Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
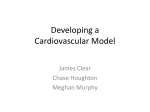
Winter 2015 Miami Cardiac & Vascular Institute: New Name Reflects Integration I n May, Baptist Cardiac & Vascular Institute announced a name change to Miami Cardiac & Vascular Institute. The transformation, however, goes much deeper than a simple name revision. The Institute is now extending its services, expertise and innovation across Baptist Health South Florida to bring benefits in clinical care that will enhance the Institute’s vision to become one of the leading cardiac and vascular centers in the country. These newly integrated heart and vascular services are available at Baptist Hospital, Doctors Hospital, Homestead Hospital, Mariners Hospital, South Miami Hospital and West Kendall Baptist Hospital, along with more than 15 outpatient centers spanning three counties. Combining the unique talents and technologies of each facility and allowing for the sharing of clinical data make it possible for cardiac and vascular patients to experience consistent, exceptional, evidence-based care no matter the location. Barry T. Katzen, M.D., who founded the Institute in 1987, remains at the helm with the title of chief medical executive. Carol Mascioli has assumed the title of chief operating officer, and Bo Boulenger, CEO of Baptist Hospital, will provide oversight for the Institute as the executive champion for Baptist Health. “The integration involves the continued development of multidisciplinary cooperation and partnerships between physician leaders and administrators that will be based on quality and outcomes, service, efficiency and cost,” Mr. Boulenger said. Part of Baptist Health’s commitment to the community and beyond is a $100 million expansion project that is underway on the Baptist Hospital campus. It will include the development of unique programs for aneurysms, structural heart disease and endovascular therapies, advanced procedure suites and a larger gallery where physicians can collaborate and teach the techniques they have pioneered to others from across the world. It will open in 2016. DOTTER LECTURE James Benenati, M.D., Delivers Dotter Lecture For more than 50 years, Baptist Health has provided excellent heart and vascular care. The Institute has long been known as a pioneer in multidisciplinary, less invasive techniques. Not only has the Institute participated in hundreds of clinical trials, but its groundbreaking research has led to new approaches in medicine. Its physicians lecture around the world. Although its name has changed, one priority of the Institute has not faltered — its desire to help patients from throughout Florida and around the world. If you have a patient who may qualify for one of our research trials, we hope you will contact Miami Cardiac & Vascular Institute at 786-596-5974. For a full list of research trials, please visit BaptistHealth.net/Research. n James Benenati, M.D., medical director of both the Peripheral Vascular Laboratory at Miami Cardiac & Vascular Institute (formerly Baptist Cardiac & Vascular Institute) and Interventional Radiology for Baptist Health, received the honor of delivering the opening talk at the Society of Interventional Radiology’s 39th Annual Scientific Meeting in San Diego. It is the largest national meeting of interventional radiologists. The lecture is named after one of the founding fathers of interventional radiology, Dr. Charles T. Dotter, who was nominated for the Nobel Prize in Physiology for Medicine in 1978. “I am deeply humbled to be included among past Dotter lecturers — interventional radiology pioneers who solved difficult medical problems with creativity, innovation and research,” said Dr. Benenati, who is credited with developing one of the country’s most coveted and sought-after fellowships and is best known for his work to establish a nationally renowned, accredited peripheral vascular laboratory. “I have known Jim since the early days of our founding and I am pleased that he is recognized for his dedication, brilliance and ability to lead while encouraging collaboration among our teams at the Institute,” said Barry T. Katzen, M.D., founder and chief medical executive. n James Benenati, M.D. This is the final issue under the name Baptist Cardiac & Vascular Institute. In the future, this publication will reflect the Institute’s new name, Miami Cardiac & Vascular Institute. If you prefer to receive this in an electronic format, please email [email protected]. Assessing Potentially Safer, Faster and Easier AAA Repair Patients with challenging infrarenal abdominal aortic aneurysms (AAA) – and the physicians who treat them – may soon benefit from a new treatment option. A clinical trial at Miami Cardiac & Vascular Institute examined the long-term safety and efficacy of completely sealing these risky aneurysms with a biocompatible polymer. Minimally invasive repair with the Nellix EndoVascular Aneurysm Sealing System (Endologix, Inc.) was provided to appropriate candidates with an infrarenal AAA larger than 5 cm. Institute researchers plan to assess the safety of the Nellix polymer strategy relative to more-traditional shunt repairs. The Institute participated in this multicenter trial because this intervention could prove beneficial for many aneurysm patients, including those with more-challenging aortic presentations. Shorter procedure time could be a benefit for both patients and physicians. The Nellix permits easier endovascular delivery and deployment compared to many existing devices for aneurysm repair. Once injected in the aneurysm sac, the biocompatible polymer hardens in three to five minutes. Researchers hope that complete sealing of the sac will preclude the need for any secondary interventions. Pending results of this and other trials set to evaluate Nellix in up to 180 patients at 30 sites in the United States, Canada and Europe, the study could be expanded to anyone with a treatable size AAA. The study duration is 24 months. Institute physicians plan to evaluate participants twice in the first year post-intervention and then annually for life. n Researchers Evaluate the Potential of Sutureless Aortic Valve Implantation potential benefits compared to existing aortic valve replacement technology. People who require aortic valve replacement are typically complex, highly comorbid patients who can benefit in particular from a shorter duration of cross-clamping and cardiopulmonary bypass. The Perceval S device is placed through a minimally invasive procedure or implanted in combination with more-conventional heart surgery. People experiencing symptomatic aortic valve stenosis and small annuli and/or calcified annuli could benefit from this valve procedure. Additionally, the Perceval could be appropriate for some patients who require redo valve procedures. Medium-to-high-risk patients over the age of 60 who require aortic valve replacement were considered for the trial. The Perceval S is a collapsible profile valve positioned and secured without the need for sutures. Commissural, straight struts hold the valve to the heart anatomy and sinusoidal struts attach the valve to the sinus of Valsalva. By making this new technology available for aortic valve replacement, the Institute remains on the forefront of providing innovative technology for our patients. Institute researchers plan to specifically assess the five-year results for improved gradients across the valves, a decreased heart size over time and a lower rate of overall complications, including the incidence of perivalvular leak. Ideally, investigators would like to see fewer patients returning because of complications, a reduced need for pacemaker placement and improved five-year survival. n Sutureless Aortic Valve that anchors itself during the aortic valve replacement surgery, shortening the surgery time for the patient to spend supported by the heart and lung bypass machine and improving performance of the operation through smaller and better-tolerated incisions. Miami Cardiac & Vascular Institute researchers are evaluating new technology with the potential to permit faster and easier replacement of an aortic heart valve. The Institute was the only site in Florida that participated in the prospective, multicenter trial to evaluate the Perceval S Sutureless Heart Valve (Sorin Group USA, Inc.). Although the trial is now closed, researchers plan to monitor participants for a minimum of five years after implantation. Investigators will specifically evaluate complication and survival rates versus historic controls, and will compare outcomes against performance measures for other stented bioprostheses reported in the literature. Shorter cross-clamp duration, faster overall cardiopulmonary bypass time and quicker recovery for patients are among the a) Intra-luminal catheterization of the aneurysm in the abdominal aorta. b)Covered stent-grafts placed inside the aneurysm to preserve the intraluminal flow. Proximal ending of the stent at the orifice of the renal arteries and distal end in the common Iliac artery. c) Endovascular aneurysm sealing with polymer to minimize risk of leaking. Taking a New Route to Aneurysm Repair A young woman with a large intracranial aneurysm and bad headaches came to Miami Cardiac & Vascular Institute for consultation. Having met the criteria for an innovative, minimally invasive new trial of flow diverter technology, she underwent the procedure and fared well. Noteworthy, yes; but her story also represents hope to other high-risk patients – people with giant irregular aneurysms and few options. Large or giant brain aneurysms can be deadly if left untreated. Although some people remain symptom-free, others experience debilitating symptoms when the aneurysms grow so large that they compress on nerves or other structures in the brain. Large or giant aneurysms are difficult to treat with traditional “open” surgery due to the high mortality rate. Smaller aneurysms elsewhere in the body are commonly repaired through conventional endovascular or surgical approaches. However, internal carotid artery aneurysms larger than 10 mm come with bigger challenges. Physicians at the Institute are now enrolling patients in this new trial to evaluate the Surpass Flow Diverter (Stryker Neurovascular Corp.). Enrollment criteria include having an unruptured, complex internal carotid artery aneurysm greater than 10 mm in diameter. The Institute is the only site in South Florida participating in the multicenter Safety and Effectiveness of an Intracranial Aneurysm Embolization System for Treating Large or Giant Wide Neck Aneurysms (SCENT) trial. Safety and efficacy over 12 months are the primary outcomes of the trial. Although not the first flow diverter device, the mesh component is different. The Surpass system also is designed to be easier to deliver and deploy at the aneurysm site. It could soon become a new endovascular option for physicians treating these challenging patients. Under X-ray guidance, physicians insert a catheter in the groin and advance it to the site of the aneurysm. A microcatheter delivers the flow diverter. Once properly positioned, the device is deployed. Before Immediately after deployment stagnation of flow in the aneurysm This device received FDA approval in 2013. A flow diverter is essentially a special stent with very tight mesh. The device diverts blood flow from the aneurysm into the normal vessel to cause the shrinking and permanent sealing of the aneurysm. Over time, full diversion of blood flow results in rerouting and reconstruction of the vessel. Initially the flow diverter technology was reserved for aneurysms considered otherwise untreatable, such as giant fusiform dissecting aneurysms. If the initial promise of the SCENT and other trials continues, flow diverters could revolutionize how physicians repair a wider scope of aneurysm types. Exploring the full potential of this new-generation device aligns with the Institute’s goal to remain on the forefront and offer new technology to patients.n Setting the Pace on Leadless Technology Potential problems for some patients with traditional pacemakers include the risk of infection and the need to retrieve and replace the leads over time. New technology offers a possible solution. Miami Cardiac & Vascular Institute physicians are enrolling candidates in a Phase I clinical trial to assess the safety and efficacy of a leadless, single-chamber ventricular pacemaker system. Study participants will be among the first humans worldwide to undergo implantation with the Micra Transcatheter Pacing System (Medtronic). The miniaturized pacemaker is about the size of a vitamin, making it about 10 times smaller than a traditional pacing system. Physicians deliver the device directly into the heart using a catheter inserted in a femoral vein. They attach the pacemaker in the muscle wall using tines only a few millimeters long. A tiny electrode then delivers electrical pulses to pace the heart. Because the Micra device does not require leads that connect to the heart, researchers hope patients will experience fewer complications. For example, although risk of infection is low with current leadbased devices, when they do occur, infections can be devastating for patients. In addition to potentially safer pacing, patients will likely be more comfortable and experience fewer limitations on activities of daily living immediately post-procedure and over the long term. Appropriate candidates for the trial will need ventricular pacing and must be capable of walking one to three minutes on a treadmill during evaluation. In addition, people must be able to return for follow-up evaluation during the trial in order to be considered for enrollment. Physicians will use radiofrequency technology to communicate with the implanted pacemaker. This allows them to noninvasively calibrate and communicate with the device. Morbidly obese patients are not candidates for the trial because of the small chance that physicians will be unable to properly communicate with the device. The Institute is the only site in South Florida enrolling patients in this international trial. Demonstrating the safety of the Micra system is the main objective of the trial. It’s also a non-inferiority study, meaning researchers at the Institute hope to show that the device is as good as, if not better than, commercially available pacemakers. The retrievable device is designed to last at least seven years. Retrieval, if any, will depend in part on how patients fare over the duration of study followup. As engineering and technology progress, the next generation of miniaturized technology may be wireless, dual-chamber devices. n Wireless advanced pacing technology with a miniaturized devise that represents the world’s smallest pacemaker, delivered directly into the heart through a catheter inserted in the femoral vein. The pacemaker is MRI compatible. Baptist Health South Florida 8900 North Kendall Drive Miami, FL 33176-2197 Change service requested Leading the Way on Lipid Management The Role of PCSK9 in the Regulation of LDL Receptor Expression !"#$%&&'()#*+",$-'#-"(.($",&/ NON-PROFIT ORGANIZATION U.S. Postage PAID Permit No. 2655 Miami, FL remove them, disposing of them through the bile. Typically the receptors regenerate and remove the particles over and over. However, PCKS9 doesn’t allow the receptor to recirculate. As a result, elevated lipid levels remain. Institute physicians are on the forefront of this research and conducting multiple Phase 3 studies to further evaluate PCKS9 inhibition, including: Statin Intolerant Trial. Patients who cannot tolerate statins because of side effects or a relevant family history may be candidates for this research. A sizable minority of people cannot tolerate statin therapy (approximately 10 percent to 15 percent of Caucasians, for example). Participants will be evaluated for response to PCKS9 treatment over 24 months. 13 13 Cholesterol travels inside lipoprotein particles. The main way excess cholesterol is removed by the body is by these cholesterol containing particles to fit a receptor in the liver and the entire particle and receptor is taken in by the liver. The cholesterol is removed in the bile and the receptor is recycled to pick up another particle. PCSK9 is a protein that prevents the receptor from recycling. Blocking PCSK9 increases the receptors and, thus, particle and cholesterol removal. Clinical trials underway at Miami Cardiac & Vascular Institute explore the promise of a new strategy to treat people with lipid abnormalities. This novel treatment takes advantage of the body’s own mechanism for removing LDL cholesterol from the bloodstream. For some people, favorable genes enable them to live with naturally lower levels of LDL cholesterol. For others who are not as fortunate, an antibody therapy could provide the same advantage. By harnessing and enhancing the liver’s own cholesterol-clearing action, inhibition of PCKS9 (proprotein convertase subtilisin/ kexin type 9) could revolutionize how physicians prevent cardiovascular events. This approach may even help people with lipid abnormalities who do not respond or who respond only partially to traditional cholesterol-lowering medication. In fact, some initial PCKS9 inhibitor trials demonstrated benefits for patients with elevated cholesterol despite statin therapy. Institute researchers are capitalizing on recent discoveries about PCKS9. The PCKS9 protein is an adverse player in the liver’s natural mechanism for removing LDL cholesterol and triglycerides from the blood. Normally, lipoprotein particles travel the bloodstream, where they pick up and encapsulate LDL cholesterol and triglycerides. When these particles reach the liver, special receptors grab and Baptist Cardiac & Vascular Institute LLC Management Company Founder and Medical Director Barry T. Katzen, M.D., James F. Benenati, M.D., Lawrence Blacher, M.D., Abilio A. Coello, M.D., Nestor Demorizi, M.D., Rajesh Dhairyawan, M.D., Jonathan Fialkow, M.D., Julius Gasso, M.D., Alvaro A. Gomez, M.D., Efrain H. Gonzalez, M.D., Curtis A. Hamburg, M.D., Dean Heller, M.D., Howard E. Katzman, M.D., Karl H. Lembcke, M.D., Ramon L. Lloret, M.D., Madeleen Mas, M.D., Alvaro Mayorga-Cortes, M.D., Niberto L. Moreno, M.D., Constantino Peña, M.D., Edward Peron, M.D., Gerardo A. Polanco, M.D., Alex Powell, M.D., Orlando Puente, M.D., The FOURIER Outcomes Trial. People with elevated LDL cholesterol despite statin treatment (including partial responders) and those with diabetes and/ or a history of myocardial infarction might be suitable candidates for an outcomes trial. This international, double-blind, placebo-controlled study is called the Further Cardiovascular Outcomes Research with PCKS9 in Subjects with Elevated Risk (FOURIER) trial. Researchers hope to demonstrate that PCKS9 inhibition is associated with a decrease in “hard events,” including heart attack and stroke. They also plan to track secondary outcomes, such as the incidence of stent placements and hospitalizations. Consider referring your patients to the Institute if they meet the criteria for these PCKS9 Phase 3 trials. Thought leaders and experts in multiple areas of cardiovascular medicine collaborate in research and clinical treatment at the Institute for the benefit of patients. n Ramon Quesada, M.D., Jonathan S. Roberts, M.D., Ignacio Rua, M.D., Shaun Samuels, M.D., Paul Seigel, M.D., Marcus St. John, M.D., Richard E. Tannenbaum, M.D., Athanassios Tsoukas, M.D., Billy K. Yeh, M.D. Editors: Barry T. Katzen, M.D., and Ramon Lloret, M.D. Managing Editor: Amy Erez Writer: Damian McNamara Editorial Contributors: Ripal Gandhi, M.D., Jonathan S. Roberts, M.D., Adrienne Sylver