for fulfilling the requirements of Medicaid funded individual support plans and is important for moral, ethical, and societal reasons.Unfortunately, there is no national standard for behavioral support practices or source of information on the status of behavior support policies, practices, and services for adults with IDD at either state or national levels. The collection of comprehensive data on state behavior support definitions, provider qualifications, training, and oversight requirements is a necessary starting point for the development of plans to address needed policy and practice changes. This survey is the first national assessment of state policies and practices regarding the definition and delivery of behavior support services to people with intellectual and developmental disabilities receiving publicly financed supports in the United States. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 154 Psychiatric medication • • • • • • • • • • • • • Treat signs/symptoms of diagnosed psychiatric disorder Anti-anxiety Anti-depressive Anti-psychotics Not for behavior Placebo better than antipsychotic drugs for treating aggression in the intellectually disabled No evidence that MR per se changes the mechanism of action of psychotropic drugs (pharmacokinetics) Influenced by a medical/neurological disorder “associated” with MR “L”ithium-incorrect (not trade name e.g. Lithobid) lithium-correct (salt) Standing psychotropic PRN medications are not permitted-use STAT Use of PRN medications should not be utilized for longer than a few weeks. Agitation is not a sufficient rationale as it describes an internal state Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 155 Manual for Psychiatric Clinics • Specific detailed procedures • Integration of psychological/behavioral/psychiatric data Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 156 Restraint Physical: any manual method that restricts freedom of movement or normal access to one’s body, including hand or arm holding to escort an individual over his or her resistance to being escorted. Physical restraint does not include medical intervention or brief, limited, and isolated use of physical guidance, positioning, or prompting techniques that are used to teach or redirect an individual or assist, support, or protect the individual during a functional therapeutic or physical exercise activity; response blocking and brief redirection used to interrupt an individual’s limbs or body without the use of force so that the occurrence of challenging behavior is prevented; holding an individual without the use of force to calm or comfort, or hand-holding to escort an individual from one area to another; and response interruption used to interrupt an individual’s behavior using facility-approved techniques. The only approved physical restraint techniques are hand, arm, and leg holds and techniques covered in the prevention and management of aggressive behavior (PMAB) curriculum. [Non-contingent physical restraints are not permitted] Chemical: any drug prescribed or administered to sedate an individual or to temporarily restrict an individual’s freedom of movement for the purpose of managing the individual’s behavior. Mechanical: any device attached or adjacent to an individual’s body that he or she cannot easily remove that restricts freedom of movement or normal access to his or her body. The term does not include medical intervention or any device used to achieve functional body position or proper balance or to prevent injury due to involuntary movement (e.g., falls due to seizures). Only those commercially available mechanical restraint devices designed specifically for safe and relatively comfortable restraint are permitted to be used. Prone: any physical or mechanical restraint that places the individual in a face down position. Prone restraint does not include medical intervention or brief physical holding of an individual who, during an incident of physical restraint, rolls into a prone position, when staff restore the individual to a standing, sitting, or side-lying position as soon as possible. Prone restraint is prohibited. Supine: any physical or mechanical restraint that places the individual on his or her back. Supine restraint does not include medical intervention or brief physical holding of an individual who, during an incident of physical restraint, rolls into a supine position, when staff restore the individual to a standing, sitting, or side-lying position as soon as possible. Supine restraint is prohibited. SECTION 1. Chapter 592, Health and Safety Code, is amended by adding Subchapter E to read as follows: SUBCHAPTER E. USE OF RESTRAINTS IN STATE SUPPORTED LIVING CENTERS Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 157 Not Restraint • • • • • • • • • • • Adaptive Supportive Devices-provide individual with opportunity to have more normal posture or freedom of independent movement (bedrails not permitted for “safety”) Medical Protective Devices-used to treat a medical condition or to aid in wound healing following an injury or surgical lesion Medical Immobilization-prevents movement during medical procedure Issue is the function of the restraint not the structure of the restraint We don’t restrain people because they are upset We don’t release people from restraint because they are calm Upset/calm is the establishing operation surrounding the behavior that places the individual at imminent risk of harm to self or others Imminent risk of harm to self or others is the criteria Risk versus Risk analysis: Liability accrues whether the restraint is given or not given (more trouble by not following physician order and not administering chemical restraint if someone is harmed than by following physician order and administering chemical restraint and no one is harmed/nurse judgement/how many nurses have lost licenses in both scenarios) Calm time is the time to administer the chemical (behaviors occur cyclically and therefore there are peaks and troughs, therefore the chemical restraint is more effective when given at a a trough time/easier to administer/chemical restraint is more effective during trough time/consider behvioral events leading up to physician order for chemical restraint and that rather than being reactive to the preceding behavioral episode, being proactive to the possibility of ongoing behavioral episodes/data is important to substantiate clinical judgment related to the administration or non-administration of the chemical restraint based on the individual’s behavior/history being the greatest predictor of future events e.g. in the current behavioral episode) The issue of “calm” is irrelevant and should never be the determining factor in either initiating or terminating a restraint of any kind. “Calm” is the establishing operation or context in which the challenging behavior is either occurring or is not occurring. The issue at hand is whether the individual is at imminent risk of harm to self or others. If the individual in question is known to staff e.g. clinical judgment, to the degree that displaying “calm” behavior does not preclude the ongoing imminent risk of harm to self or others then the individual may be assessed as such regardless of whether the individual is “calm” or not. Again, the issue of “calm” is irrelevant to the issue of imminent danger to self or others and thus to the issue of restraint. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 158 Safe Restraints No prone restraint Only approved restraints Immediate and serious risk of harm Terminate restraint when no longer danger No injury to the individual as result of using restraint • No evidence restraint was used for punishment • No evidence restraint used for convenience • • • • • Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 159 Restraint Not Used As Alternative – APPROPRIATE ASSESSMENTS – PBSP TO ADDRESS BEHAVIORS RESTRAINED – EVIDENCE OF ISP/PBSP IMPLEMENTATION – STRATEGIES TO REDUCE USE OF RESTRAINT – ENGAGED MEANINGFULLY – CONSISTENT PSYCHIATRIC TREATMENT – COMMUNICATION, IF RELATES TO BEHAVIOR – NO MEDICAL UNTREATED Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 160 Restrained After Less Restrictive Measures – USED PMAB – USED THE PBSP – ATTEMPTED LEAST RESTRICTIVE FIRST – PRIOR TO CHEMICAL CONTACTED BHS TO REVIEW/ASSESS FOR LESSER RESTRICTIVE METHODS. – MEDICAL/DENTAL EVIDENCE TREATMENT ATTEMPTED WITHOUT RESTRAINT – NO CONTRAINDICATIONS: ISP, PBSP, MEDICAL Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 161 Restraints DISCUSS/ DETERMINE RELEVANCY/ACT – Adaptive skills, biological, medical, psychosocial issues – Environmental variables (setting events) – Environmental antecedents – Variables maintaining the dangerous behaviors (consequences) – *Is there a current PBSP? Or in development – *Is there a Crisis Intervention Plan – The PBSP was reviewed and complete • Integrity data at 80% within two months of cluster – The CIP was reviewed and complete Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 162 Senate Bill (S.B.) No. 41 • • • • • • • • • • • • • • • • • • • • AN ACT relating to the use of restraints in state supported living centers. BE IT ENACTED BY THE LEGISLATURE OF THE STATE OF TEXAS: SECTION 1. Chapter 592, Health and Safety Code, is amended by adding Subchapter E to read as follows: SUBCHAPTER E. USE OF RESTRAINTS IN STATE SUPPORTED LIVING CENTERS Sec. 592.101. DEFINITION. In this subchapter, "executive commissioner" means the executive commissioner of the Health and Human Services Commission. Sec. 592.102. USE OF RESTRAINTS. (a) The executive commissioner shall adopt rules to ensure that: (1) a mechanical or physical restraint is not administered to a resident of a state supported living center unless the restraint is: (A) necessary to prevent imminent physical injury to the resident or another; and (B) the least restrictive restraint effective to prevent imminent physical injury; (2) the administration of a mechanical or physical restraint to a resident of a state supported living center ends immediately once the imminent risk of physical injury abates; and (3) a mechanical or physical restraint is not administered to a resident of a state supported living center as punishment or as part of a behavior plan. (b) The executive commissioner shall adopt rules to prohibit the use of prone and supine holds on a resident of a state supported living center except as transitional holds. Sec. 592.103. STANDING ORDERS FOR RESTRAINTS PROHIBITED. (a) A person may not issue a standing order to administer on an as-needed basis mechanical or physical restraints to a resident of a state supported living center. (b) A person may not administer mechanical or physical restraints to a resident of a state supported living center pursuant to a standing order to administer restraints on an as-needed basis. Sec. 592.104. STRAITJACKETS PROHIBITED. A person may not use a straitjacket to restrain a resident of a state supported living center. Sec. 592.105. DUTY TO REPORT. A state supported living center shall report to the executive commissioner each incident in which a physical or mechanical restraint is administered to a resident of a state supported living center. The report must contain information and be in the form required by rules of the executive commissioner. Sec. 592.106. CONFLICT WITH OTHER LAW. To the extent of a conflict between this subchapter and Chapter 322, this subchapter controls. SECTION 2. Not later than January 1, 2012, the executive commissioner of the Health and Human Services Commission shall adopt rules required under Sections 592.102 and 592.105, Health and Safety Code, as added by this Act. SECTION 3. This Act takes effect immediately if it receives a vote of two-thirds of all the members elected to each house, as provided by Section 39, Article III, Texas Constitution. If this Act does not receive the vote necessary for immediate effect, this Act takes effect September 1, 2011. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 163 Title 40, Part 1, Chapter 5, Subchapter H – General Principles for the Use of Restraint, §5.355 • • • • • • b) Upon an individual's admission to a state MR facility, an IDT must: (1) with the involvement of a physician, identify: (A) the individual's known physical or medical conditions that might constitute a risk to the individual during the use of restraint; and (B) other factors that must be taken into account if the use of restraint is considered including, but not limited to, the individual's cognitive functioning level, size, weight, emotional condition (including whether the individual has a history of having been physically or sexually abused), and age; and (2) document the identified conditions and factors and, as applicable, limitations on specific techniques or mechanical devices for restraint, in the individual's record. (c) At least annually, or when significant changes occur to the extent and nature of the identified conditions and factors documented in the individual's record, the IDT must ensure that a physician, advanced practice nurse, or physician assistant reviews and updates, as necessary, the identified conditions, factors, and limitations on specific techniques or mechanical devices for restraint documented in the individual's record. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 164 Senate Bill (S.B.) No. 34 • Administration of psychoactive medications in facilities • Takes effect September 1, 2013 Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 165 Psychotropic Medication for a Psychiatric Emergency This is a relatively new concept, and in the past, this type of processing was categorized as a chemical restraint. This new concept emphasizes a psychiatric treatment need and the medication is in response to an escalation or exacerbation of the signs and symptoms that the psychiatrist and IDT have discussed and documented as part of the ISP. In contrast to chemical restraint, if there is a psychiatric emergency, the intent of the medication has a relationship to treatment of the presenting medical condition. The teams should be aware of the use of psychotropic medication as part of a psychiatric emergency and the difference from a chemical restraint. Our psychiatrists can help with the clarification of this difference. “Crisis” Intervention Plan-Behavior that is predicted It would be hard to develop a plan for behavior that isn’t predicted. A CIP is based on the behaviors that an individual exhibits that requires the use of restraint Definition of “emergency” precludes routine, predicted, or expected Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 166 Psychotropic Medication • Texas Administrative Code (TAC) • Rules of the Texas Department of Mental Health and Mental Retardation • Title 25, Part II • New Subchapter Governing • PRESCRIBING OF PSYCHOTROPIC MEDICATION• MENTAL RETARDATION FACILITIES • Chapter 405, Subchapter B • EFFECTIVE DATE: August 19, 1994 • Guidelines for the Use of Psychotropic Medication Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 167 Seclusion • Prevention of egress • Not allowed: person cannot leave area whether a room, a central location, or a building • Issue is the function (not structure) • Issue is rights (due process) Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 168 Role of Psychologists in Administration of Psychotropic Medications • • • • • • • • • Psychologists are legally prescribing psychoactive medications in seven states, including the island of Guam, a territory of the US. This issue has been addressed on a state by state basis thru the psychology licensing boards over the past twenty five years. Non-prescriber therapists should communicate with prescribing clinicians if, in their assessment, such communication may be helpful to the client. In other words, the best interests of the patient should determine whether the non-prescriber therapist should be engaged with prescribing clinician. While Consulting With Prescribing Clinician, Non-Prescribing Therapist Should: Obtain an authorization to release information. Even though HIPAA law allows psychotherapists to discuss medication and other treatment issues with medicating clinicians, most state laws require that therapists, in most situations, obtain client authorizations before disclosing any confidential information to the prescribing clinician. Provide only the minimum information necessary. Be careful with the release of information related to people who are not your clients but are related to the client, such as spouses, children, parents, etc. Suggest different medication, different doses or recommend the discontinuation of medication. Be advised to document their medication consultation with clients and medicating clinicians or anyone else they may consult with (i.e., parents, etc). In summary, non-prescribing psychotherapists can play an important role in helping clients manage their psychotropic medications. Needless to say, they should never prescribe, discontinue or change clients’ meds, unless they are licensed to prescribe. Non-prescribing psychotherapists may inform clients about treatment options, including medications, and consult with the medicating physician as clinically necessary. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 169 Applied Behavior Analysis (ABA) • Originated in Psychology • Implications for licensure/board regulating BCBA • Application of learning theory/behavioral principles to real life • Classical conditioning: antecedents to the behavior • Operant conditioning: consequences to the behavior Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 170 Role of environment • Definition-External to individual e.g. density, structure, temperature, and most importantly “people”, etc. • Critical to behavioral change • Changes to environment • There is no all inclusive list • Engagement in the environment as a first line defense Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 171 • • • • • • • • • Basic Terms Acquire-attention, tangibles, activity Escape Avoidance Positive reinforcement (within 1 second) Negative reinforcement Extinction Punishment-positive versus negative Shaping Successive approximations Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 172 Definition of learning “These people can’t learn” Unicellular organisms learn Change in behavior not due to neurological or disease, or trauma Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 173 Interdisciplinary Team (IDT) Not headed by physician Not medical model All members equal Interactions between professionals that lead to a holistic view of the individual • Transcends the physical meeting to actual behavioral scenarios that may preclude disasters resulting from lack of communication amongst staff from varying disciplines • Integration begins at the IDT level (not as an afterthought to signing a document) • • • • Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 174 Interdisciplinary Team (IDT) An interdisciplinary approach to service delivery presupposes interaction among the disciplines. Not only are individuals from several disciplines working toward a common goal, but the team members have the additional responsibility of the group effort (Rothberg, 1981). This approach necessitates effective communication among the various individuals involved in the patient’s rehabilitation (Melvin, 1989). The team includes not only the professionals but the patient and his or her family and significant others as well. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 175 Interdisciplinary Team (IDT) Benefits and Challenges The benefits of teamwork are obvious. Team practice has led professionals to see clients and their families as whole persons, not as parts of a whole (e.g., mouths, brain, arms, legs). An appreciation of other disciplines allows professionals to accommodate larger functional goals and integrated interventions, instead of working on isolated tasks. From the patients’ and families’ point of view, it is easier to communicate with a cohesive team, rather than numerous practitioners who work in isolation. It is also less overwhelming if information related to intervention is synthesized across disciplines, rather than presented separately from each practitioner. Teamwork brings together diverse knowledge and skills and can result in quicker decision making. As a result of professional collaboration, redundancy or fragmentation of service can be reduced or eliminated, thereby increasing the cost efficiency of service. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 176 Interdisciplinary Team (IDT) But there are drawbacks to teaming as well. Certain economic and professional factors must be considered. A substantial amount of time can be spent by team members from various disciplines in communicating. Think, for example, of the salary costs of a team conference or rounds [combined salaries of professionals discussing the logo for the tee shirt]. In addition, most professionals have a productivity standard that must be met. This can impose a limitation on the time such individuals have for participating in these and other interdisciplinary activities. As a further complication, there are personnel shortages in many of the rehabilitation professions. Costs combined with staff shortages [staff turnover] can certainly affect the ability to deliver rehabilitation services under an interdisciplinary model (Melvin, 1989). Some team members and professional groups are threatened by the notion of giving up some of their autonomy to the group effort. There is a lack of confidence and trust in the opinions and decisions of individuals from other disciplines. In addition, team members’ perceptions of their respective roles and contributions to the team may clash. This may lead to individuals feeling that others are usurping their domain. This issue of territorialism can destroy a functioning team (Rothberg, 1981). In spite of these economic and professional factors, the interdisciplinary approach can improve the delivery of services to patients. All team members are working toward common goals and not in isolation. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 177 Person Centered • The person defines their wishes, hopes, dreams, and goals • Individual determines treatment planning • IDT supports their attainment • Lowes: “You can do it, we can help” • Important “to” versus important “for” • Functional assessment • PBSP • Risk Assessment Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 178 Meet people where they are… • If an individual does not attend class…don’t count them out…bring class to the individual • If an individual is determined to be at risk of suicide…don’t isolate the person…provide habilitation with the needed supports • If an individual can only point to a towel…don’t exclude them from cleaning the oven…..make that an important part of cleaning an oven • “Don’t lose the baby with the bathwater” Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 179 Choice • We all make choices all the time and they all have reality constraints/limitations/consequences • Does not mean overwhelming with continual choices • They can’t speak so how do we know • Self-determination (civil rights movement) plus choice result in Quality of Life (QOL) Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 180 Compliance vs Cooperation Compliance is the act of doing what we are told to do. Cooperation is the act of working together towards a common goal. Which is more appealing? Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 181 Compliance vs Cooperation What’s the compelling reason for someone to engage in a task? -If someone simply does not want to engage in a task, then there is no strategy that will directly result in them engaging in that task -So, how do we motivate someone, from their perspective, to engage in a task that we think is important? Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 182 Compliance vs Cooperation Focus Intervention on essential activities first -Pick and choose your “battles” very carefully -Use positive reinforcement and modeling to encourage general positive social behavior, but focus structured interventions on areas that will most affect an individual’s health, safety, and inclusion Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 183 Compliance vs Cooperation Are we expecting better behavior from the individuals we work with than we do from ourselves? -Are the standards we are holding the individuals we work with higher than what the average person living in the community is expected to follow? -What is a normal standard for behavior, hygiene, etc? -Do we allow for normal human error in how we define behavior and compliance? Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 184 Compliance vs Cooperation Focus on the positive! -Don’t define someone as “non-compliant” -For every non-compliant behavior, there are many more cooperative behaviors that a person engages in that go unnoticed. No one is completely uncooperative. -Recognize and reward cooperative behavior Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 185 Compliance vs Cooperation Are we utilizing the team process to address/resolve ongoing compliance issues that result in health and safety hazards? -Don’t get caught up in a battle of wills with the people we serve Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 186 Laying on of hands • Power/control/dominance-we don’t “command” people, we “ask” people • Getting out of harms way • PMAB/BMAP/TMAB • Mandt-Trauma Informed approach to Positive Behavior Support. The impact of trauma and how that trauma affects the neurodevelopment of children into adulthood. People use behavior to cope with their traumatic experiences and these coping mechanisms become the behavioral challenges and mental health disorders demonstrated throughout the lifespan. The neurodevelopmental model integrates the information into Positive Behavior Support plans through the use of structural assessments. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 187 Labeling • Person first language • House Bill (H.B.) 1481 • Correct: A person diagnosed with signs/symptoms of mental retardation • People are not their diagnoses • Incorrect: Mentally Retarded people Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 188 Data Collection • • • • • • • • • Foundation for assessment, diagnosis, treatment Closing the loop Changes in status prompt assessment, etc. We don’t assess to assess, we assess to treat Time taken to assess is time without treatment Data “shmatta” “Garbage in/Garbage out” Referral/Enrollment/Attendance/Engagement Frequency/Intensity or Severity/Duration Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 189 Antecedent-Behavior-Consequence (ABC) • Event recording-data on every occurrence • Time sampling-behavior occurs too frequently • ABC assessment is the core concept of what applied behavior analysis practitioners call functional assessment Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 190 Reliability • Achieve the same results when you do the same thing • “Shoot an arrow”-hit the same spot each time Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 191 Validity • Measuring what you purport to measure • “Shoot an arrow”-hit the bulls eye Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 192 Accuracy Measurement in agreement with an independent measure Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 193 Inter-Observer Agreement (IOA) Two observers see and record the same behavior Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 194 Treatment Integrity • Treatment Fidelity • Implementing the PBSP exactly as written • Conceptualize it as an experiment-once you change the conditions of the experiment it is no longer valid (you need to collect data to show either that the plan works or does not) • Mind-reading versus empiricism- “This plan won’t work” (before the fact) versus implementing the plan and collecting data to make determination after the fact • PBSP is ineffective-we need a new one (represents a giant leap in logic) • Critically analyze “all” of the elements that may be responsible for the PBSP appearing ineffective • Manipulate one variable at a time to determine impact • PBSP is a composite of many variables therefore one can only determine whether the PBSP as a whole is effective or ineffective Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 195 Suicide Risk Assessment • People that say they are going to do it are more likely to do it • Correlation of suicide risk and diagnostic categories e.g. Bipolar Affective Disorder Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 196 Risk Determination/Risk Management • Focus on risk determination • Leads to risk management/supports • A Positive Approach to Risk Requires Person Centered Thinking- “Holy Grail” • Purpose is as much about happiness of the person as about their safety • People have the right to make “bad” decisions Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 197 Proposed Causes for Increased Risk • • • • • • • • • • • • • Increased stress Diminished ability to cope Brain Dysfunction Limited mental health care Rejection Segregation Lack of control over one’s life Limited social support Limited vocational opportunities Poor self-image Limited social skills Labeling Increased rates of abuse and neglect Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 198 Communication • Verbal: spoken language, speech, scream, guttural • Non-verbal: behavioral, body language, gesture, affect, emotional tone Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 199 People are not their diagnoses, signs and symptoms, verbal/nonverbal • • • • • • • • • • • • People are not one dimensional People should be treated with dignity and respect. People have hopes and dreams and goals and wishes and trials and tribulations and troubles and losses and have diagnoses and are prescribed medications People are people are people There is no “us” and “them”…there is only “we” There is nothing intrinsic to the “population” that separates “them” from “us” The only thing that separates us is the nature of the relationship They are receiving treatment We are providing treatment If I become disabled I am still the same person, the only thing that has changed is the relationship to the provider Now I am receiving treatment rather than providing treatment Diagnosis characterizes the disorder not the person Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 200 Chronological age appropriateness • ICF/MR guideline • Not based on emotional/intellectual level appropriateness but on chronological age • Think “lollipop” rather than pacifier • Think art supplies rather than coloring book and crayons Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 201 Normalization • Teaching behavior that will result in integration into the larger world • “Normalization principle” does not mean making them normal but enabling them to live in as normal an environment as possible Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 202 Regulations for prescription of psychotropic medications • • • • • • • • • • • • • • • • Chemical restraint shall not be used excessively, as punishment, for the convenience of staff, as a substitute for habilitative program, or in quantities that interfere with a resident’s habilitation program. We don’t have anti-aggression medication We do have medication for mania and paranoia that may be manifested thru physical aggression We don’t medicate diagnoses-we medicate people who have signs/symptoms of a diagnosed disorder Or for signs/symptoms that do not meet the criteria for a disorder to be diagnosed Medications do not teach anything Goal is to teach the person how to meet the needs that the medication is meeting Best practice includes the use of medication when indicated We medicate people for specific signs/symptoms of diagnostic categories that have been applied People do not necessarily have to have a diagnosis in order to receive a psychotropic medication People are want to receive medication for anxiety when visiting the dentist without having been diagnosed with an anxiety disorder Guidelines for the Use of Psychotropic Medication Texas Administrative Code: Prescribing of Psychotropic Medication-Mental Retardation Facilities Chapter 405, Subchapter B A Behavioral Diagnostic Paradigm for Integrating Behavior-Analytic and Psychopharmacological Interventions for People with a Dual Diagnosis Integrating behavioral and pharmacological interventions in treating clients with psychiatric disorders and mental retardation Q: Can individuals receiving psychoactive medications for inappropriate behaviors have a coping training objective designed to reduce inappropriate behaviors instead of a formal BMP? A: Drugs used for control of inappropriate behavior may be used only as an integral part of an individual’s individual program plan (IPP) that is directed specifically toward the reduction of and eventual elimination of the behaviors for which the drugs are employed. However, individuals who receive psychoactive drugs for behaviors associated with a diagnosed mental disorder require an active treatment program designed to reduce, ameliorate, compensate or eliminate the psychiatric symptoms. For an individual with a diagnosed mental disorder, a program to reduce his or her psychiatric symptoms is more appropriate than a program to reduce his or her inappropriate behaviors. However, the requirement for a program to reduce psychiatric symptoms does not prevent a facility from also developing a BMP. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 203 Civil Rights-chemical restraint • Where have we failed that resulted in the use of a chemical restraint • Did we do it right but document it wrong • Did we inadequately document that the administration of a chemical was for the correct clinical reason e.g. anti-anxiety, antipsychotic, etc. • Chemical restraint does not end with the administration of the chemical versus a physical restraint • The chemical remains active within our body and has a half-life (pharmacokinetics) • Issue of “calm” as criterion for terminating a restraint is a fallacy (harm to self or others is the issue) • Is the use of chemicals “truly” more restrictive than the use of physical methods (philosophical issue) Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 204 Committee structures in place Best Practice • Positive Behavior Support Committee • Functional Assessment Review Committee • Peer Review Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 205 DOJ/Settlement Agreement-State of Texas • Public document • Anchored in violation of rights • Department of Justice (DOJ)-Primarily a federal criminal investigation and enforcement agency • Court monitoring • TN/MS/GA/TX/VA/AL/NE/CA etc. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 206 Lelsz v. Kavanaugh Case Name Lelsz v. Kavanaugh MR-TX-0001 Docket / Court 85-2462 ( N.D. Tex. ) State/Territory Texas Case Type(s) Intellectual Disability (Facility) Case Summary On November 27, 1974, the named plaintiffs filed a class action lawsuit pursuant to 42 U.S.C. § 1983 in the U.S. District Court for the Eastern District of Texas, challenging the adequacy of conditions, care, and habilitation at the Austin, Denton and Fort Worth, Texas state schools for the ... read more > On November 27, 1974, the named plaintiffs filed a class action lawsuit pursuant to 42 U.S.C. § 1983 in the U.S. District Court for the Eastern District of Texas, challenging the adequacy of conditions, care, and habilitation at the Austin, Denton and Fort Worth, Texas state schools for the mentally retarded. Plaintiffs alleged that the defendants failed to provide less restrictive community alternatives for residents, thereby effectively forcing them into large institutions. Plaintiffs alleged that the conditions at the large institutions were wholly inadequate and that they had been subjected to: diseases, neglect, excessive medication, unnecessary restraint, unsafe buildings, inadequate medical and dental care, and physical abuse from other residents and staff in violation of their constitutional rights. Plaintiffs sought declaratory and injunctive relief, including the forced closure of the Austin, Denton and Fort Worth institutions. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 207 Activities of Daily Living (ADL) Eating Bathing Grooming Leisure Recreation Money management Self administration of medication Transportation Self advocacy Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 208 Adaptive Functioning Importance of habilitation Reflects changes over time (interventions do work) Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 209 Stability of IQ The IQ will typically not increase Remains fairly stable over time-predictive validity Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 210 Behavioral Issues • Definition of behavior-anything that we do/operates thru space and time on environment • “Dead man” test-if a dead man can do it then it isn’t behavior (don’t use as target but as objective) • Will exhibit zero episodes of aggression (a dead man can do that) • Was blown over by the wind Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 211 BEHAVIORAL INTERVENTIONS Presented by: Robb Weiss, Psy. D. May 18, 2007 1:30-2:30 Fellowship Hall Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 212 Board Certified Behavior Analyst (BCBA) • Professionals who design/supervise those who design PBSPs • Exponential growth of BACB • With the governor’s signing of a bill on May 19, Tennessee became the 18th U.S. state to adopt a law to license (17 states) or certify (Ohio) practitioners of behavior analysis. • Applied Behavior Analysis-utilized with/for but not limited to people with ID/DD (Autism Spectrum Disorder) • Applicable to Mental Health-Behavior is indeed the product of complex neurochemical processes, but the behaviorenvironment interaction should not be overlooked • Foundation of practice is based on psychological principles and theories Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 213 Psychological Interventions Lack of knowledge and awareness of mental health and emotional problems experienced by people with intellectual disabilities Reluctance on the part of therapists to provide these interventions to people in this population Lack of good quality evidence to guide practice with this client group Difficulty of making an economic case in an increasingly challenging fiscal context Large-scale provision of psychological therapies for people with developmental disabilities has been slow to emerge because of previous assumptions about the suitability of this group for talking treatments (“therapeutic disdain”/”the unoffered chair”) Need for appropriate adaptations Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 214 Preparing People with Intellectual Disabilities for Psychological Treatment Client Expectations-Clients’ views and expectations of therapy predict therapeutic outcome • Outcome expectancy-People’s expectations of therapy as they enter the process may be significantly affected by the way in which therapy is offered • Role expectations-People with intellectual disabilities are likely to have a limited understanding of the role they will be expected to take in therapy • Process expectations-People with intellectual disabilities probably differ little from their nondisabled peers in their knowledge of how they are going to work with the CBT therapist The Therapeutic Relationship-Therapeutic relationships may present particular challenges to people with intellectual disabilities • Less secure attachment styles may be characterized by higher levels of interpersonal distrust, difficulty in depending on another person for support, or preoccupation with concerns about possible abandonment Client Factors-There are challenges and limits to using talk therapies such as CBT with people who have intellectual disabilities (verbal expression of thoughts and feelings) • Assessment structure (communicative ability) • Language • Recognition of emotion • Recognition of the link between activating events and emotional and behavioral consequences • Assessing understanding of the cognitive mediation of emotion Technique Factors: Preparing Therapists-”ability to foster and maintain a good therapeutic alliance, and to grasp the client’s perspective and ‘world view” for which the underlying competencies involve understanding of issues of therapeutic alliance/adapting referral pathways, clinical protocols, and individual therapy for people with lower ability and functional academic difficulties Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 215 Psychotherapy THE CO-OCCURRENCE OF mental illness with mental retardation/developmental disabilities (MR/DD) has been referred to as “dual diagnosis.” It is estimated that as many as 30 to 40 percent of MR/DD individuals are dually diagnosed. Unfortunately, when a person with MR/DD needs psychotherapy to treat the mental illness, it can be difficult to find a psychiatrist who is comfortable working with the patient. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 216 Psychotherapy There are relatively few studies focused on psychotherapeutic interventions in the mentally retarded (MR) patient. In 1982, Reiss, et al.,1 hypothesized that intellectual subnormality is such a salient and obvious feature of the patient’s presentation that accompanying emotional disturbances are overshadowed. He coined the term diagnostic overshadowing to describe this phenomenon and believes that diagnostic overshadowing leads to a failure to recognize and subsequently treat the emotional and behavioral expressions of mental illness in the developmentally disabled person. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 217 Psychotherapy Supportive psychotherapy is a form of psychotherapy in which the therapist plays an active role in helping the patient improve his or her social functioning and coping skills. The emphasis of the therapy is on improving behavior and subjective feelings rather than on achieving insight or selfunderstanding and, as such, is particularly relevant when working with the mildly MR/DD individual. Although there is limited literature on this, there are some small studies and case reports summarizing the benefits of supportive psychotherapy for this population. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 218 Psychotherapy/Counseling • • • • • • • • • Research Evidence Base Efficacy Psychotherapy for Individuals with Intellectual Disability Edited by: Robert J. Fletcher, DSW, ACSW Literature review Psychotherapy with persons with intellectual disabilities: a review of effectiveness research H. Thompson Prout and Brooke K. Browning-Findings – The paper concludes that there is evidence that psychotherapy with persons with intellectual disabilities is at least moderately effective. Further, there is evidence of effectiveness of psychotherapy for both child and adolescent, and adult populations. There is also evidence that a range of therapeutic interventions are effective and that a spectrum of problems can be addressed via psychotherapy. VOL. 5 NO. 5 2011 jADVANCES IN MENTAL HEALTH AND INTELLECTUAL DISABILITIES j PAGE 59 Practice-Group psychotherapy for trauma-related disorders in people with intellectual disabilities-Findings – This paper establishes the inverse relationship between the higher-than-average rates of trauma and interpersonal violence in the ID population, co-occurring with lower-than-average access to treatment, and lower-than-average treatment model development for this population. Further, this paper provides a description of a theoretically based therapeutic intervention with preliminary research efficacy. VOL. 5 NO. 5 2011 jADVANCES IN MENTAL HEALTH AND INTELLECTUAL DISABILITIES j PAGE 45 Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 219 Counseling • • • • • • • • • • • • • • • • • • • • • • Anger Management Boundaries Community Prep Competency Restoration - The goal is to restore, to trial competency, those individuals who are court-ordered for admission to SGSSLC under Article 46B of the Texas Code of Criminal Procedure (adults) or under Chapter 55 of the Texas Statutes Family Code (minors). Depending on the order, the adult admissions have up to 120 days to receive training that may restore their competency to stand trial. The minors who are admitted have up to 90 days to receive training to support them becoming fit to proceed to trial. Conflict Resolution Developing a Positive Identity Dialectic Behavior Therapy -The goal of DBT is to help individuals enrolled become more present, mindful, and at peace with the world. Participants in the group will learn tools and techniques for regaining control of one’s behaviors, to help stop self-harmful behaviors, and to develop healthy coping mechanisms and relationships. Other important components are learning to fully experience emotions and to become reintegrated with and connected to one’s world. Finally, members will work to take steps to make their lives more meaningful. Emotions Empathy and Acceptance Goal Setting Healthy Relationships Individual Counseling Overcoming Obstacles Owning My Future Positive Self-Talk Process Therapy - The goal of this group will be to increase emotional awareness and relational understanding between self and others. This group will focus on the here-and-now and learn to become more aware of their immediate surroundings and on one’s thoughts, emotions, and behaviors. Stress Management Self-Determination / Self-Advocacy Self-Empowerment Self-Esteem Thinking Errors Sex Offender Treatment Program (SOTP)-not psychosexual program Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 220 Dialectical Behavior Therapy (DBT) (Not diabolical behavior therapy) • Staff are certified in DBT • • Not Diabolical Behavior Therapy Dialectical Behavior Therapy (DBT), developed by Marsha Linehan, Ph.D., ABPP, at the University of Washington, is a comprehensive cognitive-behavioral treatment that was originally developed to treat chronically suicidal individuals suffering from borderline personality disorder (BPD). DBT has been found especially effective for those with suicidal and other multiply occurring severely dysfunctional behaviors. Research has shown DBT to be effective in reducing suicidal behavior, psychiatric hospitalization, treatment dropout, substance abuse, anger, and interpersonal difficulties. • Dr. Marsha Linehan-“ask me to tell you about the tale of the hotel room switch” • Core Mindfulness (awareness) • Emotion Regulation (understanding emotions – understanding YOUR emotions, decreasing your suffering, changing your emotion – opposite emotion, increasing positive emotions, using distress tolerance) • • • Interpersonal Effectiveness (dealing with others, getting your needs met, taking care of yourself and others) Distress Tolerance (using distraction techniques: activities, self-soothing, observing breathing) Dialectical Behavior Therapy (DBT) is a voluntary treatment designed specifically for individuals with self-harming behaviors, such as self-cutting, suicidal thoughts, urges to suicide, and suicide attempts. Many clients with these behaviors meet criteria for a disorder called Borderline Personality Disorder (BPD). It is not unusual for individuals diagnosed with BPD to also struggle with other problems- depression, bipolar disorder, post-traumatic stress disorder, anxiety, eating disorders, or alcohol and drug problems. DBT is a modification of cognitive behavioral therapy (CBT) developed by Marsha Linehan, Ph.D. who first tried applying standard CBT to people who engaged in self-injury, made suicide attempts, and struggled with out of control emotions. When CBT did not work as well as she thought it would, Dr. Linehan and her research team added other types of techniques until they developed a treatment that worked better. DBT is an empirically-supported treatment with research originally focusing on women diagnosed with BPD, but is now being researched in other populations including persons diagnosed with Antisocial Personality Disorder, depression, bipolar disorder, as well as numerous behavioral disorders. Four important core skill areas are taught including Mindfulness, Interpersonal Effectiveness, Emotion Regulation, and Distress Tolerance. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 221 Anger Control Problems • • • • • • • • • • • • • • • • • • • • • • • • • Anger is a normal human emotion and is hardwired for survival It has considerable adaptive value, although there are sociocultural variations in the manner in which it is expressed Anger can help maintain one’s self –esteem and dignity when confronted by provocation, insult or unjust treatment In the face of danger, anger can help individuals to mobilize psychological resources and prime behaviors to deal with threat It can communicate negative sentiment to others, potentiate the ability to face up to and redress grievances, and boost perseverance and determination to overcome obstacles to goal attainment Recurrent and poorly controlled anger, however, adversely affects emotional and physical health and is disruptive of social relationships that sustain personal well-being It is commonly observed in a range of mental health and emotional problems, including personality, psychosomatic, and conduct disorders, schizophrenia, and bipolar mood and organic disorders, and in conditions resulting from trauma The central characteristic of anger in the context of mental health disorders is that it is dysregulated-that is, its activation, expression, and ongoing experience occur without appropriate controls The life experiences of many people with intellectual disabilities, from childhood onward, are conducive to the activation of anger The environmental settings and social circumstances in which many such people live and work are intrinsically constraining, potentially threatening, unrewarding, and limited in satisfaction Recurrent thwarting of physical, emotional, and interpersonal needs can potentiate anger activation Cognitive deficits can readily impair effective coping with frustrating or aversive events, and impoverished support systems limit problem-solving options While it is neither necessary nor sufficient for aggression to occur, anger has been found to predict physical aggression by psychiatric hospital patients prior to admission, in the hospital, and subsequently in the community following discharge It has been shown to be strongly associated with and predictive of violence in adults with intellectual disabilities and histories of aggression and offending There are mixed reviews on the efficacy of anti-psychotic drugs for aggression Proximity bias-people generally describe (and ascribe) anger responses to events that are temporally close Consider more distal events and setting conditions that have relevance to recent anger outbursts Excitation transfer-previous provoking events that did not result in an angry reaction at the time can leave physiological and psychological residues that linger and contribute to and intensify a person’s response to more recent events Given its strong association with aggression and predictive relationship with violence, anger is a legitimate therapeutic target for people with intellectual disabilities who are aggressive and potentially violent Engaging seriously angry people in therapy is difficult as they tend to be treatment avoidant Attempts to achieve clinical change can be undermined by the adaptive functions of anger and by its embeddedness in the client’s sense of self- and personal worth Angry thinking and behavior that is strongly attached to a client’s personal identity is not easily or readily relinquished Deficits in cognitive functioning can add to the challenges of anger regulation from the standpoint of both clients and those who seek help them therapeutically Despite the ubiquitous use of medications to reduce aggression in people with intellectual disabilities, there is no conclusive evidence to support their use as first-line treatments Given their lack of specificity and variable effects, including dampening of adaptive behavior, routine use of these compounds to treat aggression is not thought to be justified Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 222 www.cms.gov • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • Centers for Medicare and Medicaid Services http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/som107ap_j_intermcare.pdf www.hhs.gov Shortcut to: http://www.in.gov/fssa/files/ICFMR_Standards_100-489.pdf State Operations Manual Appendix J - Guidance to Surveyors: Intermediate Care Facilities for Persons With Mental Retardation (Rev. 94, Issued: 12- 06- 13, Effective: 12- 06-13, Implementation: 12- 06-13) This revised ICF/MR survey protocol is to assist surveyors to focus attention on the outcomes of individualized active treatment services. The Centers for Medicare & Medicaid Services (CMS) intends the revised survey process to be less resource intensive for providers who consistently demonstrate compliance with the regulations. The survey process is based on the October 3, 1988, regulation and is applicable to all ICFs/MR, regardless of size. In 1988, when the current ICF/MR regulation was implemented, it was viewed as a great step forward in promoting a focus on the actual outcomes experienced by consumers, rather than on the policies, procedures and paperwork of the facility. Since that time there has been an evolution on thinking in both the field of developmental disabilities (DD) and in the field of quality assurance (QA). The field of DD is increasingly emphasizing supporting individuals in their own homes and communities, rather than placing people in facilities. In addition services in virtually all States are placing increased emphasis on person-centered planning and person centered services that focus on the preferences, goals and aspirations of each individual and on supporting them in reaching their personal goals. The field of QA is placing increased emphasis on outcomes related to choice, control, relationships, community inclusion, and satisfaction with life, as well as satisfaction with services and supports. Many QA systems also include organizational self-assessment and continuous quality and advocates that the ICF/MR regulation and oversight process is too prescriptive and cumbersome, and should be altered to reflect newer values of quality enhancement and continuous quality improvement. 2015 Changes to the ICF/IID Interpretive Guidelines H&W Independent Solutions www.hwisolutions.com Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 223 CMMS Centers for Medicare and Medicaid “Title XIX”: ICF-MR Medicaid survey DATE: January 16, 2015 TO: State Survey Agency Directors FROM: Director Survey and Certification Group SUBJECT: Advance Copy of Intermediate Care Facilities for Individuals with Intellectual Disabilities (ICF/IID) State Operations Manual (SOM) Appendix J - Interpretive Guidelines and new Exhibit Memorandum Summary Guidance Updated: The Centers for Medicare & Medicaid Services (CMS) has revised the ICF/IID SOM Appendix J – Interpretive Guidelines (IGs) to clarify the intent of the Conditions of Participation (CoPs) for ICF/IID as well as represent current standards of practice in the field. In addition, the probes and procedures have been removed from the IGs and placed into an Exhibit in the SOM. On October 3, 1988, the CMS published the Final Rule for the CoPs for ICF/IID, 42 CFR 483, Subpart I. The Final Rule establishes that a facility may receive reimbursement only for the cost of care of individuals classified as eligible for the ICF/IID level of care who are receiving active treatment. Facility compliance with the CoPs and standards are determined in the context of individual experiences within the facility and whether individuals are receiving needed active treatment services. These associated Interpretive Guidelines have been revised to provide a concise clarification of the regulation intent and represent current standards of practice in the field of ICF/IID. In addition, the probes and procedures have been removed from the previous guidelines and placed into an Exhibit in the SOM in the event that additional clarification beyond the guidelines is needed. The revised ICF/IID guidelines and the new SOM Exhibit are attached to this correspondence. These are the regulatory standards that guide our practice as we accept their funds. We don’t receive funds to keep people “busy”. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 224 Functional Assessment Preventive Issues • Assess basic “preventive behavioral support” procedures are in place (availability of reinforcers, availability of activities, extent to which difficult behaviors are inadvertently reinforced. • Assess and address potential medical or physical conditions that may be influencing challenging behaviors. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 225 Functional Assessment versus Functional Analysis Not limited to physical and verbal aggression and SIB Subject to all behavior Functional Assessment-Naturalistic observation Functional Analysis-Manipulation of variables (Ethical/Legal Issues) • Integration of ID with Mental Illness (setting event) • SIB-not a topography but an outcome based on injury • Constipation does not cause aggression (the physical pain from constipation does) • • • • Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 226 Consequences versus Punishment • • • • • • • • • • • • Proof of necessity-did we implement every conceivable less intrusive treatment intervention and did we do it properly (treatment integrity), continuously, and consistently, and do we have the data to verify it Proof of efficacy-data (treatment integrity, reliability, IOA) Consequence-follows a given behavior Punishment-follows a given behavior and results in the diminution of the behavior that precedes it Punishment is not intrinsic to the act, but to the consequence of the act Legal issues Ethical issues Moral issues Clinical issues Social implications-we are funded by tax dollars so we are accountable to the public Standardization Best practice Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 227 Punishment-Problems and Negative Side Effects It has been clearly and repeatedly demonstrated that punishment can very effectively be used to control behavior. So, why do behaviorists usually warn against using it? Simply because we can almost always control behavior just as effectively by using reinforcement as by using punishment, and without having to put up with the problems and negative side effects of punishment. If we wish to stop a behavior that is already occurring, we can usually do so by simply eliminating the reinforcement for the behavior — a process we call extinction. The following is only a partial list of the problems and negative side effects resulting from the use of punishment to control behavior. Others could easily be added. The following most directly apply to corporal punishment, but should also be considered when contemplating other forms of punishment. • • • • • • • • • • • • • • 1. PUNISHMENT OFTEN FAILS TO STOP, AND CAN EVEN INCREASE THE OCCURRENCE OF, THE UNDESIRED RESPONSE. Since attention is one of the most potent rewards available, and since it is difficult to punish without paying attention to the offender, punishing may serve more as a reward than as a punishment. 2. PUNISHMENT AROUSES STRONG EMOTIONAL RESPONSES THAT MAY GENERALIZE. Once the strong emotional responses are aroused the degree and direction of generalization is largely uncontrollable. The result may be excessive anxiety, apprehension, guilt, and self-punishment. 3. USING PUNISHMENT MODELS AGGRESSION. The meaning of "social power is exemplified. 4. INTERNAL CONTROL OF BEHAVIOR IS NOT LEARNED. The offender may learn to inhibit the punished response during surveillance, but once surveillance ends there is no internal control mechanism to continue inhibiting the behavior. 5. PUNISHMENT CAN EASILY BECOME ABUSE. Most parents who abuse children do not intend to do the damage they inflict. Most of the damage and injury occurs when the parent loses control, and goes beyond the boundaries of reasonable behavior. 6. PAIN IS STRONGLY ASSOCIATED WITH AGGRESSION. The pain of punishment often leads to a display of aggression against either the source of the pain or, in some cases, an innocent scapegoat. 7. PUNISHMENT WORKS BEST WHEN IT OCCURS EVERY TIME. While reward works best when given on an intermittent basis, punishment works best when a continuous basis. The degree of vigilance required to constantly monitor behavior so that every occurrence of the undesired behavior can be punished is rarely possible. The undesired behavior is, therefore, intermittently reinforced when it is not punished, and the behavior continues. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 228 Punishment • Punitive • Convenience Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 229 Reduction of Challenging Behavior • Time Out is a procedure in which an individual’s opportunity to access reinforcement is removed or prevented contingent on the occurrence of an undesired target behavior. (What that means is that “time out” refers to a time without reinforcement for a behavior after that behavior occurs. • Non-restrictive time out is a type of exclusionary time out in which the person is removed from the setting in which the reinforcers are available. • Restrictive time out occurs when we put people into the time out rooms and bar their egress, is also an exclusionary time out • Response cost • Extinction Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 230 Habilitation versus Rehabilitation • Habilitation: Learning/teaching that which has not yet been learned • Rehabilitation: Re-learning/teaching skill that has been lost (psycho-social model) Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 231 Active Treatment • • • • • • Active treatment is the continuous, aggressive, and consistent implementation of an individualized program plan, based on interdisciplinary evaluations and assessments, which is aimed at the individual’s recovery and expedient transition out of the hospital. This means both the acquisition of skills and behaviors that promote recovery and the prevention of the loss of these skills. Active treatment assumes greater “action” on behalf of the individual and those providing treatment. Except for normal rhythm of life rest cycles or medical conditions requiring inactivity, it holds to the premise that the individual should not have periods of “down time.” Active treatment does not include services to maintain generally independent individuals who are able to function with little supervision or in the absence of a continuous active treatment program. 24/7 Formal Informal Teach new skills and/or reduce regression of skills We don’t receive funds to keep people occupied or busy Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 232 Token Economy • • • • A token economy is a system of behavior modification based on the systematic positive reinforcement of target behavior. The reinforcers are symbols or tokens that can be exchanged for other reinforcers. Token economy is based on the principles of operant conditioning and can be situated within applied behavior analysis. Tokens have to be used as reinforcers. A token is an object or symbol that can be exchanged for material reinforcers, services or privileges (back-up reinforcers). In applied settings a wide range of tokens are being used: coins, checkmarks, images of small suns, points on a counter. These things are worthless. Their value lies in the fact that they can be exchanged for valued things. Technically speaking tokens aren’t primary reinforcers, but secondary or learned reinforcers. Lots of research has been done on token reinforcement, including animal studies. Token economy is also being applied in settings for adults with developmental disabilities. Target behaviors can be all kinds of social behavior and self care, or the decreasing of inappropriate or disruptive behavior. Not to be used as a “one size fits all” technique. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 233 Industrial Organizational (I/O) Psychology • System issues • Clinical issues • Historical standard degree Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 234 Positive Behavior Supports • Setting the person up to succeed through antecedent structural modification • “Efficacy” of a PBSP refers to clinical setting or research setting • “Effectiveness” is the measure in realistic settings or in vivo setting Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 235 Special Supervision • It is not treatment • It does not ensure the effective implementation of the PBSP • Critical thinking is imperative in applying levels of supervision (why is it being applied, why is the particular level being applied, why is the frequency being applied) • The fading/discontinuation should be contingent upon the demonstration of a learned behavior and not simply the absence of a challenging behavior for a given period of time Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 236 Role/Impact of psychotropic medication • For example-effect on ability to glean reinforcement • Setting event for the establishment of behavioral/environmental interventions • Specificity in ID/DD • Does not treat ID/DD • Does treat signs/symptoms • Who in fact are we treating: the individual or the fear and anxiety of the treating professional about the individual • Research does not support differences in CNS Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 237 PBSP Competence • Didactic • Role-modeling/role-playing • In-vivo Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 238 Functional Assessment versus Structural Assessment • Teaching person to meet their needs in more socially acceptable ways • Functional-consequence • Structural-antecedent • Antecedent versus precursors (behaviors that the individual engaged in that often predicted the target behavior) Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 239 “It’s (not) all for attention” • Hanley, Iwata, and McCord (2003) reported escape as the most frequent function of challenging behaviors. Leading function of problem behavior: • 34.2% - Escape • 25.3% - Attention (may be a disguising factor) • 15.8% - Automatic • 10.1% - Tangible • 14.6% - Multiple Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 240 Functional versus Topographical • Topographical Replacement Behavior-historic: replacing one behavior with another e.g. sitting on hands to prevent physical aggression • Functional Replacement Behavior-current: treatment of behavior problems includes the specific reinforcement of appropriate behavior that serves the same function(s) served by the problem behavior e.g. determine function of physical aggression and then teach individual a new way to meet that function in a more socially acceptable way e.g. the social relevance of the behavior • Verbal praise should only be utilized when it matches the identified function of the problematic behavior (otherwise it’s like chicken soup-it can’t hurt) • DSM-structural/descriptive not functional • DSM focus is on the what of behavior, not the what for or the function of behavior Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 241 Medication versus Behavioral • Behavioral-much more labor intensive than medication • Best practice demands the utilization of medication when clinically indicated • Not black or white issue • No medication for Autistic Spectrum Disorders (ASD) • Pharmacotherapy is for associated behavioral and emotional sequelae Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 242 Quality Assurance (QA) Quality Improvement (QI) • Outdated/updated/quantity/quality: FAR/PBSP/Progress Note/APES/PBSP Competency Assessment/BSMT/Sessions • New admission: FAR/PBSP/APES/Full Psychological Evaluations • Identifying problems • Root Cause Analysis (RCA)-The 5 Whys • Recommendations • Action Plan-Management strategy • Corrective Action Plan (CAP)-Based on analysis of data Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 243 Specificity of knowledge base • Most professionals don’t understand ID/DD • Tendency to overly pathologize ID/DD issues via Axis I which inevitably leads to medication therapy Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 244 Psychologists and Psychiatristcompetencies in ID/DD • • • • • • • • • • Comorbidity of Mental Illness and Mental Retardation Dual Diagnosis-Psychiatric Disorder and ID (not substance abuse disorder) Accurately diagnosing mental disorders in the context of a cognitive/communication/developmental disability Talking to an imaginary friend is not a hallucination Talking in an odd voice is not diagnostic of Multiple Personality Disorder (MPD) Wanting to become a fireman may be considered delusional but for an individual functioning at the 3-5 year developmental level it would not (impacts diagnosis and treatment) Crying/grieving/mourning the loss of someone close does not warrant a psychiatric consult Throwing a tantrum does not a manic make It is necessary but not sufficient to have signs/symptoms-but without impacting ability to function on a daily basis there is no basis for diagnosing or treating Psychiatric diagnostic assessment must be comprehensive and multifocal rather than a medication evaluation based on the choice of drug to suppress a disruptive behavior Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 245 Behavior Graphs • Importance cannot be overstated • It is the basis for determining efficacy of treatment and/or need for revisions to treatment, both behavioral and chemical • It is the basis for determining the impact of environmental events on behavior • It reduces the likelihood of attributing a psychiatric diagnosis to changes in behavior • Placing a label on an individual does not explain the foundation for the behavior, it is simply calling it something else and is circular e.g. he hit me because he is psychotic. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 246 Trauma Informed Care-Karyn Harvey, Ph. D. • • • • • • • • • • • • • Based upon assumption that individuals with ID/DD have experienced some form of trauma in their lives Trauma-Informed Behavioral Interventions with Individuals with Intellectual Disabilities is based on the concept that most such individuals have experienced trauma and are exhibiting behavioral responses to that trauma. Trauma is under-diagnosed Why trauma informed care? Individuals with intellectual disabilities are at much higher risk than the general population of abuse, neglect, and the associated trauma. Research indicates that: Individuals with disabilities are 4 to 10 times as likely to be victimized as individuals without disabilities. Individuals with cognitive disabilities experience the highest risk of violent victimization. Children with intellectual disabilities or behavior disorders are at an increased risk for neglect, physical abuse, and sexual abuse as compared to children with other types of disabilities. Children with behavioral and neurological disorders are physically abused at rates 2 to 7.3 times higher than children without disabilities. Adults with developmental disabilities are at risk of being physically or sexually assaulted at rates 4 to 10 times greater than other adults. Behaviors caused by trauma are often attributed solely to the disability with minimal attention to the individual’s mental health. As defined by the Substance Abuse and Mental Health Services Administration (SAMHSA), trauma-informed care engages people with histories of trauma in a way that recognizes the presence of trauma symptoms and acknowledges the role that trauma has played in their lives. Understanding the impact of trauma on behavior and using trauma-informed strategies can help reduce the use of restraint on individuals with intellectual disabilities in both facility and community settings. Only by understanding that trauma can be the root cause of behavior challenges can service providers help to heal past pain and provide support that avoids re-traumatization. Trauma Informed Care to Effectively Reduce the Use of Restraint to Manage Challenging Behaviors of Individuals with Intellectual Disabilities. People are greater than the sum of their behavior The definition of trauma has been expanded thus greater interest in this area Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 247 Trauma Informed Care-Karyn Harvey, Ph. D. Update on Quality Supports By Karyn Harvey, PhD, Assistant Executive Director of Quality Supports What does it feel like to have an intellectual and developmental disabilities (I/DD)? On one level, the answer to that question is different for each person. No two people have the same experience. On the other hand, however, there are some universalities. One is that having an intellectual or developmental disability means experiencing a certain degree of social trauma: bullying, exclusion and/or rejection. It may also mean experiencing a significant degree of loneliness and isolation. Recent studies have shown the effects of social exclusion and/or rejection on the brain. In one particular study, participants were included in a game and then deliberately excluded. Their brains were connected to electrodes that could then show which part of the brain was stimulated and thus active during the experience. When participants were excluded, all of their brains fired in the anterior cingulate cortex. This is the part of our brain that fires when we feel physical pain. They experienced exclusion from a simple game as physical pain. Imagine what people who have been rejected over and over again have experienced. The Quality Supports Division at The Arc Baltimore has been attempting to reduce the pain and suffering due to exclusion, rejection and loneliness through increased in-house therapy from the psychology department, trauma and sensitivity training for Arc staff, and finally, through involvement in our Connections program. Science 10 October 2003: Vol. 302. no. 5643, pp. 290 - 292 DOI: 10.1126/science.1089134 REPORTS Does Rejection Hurt? An fMRI Study of Social Exclusion Naomi I. Eisenberger,1* Matthew D. Lieberman,1 Kipling D. Williams2 A neuroimaging study examined the neural correlates of social exclusion and tested the hypothesis that the brain bases of social pain are similar to those of physical pain. Participants were scanned while playing a virtual ball-tossing game in which they were ultimately excluded. Paralleling results from physical pain studies, the anterior cingulate cortex (ACC) was more active during exclusion than during inclusion and correlated positively with self-reported distress. Right ventral prefrontal cortex (RVPFC) was active during exclusion and correlated negatively with self-reported distress. ACC changes mediated the RVPFC-distress correlation, suggesting that RVPFC regulates the distress of social exclusion by disrupting ACC activity. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 248 Trauma Informed Care-Karyn Harvey, Ph. D. H.B. No. 2789 A BILL TO BE ENTITLED AN ACT relating to trauma-informed care training for certain employees of state supported living centers and intermediate care facilities. BE IT ENACTED BY THE LEGISLATURE OF THE STATE OF TEXAS: SECTION 1. Subchapter D, Chapter 161, Human Resources Code, is amended by adding Section 161.088 to read as follows: Sec. 161.088. TRAUMA-INFORMED CARE TRAINING. (a) The department shall develop or adopt trauma-informed care training for employees who work directly with individuals with intellectual and developmental disabilities in state supported living centers and intermediate care facilities. The executive commissioner by rule shall require new employees to complete the training before working with individuals with intellectual and developmental disabilities and shall require all employees to complete an annual refresher training course. (b) The training required under this section may be provided through an Internet website. SECTION 2. This Act takes effect September 1, 2015. • • • • Trauma-Informed care: Purpose: provide information on signs and symptoms of trauma; how trauma affects development and behavior, and specifically the widespread impact it has on people with intellectual and developmental disabilities and co-occurring disorders; include strategies for using trauma-informed practices for people with an intellectual disability and co-occurring disorders; include both individual-centered and system-centered information; provide information on how to support and empower individuals and prevent re-traumatization; include information on developing trauma sensitive environments and interventions that emphasize physical, psychological and emotional safety for both individuals and DSWs. Short Term Objective: Participants will be able to identify signs and symptoms of trauma and express the importance of understanding trauma when dealing with individuals with challenging behaviors. Long Term Objective: Participants will be able to assist in creating a trauma informed care environment and interventions where they work. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 249 Peer Review • • • • Internal External Individual-based Home-larger environment Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 250 Psychological Evaluation • • • • IQ Adaptive Ability Psychopathology Importance of the results in the person’s life that include though not limited to potentially affecting supports, services, waivers, etc. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 251 PBSP (BSP/BMP/WTP) format/instructions • • • • • • • • • The “genius” in creating a PBSP that is understood by staff will be more readily implemented If we continue to do the same thing and expect a change in behavior of another individual we are engaging in scapegoating-definition of insanity The change in behavior begins with “us” via the intervention section to effect change in the individual Our own behavior is all that we have control of-we can set the stage for behavioral change but ultimately cannot control another human being Skill Acquisition Program (SAP)-teaching the component parts of a behavior (motivational issue if behavior occurs at a low frequency) Determination as to existence of a given behavior in person’s repertoire vis a vis baseline or at a low level of frequency In the absence of data/baseline the default is to assume the behavior is not evident in the behavioral repertoire and thus needs to be trained via a SAP Baseline-pre-treatment Present level of functioning-ongoing treatment Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 252 Positive Behavior Support Plan (PBSP) • • • • • • • • • • • • • • • • • • Rationale/purpose of the plan Description of potential function (s) of behavior History of prior intervention strategies and outcomes Consideration of medical, psychiatric, and healthcare issues Operational definitions of target behaviors (challenging behavior) Operational definitions of functional replacement behavior Behavioral objectives for one or more target behaviors Behavioral objectives for one or more replacement behaviors Strategies/Skill Acquisition Programs (SAPs) to promote the acquisition or occurrence of replacement or alternative behavior (or stated why not) Baseline data for one or more target behavior Antecedent-based or preventative strategies Consequence-based strategies (what to do when behavior occurred) The use of positive reinforcement Descriptions of data collection procedures Signed and dated Environmental Supports Prompt the replacement behavior as early in the antecedent behavior chain as possible then provide reinforcement Written as instructions to staff e.g. “do this” or “don’t do this” Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 253 Data and monitoring progress of PBSP • • • • • Scan Data Cards Behavior Data Sheets Is PBSP effective Is PBSP ineffective Progress (or lack thereof) captured in progress note Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 254 Approval & Consent PBSP • Practice-approval (not consent) • Rights-approval (not consent) • Consent-obtained from individual or guardian-Legally Authorized Representative (LAR) • Consent for medication-must state clearly a reason for administering the drug and a legitimate benefit anticipated. • “Hearing voices” does not necessarily equate to experiencing hallucinations, and experiencing hallucinations does not justify the risks associated with antipsychotic drugs unless there is some impairment of daily functioning associated with the experiencing of hallucinations. • The reason given for administering a psychotropic drug should refer to the problem or impairment the symptom(s) creates for the client. • If we can’t articulate how a client is being harmed or impaired by a symptom, then we can’t justify a drug to address that symptom. • Risk:Benefit Analysis Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 255 Guidelines • Behavior Analysis & Programming Guidelines • Guidelines for Supporting Adults with Challenging Behaviors in Community Settings • Guidelines for Providing Behavior Supports in the Adolescent Specialty Treatment Unit • A Guide to Behavior Supports Planning and Implementation Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 256 Systematic Desensitization • • • • Medical/Dental procedure/Clinic appointments A behavioral approach in its’ own right Predicated on fear/anxiety Utilized for procedure that requires pre-treatment sedation that would not ordinarily require sedation in the “community” e.g. cleaning, etc. [TIVA is Total Intra Venous Anaesthesia] • Progressive muscle relaxation • Alternatives: A Review Of Non-Pharmacologic Approaches To Increasing The Cooperation Of Patients With Special Needs To Inherently Unpleasant Dental Procedures Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 257 Methods to develop toleration for medical and dental procedures in order to decrease the need for use of restraint and sedation-I • • • • • The PST should develop an individualized approach to increase toleration for medical and dental procedures by selecting applicable methods from the following. A single method or a combination of methods may be appropriate, dependent on the individual. Some of the methods are practical for appointments at SGSS and away from SGSS. Some are practical only for appointments at SGSS. Sensitivity to the attributes, emotions, past history, and capabilities of the individual is crucial. Behavioral rehearsal – This is reinforced practice under simulated conditions. Example: Taking the individual to the exam or treatment room many times when it is not in use. Greeting and talking with a doctor, nurse, dentist, and/or hygienist at the site. Sitting in the dental chair or sitting or lying on the exam table. Going through a simulation of what is expected of the individual during the procedure. Positively reinforcing the individual many times during the process with something the individual is known to find highly reinforcing. No medical or dental procedures are performed. Communication training – This involves teaching the individual communication skills to use prior to or during medical or dental procedures, such as teaching the individual to communicate in some manner if pain or discomfort starts during a medical or dental procedure. Contracting – entering into an agreement with the individual that following the medical or dental procedure a reinforcer that is highly desired by the individual will be provided Counseling – Counseling strategies such as: finding out the individual’s immediate goals and explaining how that going through with the procedure makes achieving his/her goals possible, talking about fears and discomfort related to the procedure and assisting the individual to work through them, educating the individual about the procedure and what is to be expected, having the individual meet and talk with someone else who has had the procedure done, and/or assisting the individual in reaching an understanding of the benefits of the procedure and the risks of not taking having the procedure done. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 258 Methods • • • • Personal support – If permitted, someone who is trusted or liked by, or who is important to the individual, encourages the individual and provides reassurance during the procedure. To reduce the potential for acting out, the authority structure in the situation must be clear to the individual receiving services. If a staff person or other support person will be with the individual during the exam or treatment, at the initiation of the appointment the dentist or physician should direct the staff or support person to do a few simple brief tasks. The staff or support person should immediately and cooperatively follow the directions. This makes the authority structure clear to the individual, and also provides a model to follow. TLC provided by the medical or dental staff prior to and during a procedure are also means of supporting the individual. Positive reinforcement – The doctor, nurse, dentist, and/or dental hygienist gives the individual something that is known to be highly reinforcing to the individual each time the individual has a procedure completed, or as soon as possible following the procedure. Priming – preparing an individual in advance by talking with the individual (possibly many times) about the medical or dental procedure in a relaxed and informal manner Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 259 Methods • • • • Relaxation therapy – teaching the individual methods to reduce tension and to induce relaxation, such as systematic tensing and releasing of different muscle groups. Relaxed, slow, deep breathing may be also used. The staff person teaching the individual should also describe pleasant and calming situations in a soothing voice. The intent is to teach the individual to recognize physical tension, to experience deep muscle relaxation, and/or to learn how to physically relax. Trigger words such as “relax” may be paired with deep relaxation. The trigger may be used by the individual to begin relaxation upon self-recognition of physical tension if possible, or by the dentist, doctor, or other staff person to assist the individual to begin relaxing when signs of tension are observed during the procedure. Role playing – while being observed by the individual, a staff member acts as if he/she is going through the steps of the procedure and is heavily reinforced. Preferably this is done on site. The individual may need to be prompted to give attention to what is occurring. Self-calming skills – teaching the individual self-calming skills to use during a medical or dental procedure such as focusing on a central point, repeating to self over and over to be calm or an encouraging verse, focused breathing, remembering pleasant things, or listening to music known to be calming to the individual. Shaping – This is systematically reinforcing successive approximations to cooperation with the procedure. An individual may immediately react to the exam or treatment room due to past experience and may try to escape or resist. This approach can involve many steps that lead closer and closer to cooperation with the procedure, such as the following scenario: Taking the individual many times as close to the exam or treatment room as the individual will tolerate and positively reinforcing the individual with something the individual is known to find reinforcing. Once the individual appears to tolerate that step of the process, having the individual go closer to the exam or treatment room prior to providing the positive reinforcement. Additional steps may include entering the exam room, standing in the exam room, sitting in the exam room, touching the dental chair or exam table, sitting on the dental chair or exam table, laying on the exam table, staying seated or laying down with the dentist or doctor standing close to the individual, staying seated or laying down with the dentist or doctor providing physical support, opening the mouth when requested, remaining in place when instruments are exposed, removal of applicable clothing at appropriate times. The actual process likely will not require the number of discrete steps described in the example. The type and number of steps, and the number of times the steps should be repeated and reinforced, should be tailored to the individual. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 260 Methods Systematic desensitization - The first step in this method is to teach the individual to relax; then the individual is exposed to the medical or dental procedure degrees at a time while being prompted to remain relaxed. For example, the staff person providing the desensitization training presents the least anxiety provoking description of the dental or medical situation and asks the individual to imagine himself or herself in that circumstance. The staff person prompts use of the relaxation skills to remain relaxed. If the individual feels anxious, the same item is repeated until the individual can remain relaxed for several trials. Each next higher degree of exposure is progressively presented in the same manner, including actual on site exposure. A variation may involve accustoming the individual to less intrusive procedures, such as dental cleanings, prior to more invasive dental work. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 261 The NADD Accreditation/Certification Program: Standards for Quality Services • 3 Separate but interrelated competency-based quality standards programs: • Certification for direct support professionals (DSP) • Certification for clinicians • Accreditation for programs • Joint Commission is not for ICF/IIDs Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 262 • • • • • • • • Offenders With Developmental Disabilities People with developmental disabilities who offend pose significant philosophical, ethical, and pragmatic dilemnas for the criminal justice system and developmental disabilities services Despite reports of increased frequency of offending among people with developmental disabilities, it is generally believed that there is no conclusive evidence of a general causal link The distinction between behavioral disorder and offending behavior is elusive and depends on individual, service, and societal factors People with developmental disabilities are more likely to be disadvantaged by the criminal justice process because of issues of competence in following and understanding necessary legal processes They are also known to admit to crimes they have not committed because of acquiesence and are considered unreliable witnesses when they themselves have become victims of crime A number of people with developmental disabilities are inappropriately placed in the penal system or in conditions of higher security than they actually need The capital punishment of people with developmental disabilities in some countries continues to provoke public outcry and passionate debate Treatment and rehabilitative programs based on behavioral, educational, and cognitive models have been reported, with length of treatment appearing as a significant positive prognostic factor in reducing recidivistic reoffending Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 263 Sex Offenders Sex Offender Treatment Program (SOTP) Licensed Sex Offender Treatment Professional (LSOTP) Based on the Cognitive-Behavioral Approach, the Texas Penal Code, the best practices in the field of sex offender treatment, and the standards of the Council on Sex Offender Treatment for the State of Texas, the purpose of the Sex Offender Treatment Program is to ensure that sex offender treatment by a Licensed Sex Offender Treatment Provider (LSOTP) is provided to individuals who have been adjudicated by the courts as registered sex offenders or individuals who have engaged in sexual offending behaviors and who reside in State Supported Living Centers and the ICF-MR component of the San Angelo State Supported Living Center (SgSSLC). This program parallels community sex offender treatment. Treatment is to ensure the safety of the community as well as the individual in the program. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 264 All behavior is communicative • • • • • What is the individual communicating How do we choose to respond Individual bangs their head-mittens on hands What is the individual communicating What is our intervention Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 265 All behavior has function • This is a “given” that guides assessment and treatment • Goal is to teach individual a better way to meet the function thru differential reinforcement Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 266 Stability of MR diagnosis Developmental window Adulthood Exceptions utilized in changing diagnosis Diagnosis of MR is in question e.g. inaccurately diagnosed • Level of mental retardation is typically not changed after criterion age of 18 • Mental Retardation is not necessarily lifelong • After age 18 a diagnosis of Dementia may be assigned • • • • Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 267 • • • • • • • • • • “Post hoc ergo propter hoc” “Post facto ipse propter facto” Latin for “after this, therefore because of this” Title of West Wing episode Correlation versus causation “The rooster crows therefore the sun rises” Critical problem in our thinking “Because something occurs before something else does not mean that it caused it to happen”-corollary: it doesn’t mean that it didn’t “Because something occurred after an event does not mean that the event caused it to happen”-corollary: it doesn’t mean that it didn’t Administration of medication caused the cure Prozac causes people to commit suicide Need for ABAB experimental design to provide support for causation Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 268 Adaptive Living Skills • • • • • • • • • • • The “significant limitations” in adaptive behavior” criterion is operationalized as performance that is approximately two standard deviations below the mean. Evolution from a global description to specifying particular adaptive skills. Vineland Adaptive Behavior Scales (VABS) American Association on Mental Retardation Adaptive Behavior Scales (AAMR) CALS Scales of Independent Behavior – Revised (SIB-R) Assesses what a person can or cannot do The Inventory for Client and Agency Planning (ICAP) is one of the most widely used adaptive behavior assessments in the United States. The ICAP can be used to assess children and adults with developmental disabilities, people who become handicapped as adults through accident or illness, and elderly people who have gradually lost their independence. Often, these individuals need special assistance at home, at school and at work. The ICAP can identify the skills requiring assistance to allow the individuals to live as independently as possible. Adaptive Behavior Level (ABL) 01 = Mild ABL deficit 02 = Moderate ABL deficit 03 = Severe ABL deficit 04 = Profound ABL deficit Level of Care (LOC) Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 269 Supports Intensity Scale (SIS) • Philosophical underpinnings in new definition of disabilities • Developed by the American Association on Intellectual and Developmental Disabilities (AAIDD) (formerly the AAMR) • Designed to determine the level of support needed for an individual to do the same things that you and I do-the comparison is to a “typically functioning” individual • Based on 7 days per week, 24 hours per day • The focus is NOT on whether or not someone can do something, or whether or not the “community” can provide the supports, but rather on what supports are needed • Is completed in conjunction with the individual • Looks at several areas of life Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 270 Psychopathology Screening • Reiss Screen for Maladaptive Behavior (RSMB)-total score e.g. score above 9 on the 26 key items • Aberrant Behavior Checklist (ABC)-not based on DSM • Psychiatric Assessment Scale for Adults with Developmental Disabilities (PAS-ADD)-psychiatric assessment schedule for adults with a DD • Psychopathology Inventory for Mentally Retarded Adults (PIMRA) • Assessment of Dual Diagnosis (ADD) • Diagnostic Assessment of the Severely Handicapped-II (DASH-II) • Charlot Semi-structured Interview for Individuals with Intellectual Disabilities (CSI-intellectual disabilities) Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 271 • • • • • • • • • Instruments Assessing Quality of Life Quality of Life Questionnaire (QOLQ) COMPASS Lifestyle Satisfaction Scale (LSS) Multifaceted Lifestyle Satisfaction Scale (MLSS) Life Experiences Checklist (LEC) Quality of Life Interview Schedule (QUOLIS) Quality of Life Instrument Package Comprehensive Quality of Life scale Personal Wellbeing Index-Intellectual Disability (PWI-ID) Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 272 “People behave normally in an abnormal environment” • Examine the contingencies in the environment • What would you do if you lived in a controlled environment where you had little control • We inadvertently reinforce the behavior that we “seek” to diminish • Maladaptive-or is it? Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 273 Rights • • • • • • • • • • • • Choice-It is our responsibility to teach skills that become choice Rights Responsibilities ICF/IID Regulations/Guidance Human Rights Committee (Specially Constitute Committee) [W261-W265] Rights [W122-W138] ID Team/IPP [W238-W239, W278, W285-W289], W295-W297, W310W315] CMS-”QIDP” Overemphasis on Rights teaches Psychopathy Prioritization of Rights-safety Rights restriction-need to put in place a plan to reduce restriction to preclude civil rights violation Risk versus Risk-particularly relevant (risk on restricting rights versus risk of not restricting rights) Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 274 Rights and Responsibilities JOURNAL OF APPLIED BEHAVIOR ANALYSIS 1990, 23, 79-89 Number 1 (Spring 1990) BALANCING THE RIGHT TO HABILITATION WITH THE RIGHT TO PERSONAL LIBERTIES: THE RIGHTS OF PEOPLE WITH DEVELOPMENTAL DISABILITIES TO EAT TOO MANY DOUGHNUTS AND TAKE A NAP DLANE J. BANNERMAN, JAN B. SHELDON, JAMES A. SHuA.N, AND ALAN E. HARCHIK UNIVERS=Y OF KANSAS In the pursuit of efficient habilitation, many service providers exercise a great deal of control over the lives of clients with developmental disabilities. For example, service providers often choose the client's habilitative goals, determine the daily schedule, and regulate access to preferred activities. This paper examines the advantages and disadvantages of allowing clients to exercise personal liberties, such as the right to choose and refuse daily activities. On one hand, poor choices on the part of the client could hinder habilitation. On the other hand, moral and legal issues arise when the client's right to choice is abridged. Recommendations are offered to protect both the right to habilitation and the freedom to choose. DESCRIPTORS: developmentally disabled, ethics, client rights, choice behavior, mentally retarded Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 275 Rights Restrictions vs. Supports “Rights Restrictions” are any externally imposed limitation to an individual’s exercise of his or her rights. Typically this refers to an IDT and HRC approved instruction to staff to keep an individual from doing something they want to do. “Supports” are services, therapy, equipment, transportation, training, etc. provided by the staff/facility to an individual in order to increase/improve/facilitate an individual’s health, safety, independence, and exercise their rights. The way an individual expresses a choice must be determined on an individual basis. Choice or opposition can be expressed vocally, through facial expression, refusals, and/or actions. Rules of thumb for IDTs when making decisions regarding restrictions vs. supports: If the individual opposes the action, it’s a restriction. (e.g. Not allowed second helpings at meals.) If the purpose is to control deliberate behavior, it’s a restriction. (e.g. Not allowing the individual to leave the home.) When the IDT determines that an action is a support, the team must still assess, document deliberations, and as necessary implement any training and services needed to increase the individual’s independence, to improve the quality of the person’s life, and to expose/offer the individual more choices and options. The team has a proactive responsibility to help individuals exercise their rights. Any limitations placed on an individual by their legal guardian that fall within the limits described in the guardianship are not considered restrictions and do not require HRC approval but do require a plan by the team to restore the individual’s freedom of choice. Examples may be voting, clothing, hairstyle, religious observance, etc. NOTE: When a person is “adjudicated incompetent” and given a full guardian, they lose their fundamental rights and there is no need for a review from a legal perspective. The actual limitations of the person should be matched with the guardian’s power and responsibility as it is not legally considered a restriction if it is within the scope of the guardianship as written. However, from a facility policy and best practice perspective, the facility should take the position of making sure the guardianship remains the "best" match of support for the person. There is not a procedural safeguard nor does the court ensure that the guardian acts in the best interest of the individual. This is how the IDT and HRC annual review requirement connects to the essence of the role the HRC is supposed to play. If the IDT or the HRC find a pattern of the guardian not acting in the best interest of the individual, they would need to address this concern. Note: Individuals with disabilities are expected and taught to comply with commonly accepted rules of behavior that apply to everyone whether disabled or not. For example, no one has the right to stay uninvited in someone’s office, sit in the middle of the street, use state computers to view pornography, etc. ALL RESTRICTIONS REQUIRE DUE PROCESS. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 276 Civil Rights of Institutionalized Persons Act (CRIPA) • • • • Foundation for Settlement Agreement The Civil Rights of Institutionalized Persons Act (CRIPA) of 1980 is a United States federal law[1] intended to protect the rights of people in state or local correctional facilities, nursing homes, mental health facilities and institutions for people with intellectual and developmental disabilities. CRIPA is enforced by the Special Litigation Section in the United States Department of Justice Civil Rights Division, which investigates and prosecutes complaints in terms of this legislation.[2] The Special Litigation Section is allowed to investigate state or locally operated institutions in order to ascertain if there is a pattern or a practice of violations of a residents' federal rights.[2] The section is not allowed to investigate private facilities. They are also not allowed to represent individuals or address specific individual cases, but they are able to file lawsuits against facilities as a whole.[2] Authorizes DOJ to investigate facilities that show a pattern or practice that prohibits residents from the free exercise of their federal constitutional or statutory rights. DOJ’s work is directed at obtaining broad reform of conditions in institutions. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 277 Change in population Increase in individuals with: Mild/Moderate ID Dual Diagnosis Forensic issues Aging Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 278 Person Centered Planning Individual determines treatment planning Interdisciplinary team approach-not medical model Composition of team includes the individual All members have an equal voice Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 279 Senate Bill (SB-41) • Utilization of Restraints • The passage of SB 41 • Passed in 2011, state Senate Bill 41 codifies the DOJ recommendations for SSLCs to stop the use of prone holds and straitjackets, eliminate standing orders for restrictive controls, limit the use of mechanical restraints to emergencies, only use the least restrictive restraint techniques, and conduct an administrative review after all restraints. SB 41 also requires that each incident of physical or mechanical restraint in a SSLC must be reported to the executive commissioner of the Texas Health and Human Services Commission. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 280 Direct Support Professionals Week • • • • • • • • • • • • • • • • • H.B.ANo.A504 AN ACT relating to designating the second full week in September as Direct Support Professionals Week. BE IT ENACTED BY THE LEGISLATURE OF THE STATE OF TEXAS: SECTIONA1.AASubchapter E, Chapter 662, Government Code, is amended by adding Section 662.155 to read as follows: Sec.A662.155.AADIRECT SUPPORT PROFESSIONALS WEEK. The second full week in September is Direct Support Professionals Week to honor the work of direct support professionals as an integral part of the long-term support system for individuals with physical and mental disabilities. SECTIONA2.AAThis Act takes effect immediately if it receives a vote of two-thirds of all the members elected to each house, as provided by Section 39, Article III, Texas Constitution. If this Act does not receive the vote necessary for immediate effect, this Act takes effect September 1, 2015. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 281 Direct Support Professional • • • • • • • Direct Support Professional Week is this week. For insight to their daily duties, below are the job description and job functions required for their role. Job Description: Direct Support Professional is responsible for the routine and emergency care, treatment, and training for specified individuals with developmental disabilities in routine and crisis situations. Responsibilities may include such duties as grooming, bathing, feeding, observing and reporting client conditions and behaviors; interacting with clients therapeutically, participating in individualized training and/or active treatment programs. The DSP is required to accurately document client behavior(s) throughout the daily schedule, including response to home activities, home training and unusual incidents. Completion of work requires use of simple and/or routine duties, while decision making is based on simple and well-defined guidelines. This position may be required to drive a state owned vehicle. May perform other duties as assigned. Works under close supervision with minimal latitude for the use of initiative and independent judgment. Essential Job Functions: Assists persons served with training to teach daily living and vocational skills. Provides behavior intervention by following the recommended behavior intervention techniques to ensure that persons served are protected from harm or injury due to abuse/neglect, sexual incidents, serious injuries, or other sources of immediate danger and provides emergency care as needed. Participates in delivering therapeutic and individualized training per the clients active treatment program, and documents client progress. Assists persons served with carrying out necessary self-care skills (i.e., bathing, dressing, oral hygiene, toileting, feeding and grooming.) Insures environment is free of safety hazards by correcting any hazards found and reporting them to the supervisor. Observes persons served for signs and symptoms of disease, injury, reactions to medications, or other conditions that warrant medical intervention. Perform other related work as assigned. May prevent or manage aggressive behavior among clients and administer CPR in emergency intervention. Other duties as assigned include but are not limited to actively participating and/or serving in a supporting role to meet the agency’s obligations for disaster response and/or recovery or Continuity of Operations (COOP) activation. Such participation may require an alternate shift pattern assignment and/or location. These 2 paragraphs do not begin to describe their many duties or the caring and giving they provide. As quoted from a post to the National Alliance for Direct Support Professionals: “Direct Support Professionals bring hope into the lives of so many. Hope for friendships. Hope for belonging. Hope to be loved. Hope for opportunities to make money, pursue one’s passions, to make difference in one’s community and Hope to enjoy a life one’s choosing.” DSP’s take that hope and help people turn it into reality!! Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 282 Antecedents • Importance cannot be overestimated • Historically there has been an emphasis on consequences of behavior • Versus precursors behaviors (i.e. behaviors that an individual engaged in that often predicted the target behaviors • Antecedent behavior e.g. precursors to the challenging behavior • Establishing operations/discriminative stimuli in the environment that set the stage for the demonstration of the challenging behavior Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 283 Definition of insanity • “Doing the same thing and expecting a different result” • Change has to begin with your own behavior • Think about the difficulty in changing your own behavior, and how easy it is to tell somebody else to change theirs • Results in scapegoating Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 284 Trauma Informed Care • Understanding that the person is greater than the sum of their behaviors • Trauma is underdiagnosed • “Happy People Don’t Hit People” • Trauma Informed Coordinator Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 285 Genetic/Metabolic Abnormalities • Necessity of assessing/diagnosing/treating”closing the loop” • Practical Implications of Genetic Diagnoses for people with Intellectual Disabilities Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 286 Dramatic Changes • Need for increased staff, money, resources • Best practices Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 287 Functional Assessment-Important “to” vs. Important “for” (person centered approach) • Assess perspectives of person, family, friends, and staff • Detective work in all areas of life • Arrive at hypothesized function of challenging behavior Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 288 Changes in Nomenclature • QDDP-Qualified Developmental Disabilities Professional • QIDP-CMS-Qualified Intellectual Disabilities Professional • ICF/IID-Intermediate Care Facility/Individuals with Intellectual Disabilities • Mental Retardation/Intellectual Disability Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 289 Definition of Community • We are part of the community • What we really mean is outside of the institution • Need to conceptualize a flow from the institution to the larger community and vice versa Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 290 Programming • People may attend a program/programming (noun) • Demeaning-we don’t “program” people (verb) • Acceptable-we teach/educate/habilitate people Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 291 Documentation “Paper follows the person…….the person does not follow paper” Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 292 Discrimination versus generalization • It’s appropriate to scream at football game but not in dining room • It was sanctioned to kill in Vietnam but not at home • Teach person to exhibit same behavior in multiple settings Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 293 Skill Acquisition Plan (SAP) When there is no baseline data to support the existence of a given behavior the default is to assume that the behavior is not in the behavioral repertoire, therefore, a skill acquisition plan is developed. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 294 Skill Acquisition Plan (SAP) • • • SAPS PRACTICAL, FUNCTIONAL, MEANINGFUL SAP involves teaching of a skill that is not in the behavioral repertoire e.g. contrived/classroom setting Maintenance plan involves the level of prompting necessary for the learned skill to be demonstrated in the natural/in vivo environment – – – – – – – RATIONALE; REVIEW ISP, FSA, PSI, VOC, DAY HAB OBSERVATIONS OF SAP IMPLEMENTATION INTERVIEWS WITH STAFF AND INDIVIDUAL CONSISTENT WITH PERSONAL GOALS RELATE TO INDEPENDENCE OR QUALITY OF LIFE ASSESSMENTS SHOW GROWTH OR QUALITY FROM PREVIOUS ISP YEAR NOT A SAP FOR SKILL THAT THE INDIVIDUAL CAN DO Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 295 Maintenance of skills versus regression of skills • It is not always about enhancing skills • Minimize regression of skills • Maintain gains made in skills Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 296 First line of defense • Don’t create a PBSP for physical aggression that is caused by constipation • Address medical conditions e.g. a functional assessment that indicates that the person has no corpus callosum (Agenesis and Dysgenesis of the Corpus Callosum • Address engagement in the environment • Environmental/Genetic/Physiological factors can influence behavior Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 297 Errors • Omission-not doing the right thing • Commission-doing the wrong thing Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 298 Names in the field • • • • • • Nirbhay Singh Brian Iwata Stephen Reiss Johnny Matson Dennis H. Reid Karyn Harvey Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 299 Resources • • • • • • • • • • • • • • • • • • • • • • • • • • American Journal on Mental Retardation (AJMR) Volume 105, Number 3, May 2000, Special Issue, Expert Consensus Guideline Series: Treatment of Psychiatric and Behavioral Problems in Mental Retardation Expert Consensus Guidelines Update: Treatment of Psychiatric and Behavioral Problems in Mental Retardation 2004 American Psychologist, Journal of the American Psychological Association, January 2012, Volume 67, Number 1, Practice Guidelines, Guidelines for Assessment of and Intervention With Persons With Disabilities, Page 43-62 Olmstead v. L.C. & E. W., The Story of the Olmstead Decision and Three Determined Women from Georgia Functional Analysis of Problem Behavior, A Practical Assessment Guide, Robert E. O’Neill, Robert H. Horner, Richard W. Albin, Keith Storey, Jeffrey R. Sprague The International Consensus Handbook, Psychotropic Medications and Developmental Disabilities: Steven Reiss and Michael G. Aman, Editors Journal of Mental Health Research in Intellectual Disabilities, 6:208–224, 2013 Copyright © Taylor & Francis Group, LLC ISSN: 1931-5864 print/1931-5872 online DOI: 10.1080/19315864.2012.680681 Family Members’ Views on Seeking Placement in State-Supported Living Centers in Texas Teaching Anger Management to Persons with Mental Retardation. Betsey A. Benson, PH. D. 1992 Mental Health Aspects of Developmental Disabilities (formerly The Habilitative Mental Healthcare Newsletter) Cooper/White Book/BCBA Autism Speaks/Family Services/Challenging Behaviors Tool Kit www.qualitymall.org – Intellectual Disability Mental Health First Aid Manual 2nd edition http://aadmd.org – American Academy of Developmental Medicine and Dentistry http://www.ncd.gov/ - National Council on Disability Association of Professional Developmental Disabilities Administrators (APDDA) State Policies and Practices in Behavior Supports for Persons With Intellectual and Developmental Disabilities in the United States: A National Survey David A. Rotholz, Charles R. Moseley, and Kinsey B. Carlson INTELLECTUAL AND DEVELOPMENTAL DISABILITIES 2013, Vol. 51, No. 6, 433–445 AAIDD DOI: 10.1352/1934-9556-51.6.433 D. A. International Journal of Developmental Disabilities http://www.txdisabilities.org/ Coalition of Texans with Disabilities May Institute Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 300 Graduate Certificate in Developmental Disabilities • • • • • University of Kentucky The Human Development Institute (HDI) began offering a Graduate Certificate in Developmental Disabilities in the Fall semester of 2001. The purpose of this Graduate Certificate is to prepare professionals from a broad range of disciplines to play a leadership role in providing services and supports for people with developmental disabilities and their families. The curriculum emphasizes a life span and interdisciplinary perspective. Students will also have the opportunity to participate in a practicum and learn directly from individuals with developmental disabilities and their families. The Human Development Institute is Kentucky's University Center for Excellence in Developmental Disabilities Education, Research and Service. We focus our efforts on improving lifelong opportunities and services for individuals with disabilities, their families and the community. The Institute provides a strong foundation for more than 40 research, training and service projects, addressing a wide range of topics and issues in areas such as early childhood, education and alternate assessment, transition across the lifespan, employment, community living, and personnel preparation. HDI is a unit of the Office of the Vice President for Research at the University of Kentucky and a member institution of the Association of University Centers on Disabilities (AUCD). Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 301 Certificate of Completion in Intellectual/Developmental Disabilities • Minot State University • Bachelor of Science in Human Services with a major in INTELLECTUAL/DEVELOPMENTAL DISABILITIES • North Dakota Center for Persons with Disabilities Training Tools and Resources on Providing Supports for Persons with Developmental Disabilities • Department of Special Education • www.minotstateu.edu/sped/ • [email protected] • Minot, ND Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 302 College of Our Lady of the Elms • • • • • • • • • • • • Unique Programs in Autism Spectrum Disorders (ASD) Graduate Programs in Autism Spectrum Disorders (ASD) * MS in ASD with BCBA six-course sequence * Accelerated MS in ASD with BCBA six-course sequence * CAGS in ASD with BCAB six-course sequence * Certificate in Asperger's Studies Undergraduate Graduate Programs in Autism Spectrum Disorders (ASD) * Concentration in ASD * BCaBA Course Sequence www.elms.edu/asdgrad Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 303 VOR • VOR Mission Statement • VOR is a national organization that advocates for high quality care and human rights for people with intellectual and developmental disabilities. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 304 Universal LifeStiles • • THOMAS E. POMERANZ, Ed. D. Dr. Tom Pomeranz is a nationally recognized authority, trainer, clinician and consultant in the field of services for people with disabilities. The focus and spirit of Universal Enhancement© is found in how we need to behave in supporting others in improving the quality of their lives. For most individuals, a quality life is realized through friendships and meaningful relationships with others. Possessing things of meaning and value further enhances one’s quality of life. Hobbies, employment, spirituality and education are representative of the “things” most people cherish. The vision of Universal Enhancement© is to support people with disabilities to realize their quality of life outcomes; those outcomes to which we universally aspire. Universal Enhancement training provides participants with the specific tools-ways of behaving- needed to support others in realizing their preferred future. www.universallifestiles.com/pomeranz.html Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 305 DSM-5 • The recommendation of new categories for learning disorders and a single diagnostic category, "autism spectrum disorders" that will incorporate the current diagnoses of autistic disorders, Asperger syndrome, childhood disintegrative disorder and pervasive developmental disorder (not otherwise specified). Work group members have also recommended that the diagnostic term "mental retardation" be changed to "intellectual disability," bringing the DSM criteria into alignment with terminology used by other disciplines. • Autism organizations-happy • The diagnosis of Asperger’s syndrome has been removed from the DSM-5 and is now part of one umbrella, “Autism Spectrum Disorder”. This is controversial because according to the ICD-10, those suffering from Asperger’s syndrome have “no general delay or retardation in language or in cognitive development”. [Therefore why would they place this diagnostic category under "autism spectrum disorders“] • Asperger organizations-angry Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 306 Management versus Support • Management implies a reduction in the challenging behavior only. • Support implies a teaching/habilitative/educative component that supports the attainment of replacement behaviors. • Our mission is to teach functional replacement behaviors. • To do anything less implies that we are scapegoating individuals for exhibiting behaviors that they have learned in the absence of teaching better ways to meet their needs. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 307 Requesting versus informing • As “chronological” adults we should be teaching such individuals to inform others of their desires rather than requesting. • Adults don’t need to be “asking permission” to leave an area. • Adults provide information that they are leaving an area. • This speaks to the issue of dominance and control and a paternalistic environment. • We don’t command people, we ask them. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 308 Self-Injurious Behavior In Mental Retardation • Self-injurious behavior or SIB refers to an array of heterogeneous behaviors that typically create exasperating problems for the affected individual and for the surrounding human support system including parents and family members, teachers, direct care staff, paraprofessionals and professionals • The primary concern is that SIB poses a threat of lasting and irreversible physical harm Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 309 Characteristics of SIB Prevalence rates vary greatly Epidemiology of SIB -negative correlation between the prevalence of SIB and the level of mental retardation Topographies and Targeted Body Areas -invariant -individuals engage in their very own, idiosyncratic form of SIB -neither the targeted areas nor the inflicted damage are random -self-hitting or banging (i.e. butting, hitting, striking, slapping) that is either directed at the head or face, or at some other body parts -banging themselves with their own body parts (i.e. palms, fists, knees), or they use stable, hard objects against which to bang themselves -second most common form of SIB is self-biting -others include scratching, pinching, hair pulling, deliberate vomiting and rumination, and different forms of digging, poking or gouging Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 310 Mechanisms Controlling The Emergence and Maintenance of SIB Establishing Operations (EO) Distal Variables -predispose a person to a greater likelihood to develop a certain behavior as compared to peers who are similar in most other respects, with the exception of the predisposing attribute -SIB as a behavioral phenotype is a case in point (predisposing genetic/biological conditions and syndromes) Proximal Variables -control SIB more immediately from one occurrence to the next and are the primary targets of manipulation in a behavior program -antecedent events (such as establishing operations, discriminative stimuli), or consequence events Establishing operations are events that temporarily affect the effectiveness of a reinforcer, and simultaneously change the probability of occurrence of the operant that had produced that reinforcer in the past [physiological conditions-sleep deprivation, menses, anxiety, stress and over or under arousal of the CNS] [psychotropic medication-anhedonic effects of neuroleptics may impact the effectiveness of primary reinforcers, as well as the availability of desirable behavioral alternatives or the lack thereof, or reinforcer satiation] Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 311 • • • • • • Functional Assessment And Analysis (SIB) Designed to identify both response antecedent and consequent events that control the target behavior in order to select proper intervention strategies The role of behavioral assessment in selecting treatments based on the specific controlling variables of the target behavior of a specific individual has been a mainstay of behavior therapy from its beginning Functional assessment typically encompasses empirical, but non-experimental assessments that do not involve the removal of the individual from the natural environment in which the target behavior occurs (interviews, unstructured observations, data collection/scatter plots, contingency observations, rating scales) Functional analysis refers to the systematic, experimentally controlled exposure of the individual to stimulus conditions (analog conditions) suspected to be maintaining SIB Leads to individualized, function-relevant treatments Produces effective behavioral treatment programs and also reduces the likelihood of unwarranted and unnecessary psychopharmacological treatment or intrusive punishment procedures Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 312 Behavioral Interventions (SIB) • In many instances, multiple controlling variables are functionally related to SIB • Effective interventions must be comprised of multiple components • Focus of function-relevant treatment is not so much suppression of SIB, as it is altering the contingencies to render the SIB irrelevant, inefficient, and ineffective, and to replace it with behavior that is more beneficial to the focus person and those around her or him • Though biological determinants may increase probability of a particular topography’s emergence, or contribute to sustenance, it that does not mean that the behavior is immune to environmental influence (genetic, acquired brain injury, physiological basis) Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 313 Behavioral Interventions (SIB) Manipulation of Antecedents-does not directly contact the behavior, but instead alter the circumstances under which the behavior is most or least likely to occur, thereby indirectly affecting the behavior, and have been called “passive behavior management” -Manipulating Establishing Operations (EOs)-motivating antecedents (alter momentary potency of consequences) that enhance or degrade the relative momentary effectiveness of a reinforcer (sleep deprivation, physical discomfort related to menstrual periods, otitis, fooddeprivation or satiation, allergies, illnesses) Treatments-establishing regular sleep patterns, medically addressing physical discomfort and illness, ensuring adequate dietary intake, addressing physiology relevant establishing operations may substantially reduce or eliminate SIB for some individuals Sensorially or materially impoverished environments have been implicated as establishing operations promoting value of various reinforcers (remedying environmental deficits) Transition from one activity or location to another may also be an establishing operation that promotes SIB for some Clinical utility of altering value of reinforcers initially accessed contingent on SIB, by presenting those (or equivalent) reinforcers non-contingently (NCR) Preferred stimulus satiation (vary the sets of empirically identified stimuli used to enrich an environment • Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 314 Behavioral Interventions (SIB) • Manipulation of Antecedents (continued) • Manipulating Discriminative Stimuli-increase or decrease the momentary probability of a behavior by having preceded the response when it was reinforced or not increased in the past • Alter momentary probability of a particular response class by virtue of their presence when prior occurrences of the response class were followed by particular consequence operations Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 315 Behavioral Interventions (SIB) • Response Based Interventions • Active behavior management operates directly on the SIB • Altering properties of the response itself, such as effort (arm splints or wrist restraints) required to attain reinforcement, or by altering consequence aspects of contingencies that require less effort for an alternative behavior Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 316 • • • • • • • • • • Behavioral Interventions (SIB) Manipulating Consequences Differential reinforcement & Extinction for SIB Difficulty in exerting control over automatic, sensory reinforcement Providing sensory experience that successfully competes with that produced by SIB, irrespective of the SIB, can render the SIB inefficient and irrelevant Punishment procedures Restraining devices-helmet/splint (require fading procedures) Personal/physical restraint Devices that mask sensory stimulation-glove Caution-iatrogenic injury or exacerbation of behavioral difficulties Risk versus Risk analysis is necessary Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 317 Behavioral Interventions (SIB) • Manipulating Consequences • Identifying properties of consequences that exert reinforcer function • Providing sensory experience that successfully competes with that produced by SIB, irrespective of the SIB, can render the SIB inefficient and irrelevant Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 318 Self-Injurious Behavior (SIB) • • • • • • • • • • • • • • • SIB refers to behaviors, such as head-hitting or scratching, that people direct towards themselves and that results in tissue damage SIB does not define a topography SIB is dependent upon an outcome of an “injury” whether acquired immediately or over time Etiology is poorly understood Poses serious risk to those who engage in the behavior It represents a formidable challenge to those who are responsible for treating it The only treatments that have been consistently effective are those based on punishment in the form of aversive stimulation Research suggests that within-subject variability is a function of distinct features of the social and/or physical environment e.g. different sources of reinforcement Genes do not code for specific behaviors; rather, they influence the “organism as a whole” developmental system The assertion is that environmental pathogens cause behavioral disorders and genes influence susceptibility to these pathogens Recent research “Monitor on Psychology” July/August 2015 Vol. 46. No.7: non-suicidal self-injury (NSSI) in the DSM-5 “new disorder in need of further study” as well as a symptom of borderline personality disorder (BPD) Dialectical Behavior Therapy (DBT) Emotional benefits versus motivations behind it Pain offset relief-removal of pain stimulus does not return individual to pre-stimulus state, rather a short but intense state of euphoria (associate self-injury with relief) Risk factors-body objectification (viewing body as object), body devaluation, lack of internal bodily awareness, emotional dysregulation, eating disorders, pain endurance, low feelings of self-worth, negative self-image, associating pain with relief, associating negative thoughts with self-related words Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 319 Stereotypy vs. OCD • Stereotypy refers to motor behavior that is repetitive, often seemingly driven, and nonfunctionalcharacteristic feature of Pervasive Developmental Disorder (PDD) • OCD refers to a dynamic involving a reduction in anxiety • Obsession refers to the thought • Compulsion refers to the behavior-more complex and ritualistic and performed in response to an obsession or according to rules that must be applied rigidly • Intermittent Explosive Disorder refers to a reduction in anxiety (not mere physical aggression) Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 320 Stereotyped Acts • Defined as repetitious, topographically invariant motor movements (or sequence of motor movements), where reinforcement is not apparent and the act of performing the behavior is considered pathological • Defined as voluntary, developmentally inappropriate, repetitive motor movements, which serve no apparent adaptive function • Defined as a movement disorder characterized by repetitive, seemingly driven, non-functional motor behavior • Distinguished from self-injurious behavior Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 321 Stereotyped Acts • • • • • • • • • • • • • • Hand flapping Finger twirling Gazing at complex hand/finger movements Body rocking Body posturing (tensing) Jumping Spinning Toe-walking Light gazing Eye pressing Hair twirling Finger sucking Mouthing objects Vocalizing Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 322 Stereotyped Acts • • • • • • • • • • • Learning Theory-results under schedules of reinforcement, either positive or negative -Positive Reinforcement (Discriminative Stimulus) Hypothesis-created and produced by the individual and acquires reinforcing properties by the mere performance of the behavior/discriminative stimuli for gaining the social attention of others -Negative Reinforcement Hypothesis-maintained through the termination, escape, or avoidance of an aversive stimulus Homeostatic Theory-self-stimulatory in the form of arousal-inducing or arousal-reducing behaviors Self-stimulation Hypothesis-based on the notion that a certain minimum degree of stimulation is necessary Arousal Reduction and Filtering Hypothesis-modulates general arousal Developmental Theory-occurs during the normal progression of early developmental stages and reflects the child’s maturational process/may serve adaptive functions e.g. promote motor and personality development Cognitive Development Hypothesis-reflect early stages of cognitive development and resemble infant behavior observed during the sensorimotor period of developmental Motor Development Hypothesis-may emerge when coordinated motor behavior has been delayed Organic Theory-resulting from aberrant or abnormal physiological processes Biological Theory-evidence of a dysregulated central nervous system Dopamine Agonist-Induced Stereotypy-can be induced through stimulant administration Opioid Theory of Stereotypy-endogenous overactivity of the opiate system in the brain Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 323 When Should Stereotyped Acts Be Modified • Potential to harm the individual • Potential to harm someone else • Interferes with the individual’s potential to learn or work or otherwise interact adaptively with the environment • Socially odd or bizarre and serves as a “Scarlet Letter” of exceptionality that compromises potential for normalization within the community Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 324 What Treatments Are Available To Modify Stereotyped Acts? Behavior Modification Indirect Strategies -Environmental modification -Positive reinforcement -Functional communication training -Differential reinforcement (DRO, DRI, DRL) Direct Strategies -Extinction -Avoidance extinction -Sensory extinction -Punishment -Response prevention -Overcorrection -Multiple interventions Psychopharmacology Exercise Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 325 Exposure to the World • Mandate is to expose and teach people to the larger world-foundation on which to make choices • Socialization is not defined by a van ride to Walmart as it is stigmatizing and does not provide individualized habilitation Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 326 The fabric of our lives • How we treat human beings the other 23 hours of the day • So many examples of the impact on people • “You can’t sit at the staff table” • “You can’t have another iced tea” • “You can’t buy a coke from the vending machine” • How is it that we hold people that we support to a higher standard than we follow (aka members of congress) Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 327 ID versus Dementia • ID-prior to age 18 • Dementia-subsequent to age 18 • Life expectancy of many persons with developmental disabilities has increased, an increasing number of people are being diagnosed with dementia • Higher incidence of early-onset Alzheimer’s disease in people with Down syndrome • Diagnosis of Dementia in individuals with ID • Epidemiology of Alzheimer Disease in MR • Practice Guidelines for the Clinical Assessment and Care Management of Alzheimer and other Dementias among Adults with Mental Retardation • Purchasing Information for Test Battery • Test Battery for the Diagnosis of Dementia in Individuals with ID • Accurate diagnosis requires data over space and time • Impact on daily life is of critical importance for diagnosing Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 328 Dementia in I/DD • • • • • • • • • • • • http://www.medpagetoday.com/upload/2013/8/20/PIIS0025619613003716.pdf The National Task Group on Intellectual Disabilities and Dementia Practices Consensus Recommendations for the Evaluation and Management of Dementia in Adults With Intellectual Disabilities Researchers recommend a nine-step approach for assessing health and function. These include: Taking thorough history, with particular attention to "red flags" that potentially indicate premature dementia such as history of cerebrovascular disease or head injury, sleep disorders, or vitamin B12 deficiency Documenting a historical baseline of function from family members of caregivers Comparing current functional level with baseline Noting dysfunctions that are common with age and also with possible emerging dementia Reviewing medications and noting those that could impair cognition Obtaining family history, with particular attention to a history of dementia in first-degree relative Noting other destabilizing influences in patient's life such as leaving family, death of a loved one, or constant turnover of caregivers, which could trigger mood disorders Reviewing the level of patient safety gleaned from social history, living environment, and outside support Continually "cross-referencing the information with the criteria for a dementia diagnosis" Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 329 Early Detection Screen for Dementia Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 330 Assessment of Dementia Diagnostic Instruments -The Cambridge Cognitive Examination (CAMCOG) part of the Cambridge Examination for Mental Disorders of the Elderly-Revised (CAMDEX-R; Roth et al., 1986 Roth et al., 1998. -Severe Impairment Battery (SIB; Saxton et al., 1993) Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 331 Assessment of Dementia Direct Performance-Based Neuropsychological Assessments -DYSPRAXIA scale for adults with Down Syndrome (Dalton & Fedor, 1997, 1998) -Dalton/McMurray Visual Memory Test: Delayed Matching to Sample Cognitive Test (Dalton, 1995) -The Rivermead Behavioural Memory Test (RBMT); Wilson et al, 1985, 1991. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 332 Assessment of Dementia Informant-Based Assessment Instruments -Dementia Questionnaire for Persons with Mental Retardation (DMR; Evenhuis, 1990, 1992, 1996) -Dementia Scale for Down Syndrome (DSDS; Gedye, 1995) Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 333 Mental Retardation & Psychiatry • Psychiatric Assessment of the Person With Mental Retardation • Essentially the same save for level of selfreport versus behavioral observations • The Role of the Psychiatrist in Mental Retardation • The Patient with Mental Retardation Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 334 • • • • • • • • • • • Expert Consensus Guideline Series American Journal On Mental Retardation (AJMR) Volume 105, Number 3 May 2000 Treatment of Psychiatric and Behavioral Problems in Mental Retardation Guideline 1. Diagnosis and Assessment Guideline 2. Informed Consent Guideline 3. Psychosocial Treatment Guideline 4. Medication Treatment General Principles Guideline 5. Selection of Medications Guideline 6. Managing Inadequate Response to Initial Medication Treatment Guideline 7. Medication Dosing Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 335 Debriefing 101 Debriefing the use of restraint Debriefing: a one-time semi-structured conversation with an individual or individuals who have experienced a stressful or traumatic event. Purpose: to reduce any possibility of psychological harm by informing people about their experience or allowing the individuals involved to talk about it. Purpose: to determine the cause of the incident that required intervention. Purpose: to determine how to avoid such incidents in the future. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 336 Developmental Disabilities and Law Enforcement Training for police officers “They’re all just people” Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 337 Consent • Informed • Risk/Benefit-Risk of implementing treatment versus benefit of implementing treatment • Risk/Risk-Risk of implementing treatment versus risk of not implementing treatment • Impact of signs/symptoms on daily life (we do not obtain consent for an individual who is hallucinating but for the impact that the hallucinations have on the life of the individual) Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 338 Empiricism • “This intervention won’t work” • Don’t engage in crystal ball reading • You cannot predict the outcome of a given intervention until you implement it and obtain data as to the effectiveness Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 339 Psychology is a Science Not because of the nature of the information, but by the way in which the information is obtained e.g. the scientific method/experimental method/research design Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 340 Motivational Assessments • Reinforcer Survey • Premack Principle • Reiss Motivation Assessment Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 341 Normalizing • We get “used to” people acting the way they do • Result is that we “normalize” or minimize the clinical significance which results in minimizing the importance of treatment • “Johnny is just being Johnny”-when in fact Johnny is suicidal, homicidal, and floridly psychotic Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 342 The Importance of Work (Vocation) Cannot be overestimated Freud: Love/family and work Key aspect of human and social functioning If an individual wants to be an astronaut begin by providing them with a book about astronomy • Employment in the community for people diagnosed with ID is both an international as well as national right. • PL (Public Law) 106-170, or the Work Incentives Improvement Act-required networks to serve people with significant disabilities • • • • Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 343 Murdoch Center Foundation • • • • • • • • Murdoch Method Task Analyses-never reduce the criterion for success for completion of a task [break down the task to enhance success] Standard Measure of Success (MOS) is 80% Individualizing the approach does not require “reinventing the wheel” but applying the appropriate step based upon task analysis Developmental Disabilities Support Needs Assessment Profile (DD-SNAP) The Murdoch Center Foundation is a private, nonprofit corporation dedicated to education, research and professional advancement in the field of intellectual and developmental disabilities (IDD). The Foundation publishes a curriculum guide and an assessment tool for use with persons having IDD. Sales of these products fund activities that benefit the people who live and work at the Murdoch Developmental Center in central North Carolina. The Murdoch Center Foundation is an Internal Revenue Service 501(c)(3) corporation (not directly affiliated with the Murdoch Developmental Center). The Murdoch Center Program Library is a collection of almost 1000 task analyses of specific skills which are particularly applicable to the habilitation of persons with severe and profound mental retardation. http://www.murdochfoundation.org/index.htm Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 344 Delayed Gratification • • • • • • • • • Delay of Reinforcement. Not feasible to immediately gratify needs. Address the need-binder effect. Guidelines for programming indiscriminable contingencies. Indiscriminability of the contingency (i.e. the learner cannot tell exactly when emitting the target behavior in the generalization setting will produce a reward at a later time.) Use continuous reinforcement during the initial stages of acquiring new behaviors or when strengthening little-used behaviors. Systematically thin the schedule of reinforcement based on the learner’s performance. When using delayed rewards, begin by delivering the reinforcer immediately following the target behavior and gradually increase the response-to-reinforcement delay. Each time a delayed reward is delivered, explain to the learner that he is receiving the reward for specific behaviors performed earlier. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 345 Psychology Discipline Ownership of Functional Assessment Ownership of PBSP No ownership of psychoactive medication consents No ownership of psychoactive prescription Discipline specific issues and competency/credential issues Example: the discipline of Medicine owns medical procedures so why should other disciplines own Psychology procedures • Example: when creating a “consult” the genius is in the formulation of the question to the “expert”, not dictating to the expert what procedure to perform • • • • • • Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 346 State Policies and Practices in Behavior Supports • State Policies and Practices in Behavior Supports for Persons with Intellectual and Developmental Disabilities in the United States: A National Survey • David A. Rotholz, Charles R. Moseley, and Kinsey B. Carlson • INTELLECTUAL AND DEVELOPMENTAL DISABILITIES • 2013, Vol. 51, No. 6, 433–445 AAIDD • DOI: 10.1352/1934-9556-51.6.433 Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 347 State Policies and Practices in Behavior Supports Abstract Providing effective behavioral supports to decrease challenging behavior and replace it with appropriate alternative skills is essential to meeting the needs of many individuals with intellectual and developmental disabilities (IDD). It is also necessary for fulfilling the requirements of Medicaid funded individual support plans and is important for moral, ethical, and societal reasons. Unfortunately, there is no national standard for behavioral support practices or source of information on the status of behavior support policies, practices, and services for adults with IDD at either state or national levels. The collection of comprehensive data on state behavior support definitions, provider qualifications, training, and oversight requirements is a necessary starting point for the development of plans to address needed policy and practice changes. This survey is the first national assessment of state policies and practices regarding the definition and delivery of behavior support services to people with intellectual and developmental disabilities receiving publicly financed supports in the United States. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 348 The Flynn Effect (The impact of an IQ score) Rising IQ scores Educational Implications: Who Receives MR Services Financial Implications: The Costs of MR Legal Implications: The Flynn effect and the Law-A Matter of Life and Death-International and U.S. Law on the Execution of Those with Mental Retardation-Under US law, the execution of the insane - someone who does not understand the reason for, or reality of his or her punishment - violates the US Constitution (Ford v Wainwright, 1986). 1989 Penry v. Lynaugh Executing persons with mental retardation is not a violation of the Eighth Amendment. (Overturned in Atkins v. Virginia (2002) • Occupational Implications: The Flynn Effect and the Military • Placement Decisions • • • • Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 349 Practice Effects • • • • • • Practice effects refer to gains in scores on cognitive tests that occur when a person is retested on the same instrument, or tested more than once on very similar ones. These gains are due to the experience of having taken the test previously; they occur without the examinee being given specific or general feedback on test items, and they do not reflect growth or other improvement on the skills being assessed. Such practice effects denote an aspect of the test itself, a kind of systematic, builtin error that is associated with the specific skills the test measures. These effects relate to the test’s psychometric properties, and must therefore be understood well by the test user as a specific aspect of the test’s reliability. Retesting occurs fairly commonly in real circumstances for reasons such as mandatory school reevaluations, longitudinal research investigations, unwitting or deliberate duplication by different professionals who are evaluating the same individual, a parent’s or teacher’s insistence that a child be retested because the test scores imply that the child was not trying, and so forth. A keen understanding of differential practice effects facilitates competent interpretation of test score profiles in those instances in which people are retested on the same or a similar instrument perhaps several times. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 350 Practice Effects • • • • • • • No specific length of time between tests is required to study practice effects; it depends on the generalization sought or needed. If the interval is very short-for example, a few hours, or a couple of days-then examinees are likely to remember many specific items that were administered. They are likely to retain specific picture puzzles, arithmetic problems, or block designs, and recall the strategies that proved most successful; the results is an inflated estimate of the practice effect; that is, relative to an inference about established (learned) effects. In contrast, intervals that are long, perhaps six months or a year or two, are confounded by variables other than the test’s psychometric properties and practice as such. Long intervals allow forgetting of the test’s content, and therefore reduce the magnitude of the practice effects, at the same time, in lengthy intervals there can be real growth or decline of the abilities measured. When change has occurred, it becomes difficult to separate the test’s practice effects, as such, from the person’s improvement or decay on the skills. For preschool children, who experience rapid development even three or four months may be too long an interval for studying a test’s practice effects. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 351 Practice Effects • The most commonly useful intervals for investigating a test’s practice effects are between one week and about two months, with one month or so representing a reasonable midpoint. • Intervals of that approximate magnitude are typical of the test-retest reliability investigations reported in the test manuals of popular individually administered intelligence and achievement tests. • The Administration and Scoring Manual for the test cautions against serial testing because of practice effects. There is no justification to disregard or even question this caution for adults with ID. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 352 Factors That May Affect Test Scores • Practice effects • “Flynn effect” (i.e., overly high scores due to out-of-date test norms) • Invalid scores may result from the use of brief intelligence screening tests or group tests; highly discrepant individual subtest scores make an overall IQ score invalid • Instruments must be normed for the individual’s sociocultural background and native language. • Co-occurring disorders that affect communication, language, and/or motor or sensory function may affect test scores • Individual cognitive profiles based on neuropsychological testing are more useful for understanding intellectual abilities than a single IQ score. Such testing may identify areas of relative strengths and weaknesses, an assessment important for academic and vocational planning • IQ scores are approximations of conceptual functioning but may be insufficient to assess reasoning in real-life situations and mastery of practical tasks Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 353 Re-Testing of IQ Implications -Requires parent/guardian consent -Results above IQ of 70 may result in loss of waiver funds -In some cases the institutionalization represents the best treatment option Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 354 IQ & Death Penalty • • • • • • • • High court bars rigid IQ cutoff for executions May 27, 2014 The Supreme Court ruled in the case of Freddie Lee Hall, on Florida's death row for more than three decades. (Photo: AP) WASHINGTON — The Supreme Court made it more difficult Tuesday for states to execute prisoners who claim an intellectual disability, marking the first time it has fine-tuned its landmark 2002 decision barring the death penalty for those with mental impairments. The court ruled that Florida must apply a margin of error to IQ tests administered to Freddie Lee Hall, 68, who killed a 21-year-old pregnant woman and a deputy sheriff in 1978. The state had argued that any test score above 70 made prisoners eligible for a death sentence, despite medical guidelines that permit scores to reach 75. "Intellectual disability is a condition, not a number," Justice Anthony Kennedy said in the 5-4 ruling, joined by the court's four liberal justices. The decision will affect a handful of states with similar policies among the 32 states with death penalties on the books. Though very few prisoners with intellectual disabilities will be granted reprieves as a result, the ruling clarifies a delicate area of criminal law. It comes as states' capital punishment procedures are under siege, beset by a shortage of drugs needed to perform lethal injections and rejuvenated efforts by disability rights groups to stop executions of prisoners with mental impairments. A federal appeals court blocked Texas this month from executing a death row prisoner claiming intellectual disability. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 355 The Death Penalty and Intellectual Disability • In a landmark decision in Atkins v. Virginia in 2002, the Supreme Court ruled that executing someone with ID is a violation of the Eighth Amendment of the U.S. Constitution, which prohibits cruel and unusual punishment. In its 2014 decision, Hall v. Florida, the Court ruled that, while states have the right to establish their own rules for handling Atkins cases, they cannot ignore scientific and medical consensus regarding intelligence and the nature and diagnosis of ID. The Court rejected the use of an IQ test score of 70 as a bright-line cutoff for determining ID and ruled that all evidence pertinent to the claim, including adaptive behavior assessments, should be considered. • Critical topics: foundational considerations, including diagnostic criteria, the definition of ID, the analyses of Atkins cases; assessment considerations; intellectual functioning, including IQ testing and the Flynn effect; adaptive behavior; and related topics, such as cultural and linguistic factors, competence to waive Miranda rights and to stand trial, retrospective diagnosis, malingering, comorbid disorders, educational records, and professional issues. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 356 “Briseno Factors” [regarding adaptive behavior] When the issue of mental retardation is raised post-conviction in a death penalty case, the Sixth and Eighth Amendments require that either the convicting court or the Court of Criminal Appeals review the evidence provided in the writ application to determine whether the evidence propounded by the applicant is sufficient to make a prima facie showing of mental retardation, and, if so, whether the evidence argued in the party's brief conclusively establishes that the applicant is mentally retarded. If the court finds, based on the pleadings, that the applicant has conclusively proven mental retardation, the court may, without empaneling a jury, grant the relief to which applicant is entitled. The applicant would receive no greater relief from a jury determination. If the applicant has only established a prima facie case, the Sixth and Eighth Amendments require the convicting court to empanel a jury and hold a hearing for the limited purpose of resolving the factual issue of mental retardation. At that hearing, the applicant carries the burden of proof and the jury is required to come to a unanimous conclusion regarding whether the applicant has shown by preponderance of the evidence that he is mentally retarded. Depending on the jury's answer, the convicting court must then provide this Court with a recommendation to either deny relief on the applicant's allegation of mental retardation or commute the applicant's sentence to life. - See more at: http://caselaw.findlaw.com/tx-court-ofcriminal-appeals/1333303.html#sthash.rz0CRBdy.dpuf Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 357 • • • • • • • “Briseno Factors” [regarding adaptive behavior] Did those who knew the person best during the developmental stage-his family, friends, teachers, employers, authorities-think he was mentally retarded at that time, and, if so, act in accordance with that determination? Has the person formulated plans and carried them through or is his conduct impulsive? Does his conduct show leadership or does it show that he is led around by others? Is his conduct in response to external stimuli rational and appropriate, regardless of whether it is socially acceptable Does he respond coherently, rationally, and on point to oral or written questions or do his responses wander from subject to subject? Can the person hide facts or lie effectively in his own or others' interests? Putting aside any heinousness or gruesomeness surrounding the capital offense, did the commission of that offense require forethought, planning, and complex execution of purpose? Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 358 • • • • • • “Briseno Factors” [regarding adaptive behavior] http://caselaw.findlaw.com/tx-court-of-criminal-appeals/1333303.html Based on “Of Mice And Men” by John Steinbeck http://damiencomerford.com/tag/briseno-factors/ Texas Continues To Execute People Who Have Severe Intellectual Disabilities The Texas definition is bizarre to put it mildly. Many would be familiar with the John Steinbeck 1937 novella, Of Mice and Men. It is a classic piece of American literature. But in Texas the book is more than just a classic, it has legal status. Under what are known as “Briseno factors”, the State establishes the profile of an individual who ordinary Texans would agree was intellectually disabled. It points to Lennie Small, the lumbering and childlike character in John Steinbeck’s book, identifying him as the legal yardstick. In other words, the Texas definition of intellectual disability has to match the degree of mental impairment depicted by a character in a fictional novella. The writer, John Steinbeck once said, Texas was a state of mind. But, if the State of Texas continues to use one of his characters, as a legal benchmark for intellectual disability, out of its mind might have been a more accurate description. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 359 CURRENT DEVELOPMENTS 2012-2013: Of Mice and Men, Fairy Tales, and Legends: A Reactionary Ethical Proposal to Storytelling and the Briseño Factors Fall, 2013 Georgetown Journal of Legal Ethics In reviewing Texas' adherence to the Briseño factors--non-scientific standards inspired by the character Lennie in Of Mice and Men and not by actual science or clinical protocol 1--it is evident that the use of storytelling can have a result that even Critical Race theorists would not desire. Critical Race theorists have traditionally been against the conservative trends of adhering strictly to law, precedent, and controlling cases. Instead, they advanced theories that examined legal issues on a case-by-case basis while paying attention to how society shaped the individuals who are likely to be affected by legal decisions. Typically, a marginalized person, such as a minority with an intellectual disability, would be a part of the constituency that Critical Race Theory (CRT) would choose to protect. Unfortunately, CRT supports Texas' divergence from Atkins v. Virginia, which holds that the execution of intellectually disabled persons is a violation of the Eighth Amendment's prohibition against cruel and unusual punishment, and supports the Of Mice and Men-influenced Briseño factors. It perpetuates a general misunderstanding of persons with intellectual disabilities and hinges an individual's life on non-scientific and non-fact based assertions. Tempering the practice of storytelling with an ethical guideline will avoid the manipulation of information that is presented to the trier-of-fact. 2 Recently, the Texas courts refused to classify Marvin Wilson as an intellectually disabled person protected by the Supreme Court's decision in Atkins, 3 making Wilson one of seventy individuals who have contested their death sentence under ... https://litigationessentials.lexisnexis.com/webcd/app?action=DocumentDisplay&crawlid=1&doctype=cite&docid=26+G eo.+J.+Legal+Ethics+859&srctype=smi&srcid=3B15&key=319fa09f59c7d5dce8457f2fdd17f9fe Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 360 Punishment Model • We do not provide a punishment model-harsh, demeaning, negative, etc. • By “punishing” an individual for behavior by precluding the involvement in preferred activity we effectively set the person up to fail due to the lack of habilitation, engagement, etc. • The only justifiable means for precluding an individual from engagement in a preferred activity is current/imminent danger to self or others Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 361 Court Three things that the Judge wants to know: 1. Does the individual meet the criteria for a diagnosis of ID 2. Is the individual competent to stand trial 3. What is the best placement for the individual Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 362 Forensic Evaluations Texas Code of Criminal Procedure Competence Assessment for Standing Trial for Defendants with Mental Retardation (CAST*MR) Evaluation of Competency to Stand Trial-Revised (ECST-R) Under age 17- “Unfit to Proceed” Texas Family Code Chapter 55 Over age 17- “Incompetency to Stand Trial” Texas Code of Criminal Procedure Chapter 46B Article 46C, “Insanity Defense” Court does not currently recognize DSM-5 changes to ID Court currently recognizes IQ and MR Competency-This standard relates to the defendant’s ability to relate to the criminal justice system Presumption of competency Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 363 Forensic Evaluations Hi Robb: Very nice talking with you in Austin. CST is clearly a functional analysis of current functioning. Sanity, on the other hand, is a retrospective analysis of what an individual was capable of knowing sometime in the past. Sanity relies much more heavily on collateral information. Statute precludes continuing with sanity if, in your opinion, the person is not competent to stand trial. This is because if a person is not competent at the time of the evaluation, chances are the person is also incompetent to comprehend your disclosure (or informed consent if the evaluation is not court ordered). It is also not clear that the individual would be able to give you truly helpful information regarding sanity under these circumstances. Mary Alice Mary Alice Conroy, Ph. D., ABPP Sam Houston State University Assuming the individual has not been transferred to adult court, a 17 or under would fall under Chapter 55—same standard for competence (fitness to proceed), different standard for sanity (responsibility for conduct). Mary Alice Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 364 House Bill (H.B.) No.807 Determination of Mental Retardation (DMR) DMR is equivalent to Full/Comprehensive Psychological Evaluation H.B.ANo.A807 AN ACT relating to the practice of psychology; authorizing a fee. BE IT ENACTED BY THE LEGISLATURE OF THE STATE OF TEXAS: SECTIONA1.AASections 593.004 and 593.005, Health and Safety Code, are amended to read as follows: Sec.A593.004.AAAPPLICATION FOR DETERMINATION OF MENTAL RETARDATION. (a) In this section, "authorized provider" means: (1)AAa physician licensed to practice in this state; (2)AAa psychologist licensed to practice in this state; (3)AAa professional licensed to practice in this state and certified by the department; or (4)AAa provider certified by the department before September 1, 2013. (b)AAA person believed to be a person with mental retardation, the parent if the person is a minor, or the guardian of the person may make written application to an authorized provider [the department, a community center, a physician, or a psychologist licensed to practice in this state or certified by the department] for a determination of mental retardation using forms provided by the department. Sec.A593.005.AADETERMINATION OF MENTAL RETARDATION. (a) In this section, "authorized provider" has the meaning assigned by Section 593.004. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 365 Diagnostic Assessment Rule March, 2015 Chapter 5, Provider Clinical Responsibilities--Intellectual Disability Services Subchapter D, Diagnostic Assessment • §5.151. Purpose. • The purpose of this subchapter is to describe the criteria to be used and the process to be followed: • (1) by an authorized provider employed by or contracted with a local intellectual and developmental disabilities authority (LIDDA) or a state supported living center (SSLC), to conduct a diagnostic assessment for intellectual disability, autism spectrum disorder (ASD), and a related condition; • (2) by a LIDDA or SSLC, to review a DID or a diagnosis of ASD or related condition for endorsement; and • (3) by DADS, to approve an employee of a LIDDA or an SSLC as a certified authorized provider. • (10) DID (determination of intellectual disability)--An assessment conducted in accordance with §5.155 of this title (relating to Determination of Intellectual Disability (DID)) by an authorized provider to determine if an individual meets the criteria for a diagnosis of intellectual disability. • §5.158. Related Condition (RC). • If an individual is determined not to have an intellectual disability, an authorized provider described in §5.155(c) of this title (relating to Determination of Intellectual Disability (DID)) may use information from the DID to assist in establishing the individual’s eligibility for certain Medicaid services based on the existence of a related condition, as described in the DADS-approved list of related conditions and §9.238 of this title (relating to ICF/MR Level of Care I Criteria) or §9.239 of this title (relating to ICF/MR Level of Care VIII Criteria). Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 366 DIAGNOSTIC ELIGIBILITY FOR SERVICES AND SUPPORTS http://www.dads.state.tx.us/providers/LA/DMRBestPracticesOctober2000.pdf MENTAL RETARDATION PRIORITY POPULATION CHAPTER 415, SUBCHAPTER D BEST PRACTICES GUIDELINES OCTOBER 2000 1. Choosing Appropriate Intellectual Testing Instruments 2. Overall Intellectual Functioning 3. Standard Error of Measurement 4. IQ Scores Needed to Qualify for Mental Retardation Services funded by General Revenue vs. Medicaid (70 vs. 69) 5. Suggested Instruments and Procedures to Use When an Individual is Unable to Participate in Traditional Standardized Intellectual Testing 6. Assessing Adaptive Behavior 7. Determining and Documenting that Mental Retardation was Present During the Developmental Period 8. Accessing Information from Public Schools 9. Endorsing Reports or Validating Assessments Conducted by Others 10. Interpretation of Results of the DMR 11. When to Conduct DMR Updates and Reevaluations 12. Evaluating Very Young Children 13. Addressing the Needs of Persons with Other Conditions who can be Served in Mental Retardation Services 14. Capacity Assessment Instrument for Use in Guardianship Hearings 15. Competency to Stand Trial under Chapter 46.02 of the Criminal Code 16. Assessments under the Family Code Chapter 55.33 17. Reimbursement for DMRs 18. Ethical Standards that Apply to the DMR Process Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 367 SB 1664 (The ABLE Act) Texas Legislative Session ending 06/01/2015 Current law essentially requires people with disabilities to remain in abject poverty to access necessary services and support from the state and federal government. With the passage of SB 1664 (The ABLE Act) individuals with disabilities will be able to set up a tax-free savings account for health care, education, transportation, personal support services, housing, and other qualified expenses. This program is not a government handout that produces government dependency. Instead it is a hand-up that allows an individual use their own funds to manage their disability which will lead to greater independence and healthier living at no cost to the state. This legislation is a game changer for the disability community by allowing individuals to save their own money and contribute towards their own independent living. http://www.txdisabilities.org/able-act Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 368 Endorsement/Validation/Concurrence/ Update • • • • • • • • • • • • • • • • • • • • Endorsement of a report refers to accepting the entire report and assessments of another professional without any changes or additions. Validation refers to accepting the results of specific assessment measures obtained by another professional. An endorsement should, at minimum, identify the results and include a statement referring to the report being accepted with the report attached. All the required elements of a Determination of Mental Retardation (DMR) report specified in the rule must be present. If any element is missing, the MRA (Mental Retardation Authority usually referred to now as the Local Authority) will need to complete its own assessment to include that missing element, but can use the test results by validating them. Validated testing may be included in a report when additional current assessments are also included. For validation, a statement should be included noting that the results of the testing done by the other professional remain valid. Concurrence signifies that the reviewer agrees that the information reviewed is still a valid representation of the individual. Update involves the addition of new information. Upon application, the court will require a DMR that is current within 6 months. DADS policy and the TAC on DMRs, permits a concurrence. The PMRA (Persons with Mental Retardation Act)-Standard civil commitment requires an IDT report current within six months of the court hearing but does not specifically require the DID/DMR to be current within six months, although some courts may have that requirement. All adult forensic commitments are based on the maximum time they would’ve received if convicted of their crimes. For many, their max time may be 6 mo. to 2-5 years. Each one will need to be assessed by their team for community transition prior to their max time deadline. If they are not referred the LA will be asked to obtain a new commitment. This procedure needs to be implemented for all adult forensic cases. A concurrence should work. The PMRA (Civil Commitment) requires an IDT report current within six months of the court hearing but does not specifically require the DID/DMR to be current within six months, although some courts may have that requirement. (46B maximum time out ). Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 369 • Satiation • Variety Reinforcement Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 370 Noncontingent Reinforcement (NCR) • Reduction of challenging behavior from baseline (i.e. reinforcement) levels • Delivery of an aberrant behavior’s known reinforcer on a response-independent basis i.e. fixed time (FT) or variable time (VT) • Conceptualized as establishing operation (EO) manipulations • Attenuating a deprivation state (weaken the reinforcement for the aberrant behavior) • Think about “attention”-if we provide attention then attention will not be so important for the individual to obtain Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 371 Self-Soothing • Teaching self-calming • Providing the environment conducive to selfcalming • No “quiet/time-out” rooms based on structure but based on function Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 372 Sexuality & Love • • • • • • “I was not attempting to evaluate its’ moral implications” Spock Whose issue is it anyway: “ours or theirs” Needs to be addressed Intellectually/developmentally disabled does not equate with sexually disabled Education is paramount Still in the caveman days Vital part of functioning Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 373 Sexuality People with intellectual and developmental disabilities (IDD) have a history of being seen as asexual. Separated from society at large, they have been denied access to life experiences afforded to the typically-abled population, the most glaring of which is access to an intimate partner. Like most adults, many people with IDD have a desire to engage in sexual activity with another person. The penal laws in many states dictate that this sexual interaction should only occur if both parties are consenting. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 374 Sexuality • • • • • • Choices and Consent: Adults with developmental disabilities have the right to make their own decisions about relationships. A person with a developmental disability has the right to engage in sexual activity with another person providing he/she is capable of providing informed sexual consent. Friendships and Relationships: Most relationships are not sexual, but some are physically affectionate. All people have the right to be physically affectionate with an agreeable party. Physical affection differs from sex. Sex is the touching of the sexual parts (breasts, vagina, penis, anus) of the body for sexual gratification. Physical affection does not require the ability to provide consent, but rather, just a willing partner. Education and Information: ...education and information depending on interest and need, at a level and pace people with a developmental disability can understand, including the following in this suggested order: Development of self-awareness and self-esteem, awareness of others, body language, assertion, relationships, body changes and awareness, awareness of self as a sexual being, abstinence, sexual expression, awareness of laws relating to sexual expression, avoiding abuse, personal and sexual hygiene, STDs and HIV/AIDS, pregnancy and contraception, marriage, and parenting skills. Sexual Expression: We also recognize that people have different sexual orientations and preferences. Stated in our policy is the following: "Accept that people with developmental disabilities may be heterosexual, lesbian, gay, bisexual, transgender, monogamous or not monogamous, and have the right to express themselves accordingly." As previously stated, staff do not have the right to impose our values. As long as the sexual act is legal and involves consenting adults, we don't interfere. Reproduction and Contraception: Most people with ID/DD would have significant difficulties raising a child. Yet there are some people who can. If the person is a consenting adult, he or she has the right to determine a method of contraception if so desired. A person with ID/DD who is a consenting adult and gets pregnant has the legal right in our state to carry the child to term and attempt to raise the child, or to have an abortion, or to give the child up for adoption, and we support those rights. For those who do decide to parent, we offer parenting groups to support them in raising their children. Sexual Behaviors: Some of the people we support try to meet their sexual needs through the Internet and/or 900 numbers. We are very concerned that they might be exploited or abused due to their cognitive limitations and possible emotional vulnerabilities. Our policy states that we "Ensure that the treatment team is aware of consumer's use of technology (such as accessing personal ads, calling sexually explicit 900 numbers, etc.) in fulfilling sexual expression." Also that we "limit the use of the Internet and/or monitor telephone calls if there is probable cause that the person is engaging in illegal activity." Because the chat lines also have per-minute calling charges, we also try to keep a close eye on the expenditures of those who use them and catch any financial problem as early as possible. Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 375 Texas Statutes - Subtitle D: PERSONS WITH MENTAL RETARDATION ACT (PMRA) • Texas Health & Safety Code-formerly known as PMRA • • • • • • • • • • • • • • • Chapter 591 GENERAL PROVISIONS Subchapter A GENERAL PROVISIONS Subchapter B DUTIES OF DEPARTMENT Subchapter C PENALTIES AND REMEDIES Chapter 592 RIGHTS OF PERSONS WITH MENTAL RETARDATION Subchapter A GENERAL PROVISIONS Subchapter B BASIC BILL OF RIGHTS Subchapter C RIGHTS OF CLIENTS Subchapter D RIGHTS OF RESIDENTS Chapter 593 ADMISSION AND COMMITMENT TO MENTAL RETARDATION SERVICES Subchapter A GENERAL PROVISIONS Subchapter B APPLICATION AND ADMISSION TO VOLUNTARY MENTAL RETARDATION SERVICES Subchapter C COMMITMENT TO RESIDENTIAL CARE FACILITY Subchapter D FEES Subchapter E ADMISSION AND COMMITMENT UNDER PRIOR LAW Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 376 Texas Statutes - Subtitle D: PERSONS WITH MENTAL RETARDATION ACT (PMRA) • • • • • • • • • • • • • • • • • • • • Chapter 594 TRANSFER AND DISCHARGE Subchapter A GENERAL PROVISIONS Subchapter B TRANSFER OR DISCHARGE Subchapter C TRANSFER TO STATE MENTAL HOSPITAL Chapter 595 RECORDS Section 595.001 CONFIDENTIALITY OF RECORDS Section 595.002 RULES Section 595.003 CONSENT TO DISCLOSURE Section 595.004 RIGHT TO PERSONAL RECORD Section 595.005 EXCEPTIONS Section 595.0055 DISCLOSURE OF NAME AND BIRTH AND DEATH DATES FOR CERTAIN PURPOSES Section 595.006 USE OF RECORD IN CRIMINAL PROCEEDINGS Section 595.007 CONFIDENTIALITY OF PAST SERVICES Section 595.008 EXCHANGE OF RECORDS Section 595.009 RECEIPT OF INFORMATION BY PERSONS OTHER THAN CLIENT OR PATIENT Section 595.010 DISCLOSURE OF PHYSICAL OR MENTAL CONDITION Chapter 597 CAPACITY OF CLIENTS TO CONSENT TO TREATMENT Subchapter A GENERAL PROVISIONS Subchapter B ASSESSMENT OF CLIENT'S CAPACITY; INCAPACITATED CLIENTS WITHOUT GUARDIANS Subchapter C SURROGATE CONSENT FOR ICF-MR CLIENTS Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 377 ASSESSMENT OF STIMULUS PREFERENCE AND REINFORCER VALUE WITH PROFOUNDLY RETARDED INDIVIDUALS Reinforcement is a central mechanism in the development of operant behavior. In attempting to apply operant techniques to establish or maintain socially desirable outcomes, considerable emphasis is placed on the selection of suitable reinforcement schedules and contingencies; however, the process of reinforcer identification is often taken for granted. Thus, it is likely that at least some of the failures to effect behavior change can be attributed to defective stimulus selection rather than to contingency management. Potential reinforcers may be identified quite readily for some individuals by simply asking them what they prefer, or by exposing them to an array of stimuli and recording the duration or frequency of interaction with each stimulus. In contrast, for many impaired individual who may be nonverbal and do not engage in spontaneous play, or who have limited sensory and motor capabilities, the identification of reinforcing stimuli has been problematic. JOURNAL OF APPLIED BEHAVIOR ANALYSIS 1985, 18, 249-255 NUMBER 3 (FALL 1985) Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 378 Great Quotes • • • • • • • • • • • • • • • “What do we call them?” They have names just like you do……. “We can’t treat them…..they’re psychotic” That is what you should be treating……. “These people can’t learn” Perhaps you can’t learn…….single celled organisms can learn “Why are you doing that” What difference does it make….. “He has multiple personality because he is talking in funny voices” Read your DSM “He has intermittent explosive disorder because he hit someone” Read your DSM “He is cycling” He does not have a bicycle…..His symptoms are cyclical “If they drool and look funny it doesn’t mean they are mentally retarded” DSM criteria in plain English “Sheila is just being Sheila” Sheila just ripped the artery out of her arm with a piece of wood. I believe she is suicidal. “Randy is just being Randy” Randy has no corpus callosum and is jumping out in front of 18 wheelers on the highway……and by the way don’t you think such information should be captured in the functional assessment under the heading of medical issues He’s not seeing things…. Don’t presume to tell another individual what their reality is. All you can say is that you don’t see what he is seeing. “I’m going to jump out the window and kill myself” Nurse replies “I’ll go get the key to open the window for you”…….Countertransference? “It’s genetic so there is nothing we can do”……Think about genotype versus phenotype…..genotype does not code for behavior “He’s crying over the loss of his friend”…..He needs a psychiatric consult……Grief is a normal human emotion “He’s having tantrums”…..He is manic….No, he is having tantrums Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 379 The End Hope you enjoyed my presentation Thank you Copyright Dr. Robb Weiss, Psy. D., BCBA-D 2015 380