Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Cardiac contractility modulation wikipedia , lookup
Heart failure wikipedia , lookup
Coronary artery disease wikipedia , lookup
Electrocardiography wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
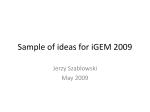
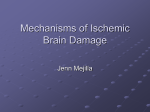
1525 Effects of Ischemia and Hypercarbic Acidosis on Myocyte Calcium Transients, Contraction, and pHi in Perfused Rabbit Hearts Rajendra Mohabir, Hon-Chi Lee, Robert W. Kurz, and William T. Clusin Downloaded from http://circres.ahajournals.org/ by guest on October 13, 2016 The time courses of changes in pHI and cytosolic calcium were compared in isolated perfused rabbit hearts with the use of the calcium-sensitive fluorescent indicator indo-1 and the pH indicator 2',7'-bis(2-carboxyethyl)-5(6)-carboxyfluorescein (BCECF). Cell-permeant forms of these indicators were loaded into myocytes by arterial infusion or by direct infusion into the extravascular space. Indo-1 fluorescence was recorded from the epicardial surface of the left ventricle at an excitation wavelength of 360 nm and emission wavelengths of 400 and 550 nm. BCECF fluorescence was recorded at an excitation wavelength of 490 nm and an emission wavelength of 530 nm. Calibration procedures were developed for each indicator that allowed [Ca2"], and pHi to be quantified during ischemia. Global ischemia decreased contractility and caused a rapid increase in both the systolic and end-diastolic levels of the calcium transients. Ninety seconds of ischemia increased peak systolic [Ca2"]i from 609±29 to 1,341±+159 nM, while end-diastolic [Ca2"]I increased from 315+±25 to 553+52 nM. The observed increase in diastolic [Ca21]1 was shown not to arise from indo-1-loaded endothelial cells. The initial increase in [Ca21]i was followed by a gradual decline and then a secondary rise occurring between 5 and 15 minutes of ischemia. In contrast, ischemia caused a monotonic decrease in pH; from a baseline of 7.03+0.06 to 6.83±0.02 after 2 minutes, 6.32±0.1 after 10 minutes, and 6.11±0.04 after 15 minutes. Perfusion of hearts with acidified (hypercarbic) saline increased the systolic and diastolic levels of the calcium transients, but only when pH; fell below a threshold value, which was more acidic than values achieved during the first 2 minutes of ischemia (6.83+±0.03). Lesser degrees of acidification caused a decrease in contractility but did not affect the calcium transients. Effects of pHi on the calcium transients were not due to altered calcium sensitivity of indo-1. These results suggest that cytosolic acidification may contribute to the increase in [Ca2`]; during the first 15 minutes of global ischemia, but the [Ca2`J, increase during the first 2 minutes is mediated by other factors. (Circulation Research 1991;69:1525-1537) Recent studies have revealed that an increase in [Ca2"]i occurs during the reversible phase of myocardial ischemia, when contraction strength is declining.1'2 Although the decline in contraction strength was initially taken as evidence From the Division of Cardiovascular Medicine, Falk Cardiovascular Research Center, Stanford University School of Medicine, Stanford, Calif. Supported by a grant from the National Institutes of Health (HL-32093) and by a Grant-in-Aid from the American Heart Association, California Affiliate. R.M. and H.-C.L. were recipients of individual postdoctoral fellowships from the Canadian Heart Foundation and the California Affiliate of the American Heart Association. R.W.K. was supported by the Max Kade Foundation, and W.T.C. was an Established Investigator of the American Heart Association. Address for correspondence: William T. Clusin, MD, Division of Cardiovascular Medicine, Falk Cardiovascular Research Center, Stanford University School of Medicine, Stanford, CA 94305. Received February 13, 1989; accepted June 28, 1991. against an early [Ca2"]i increase, several factors are now believed to decrease the sensitivity of the myofilaments to Ca2' during ischemia3 and prevent the increase in [Ca2"]i from being manifested as increased force. One of these factors is intracellular acidosis.4 An early decrease in pHi has been observed during ischemia by a variety of techniques (see Reference 5 for review), and there is evidence that the degree of acidification that occurs in the first few minutes of ischemia would be sufficient to reduce contraction strength. However, continuous measurement of pHi has only recently become feasible in the intact heart. Intracellular acidification may also be a causative factor in mediating the increase in [Ca2"]i during ischemia. Recordings of calcium transients in aequorin-loaded papillary muscles show that acidification with lactate or CO2 causes a rapid increase in the 1526 Circulation Research Vol 69, No 6 December 1991 Downloaded from http://circres.ahajournals.org/ by guest on October 13, 2016 peak systolic level of the calcium transients.6,7 A resting [Ca2"]i increase has also been recorded in acidified cardiac fibers impaled with calcium-selective intracellular electrodes.8 These observations have fueled speculation that acidification of the cytoplasm during ischemia may contribute to, or perhaps wholly explain, the concomitant increase in [Ca2+1i.9-11 In the present study we used cell-permeant fluorescent indicators to obtain measurements of pHi and [Ca2+]i from the left ventricular surface of rabbit hearts during global ischemia and during perfusion with C02-enriched saline. pHi was measured with 2 ',7 ' -bis(2-carboxyethyl)- 5(6)-carboxyfluorescein (BCECF),12-14 whereas [Ca2+i] was measured with indo-1. The indo-1 method was refined to permit conversion of fluorescence to [Ca2+]i and to allow examination of whether the increase in diastolic [Ca 2]i during ischemia reflects changes occurring in the cardiac myocytes. These measurements confirm that cytoplasmic acidification can contribute to the decrease in contraction strength and the increase in [Ca 2]i during the first 15 minutes of ischemia. However, the early elevation of myocyte calcium transients during the first 2 minutes of ischemia cannot be accounted for by cytoplasmic acidification and must therefore be due to other causes. Materials and Methods Isolated Heart Preparation Male albino New Zealand rabbits (1.8-2.2 kg) were killed by cervical dislocation. The heart was rapidly removed and perfused with a saline solution via the aorta at a constant flow rate of 20-30 ml/min. The perfusate contained (mM) NaCl 115, KCl 4.7, CaCl2 2.0, MgCl2 0.7, NaHCO3 28, NaH2P04 0.5, glucose 20, and probenecid 0.3 as well as insulin (10 units/l) and bovine serum albumin (40 mg/l). The pH was adjusted to 7.4. Probenecid has been shown to prevent loss of tetracarboxylate fluorescent indicators from cells by blocking an organic anion transport system.15 The buffer was equilibrated with 95% 02-5% CO2 and heated to maintain the heart at 30+ 1°C. Left ventricular pressure was recorded with an isovolumic intracavitary latex balloon containing a fiberoptic pressure transducer (Camino Laboratories). The cannulated latex balloon was inserted through the mitral orifice of the left ventricle. The cannula was secured by sutures placed at the lower left atrium. A syringe filled with deaerated water was attached to the cannula and was used to fill the balloon. The heart was paced at 180 beats/min using an epicardial plunge electrode placed in the right ventricle. Optical Recording Apparatus Calcium transients were recorded from the epicardial surface of the left ventricle as previously reported.1 Illumination from a 100 W mercury vapor lamp was filtered at 360±5 nm and directed via a silica fiberoptic cable onto the surface of the heart. The fiberoptic cable was attached to the heart by a plastic sleeve and rubber girdle to minimize relative motion. Ultraviolet illumination was confined to a circular region on the left ventricular epicardial surface 1 cm in diameter. Fluorescence emissions were collected by a ring of eight coaxial fiberoptics and were directed through a beam splitter into two photomultipliers (Hamamatsu) fitted with optical band-pass filters (400±5 and 550±5 nm). The output of the photomultipliers was passed into an electronic ratio circuit to obtain the fluorescence ratio (F400/F550). The output of the ratio signal was filtered by a low-pass filter at settings of 30-70 Hz and recorded on a strip-chart recorder. Vascular and Extravascular Loading Techniques Indo-1 AM was solubilized in anhydrous dimethyl sulfoxide containing pluronic F-127 (25% wt/vol) and infused at a final concentration of 2.5 ,uM with 5% fetal calf serum. Initial experiments were performed in hearts that had been perfused with indo-1 AM for 30 minutes followed by a 30-minute washout to eliminate extracellular indo-1 AM. High-quality calcium transients were obtained by this technique, but several factors suggest that much of the total fluorescence arose from nonmyocytes. 1) The total fluorescence at 400 and 550 nm is 14- to 20-fold greater than the net amplitude of the calcium transients.12 A baseline fluorescence of this magnitude is not expected from single myocyte experiments or from the in vitro spectra of indo-1. 2) The maximum calciumdependent fluorescence level, determined with high calcium and ionophore concentrations, is also too large in relation to the calcium transients.' 3) Infusion of bradykinin (10-5 M) into the heart produced a parallel shift in the systolic and diastolic levels of the calcium transients, even though bradykinin (10`5 M) had no effect on [Ca 2]i in isolated rabbit ventricular myocytes (M. Lauer, unpublished observations). Bradykinin is known to increase [Ca 21i in vascular endothelial cells, and therefore, uptake of indo-1 AM by endothelium could explain the effects of bradykinin on surface fluorescence in the intact heart.16 To minimize the uptake of indo-1 AM by endothelial cells, indo-1 AM was introduced directly into the extravascular space by intramyocardial infusion. A 25-gauge hypodermic needle was inserted 1-2 mm beneath the epicardium of the left ventricle, at the site where the fiberoptic cable was attached. Solution containing indo-l AM was then infused by a syringe pump at 0.5 ml/min for 30 minutes. An additional period of 30 minutes was allowed for removal of indo-1 AM after the syringe pump was turned off. This method produced a bright region of localized fluorescence 6-10 mm in diameter from which calcium transients could be recorded. The extent of nonmyocyte fluorescence in hearts loaded by the extravascular infusion was tested with bradykinin (10-5 M). The response of the calcium transient to bradykinin was reduced by extravascular loading and could be eliminated completely by pretreatment of the heart with a low concentration of Mohabir et al Ischemia and Hypercarbic Acidosis in Rabbit Hearts Downloaded from http://circres.ahajournals.org/ by guest on October 13, 2016 ionomycin. Infusion of 100 nM ionomycin caused a parallel upward shift in the peak and baseline levels of the calcium transients, similar to that produced by bradykinin. This response was not due to fluorescence changes in myocytes, because diastolic ventricular pressure did not increase. Addition of i0-` M bradykinin in the presence of ionomycin had no effect on the calcium transients. The bradykinin response was also blocked by ionomycin in cultured rat aortic endothelial cells containing indo-1 (authors' unpublished observations). We infer that elevation of endothelial [Ca2+]i is the mechanism by which ionomycin blocks the bradykinin response. The effects of ionomycin on the bradykinin response are temporary if the infusion is discontinued after 5-10 minutes, but prolonged exposure (45 minutes) causes permanent loss of the response, even though the myocardial calcium transients remain unchanged. Loss of the bradykinin response is accompanied by a reduction in the baseline fluorescence at 400 and 550 nm, with no reduction (and therefore a relative increase) in the phasic component of the calcium transient. These observations suggest that there is selective loss of indo-1 from nonmyocytes after prolonged ionomycin treatment. The basis for such an effect is not known, but experiments in fura-2-loaded mast cells show loss of the indicator from the cytoplasm during calcium-mediated exocytosis.17 Loss of indo-1 has been observed in isolated muscle cells exposed to oxygen radicals,18 and it is possible that the nitric oxide radical, which is thought to be produced in response to ionomycin, has similar effects. Calibration Procedure Calibration of myocyte [Ca2"]i is feasible if there is no significant calcium-dependent fluorescence from nonmyocytes. Calibration was undertaken whenever the response to bradykinin was shown to be absent. The calibration procedure was similar to that reported previously.19 This method involves determination of maximum (Fm,a) and minimum (Fmin) fluorescence at the 400±+5 nm emission wavelength using ionomycin. The heart was first infused with 100 mM CaCl2 plus 1.5 ,uM ionomycin to obtain Fm. This solution also contained 5 mM HEPES (pH 7.4) along with 6% fetal calf serum to prevent binding of ionomycin to the tubing. In contrast to low concentrations of ionomycin, this solution produced a sustained contracture that was stronger than the normal systole. The heart was then perfused with a solution containing 1.5 ,uM ionomycin and 100 mM MnCl2. Entry of Mn21 into myocytes was also facilitated by ionomycin, resulting in quenching of indo-1 fluorescence. Fmjn, the indo-1 fluorescence in the absence of Ca +,was then given by the equation Fmin==FMn2+ + O.18(Fmax-FMn2+) where FMn2+ is the fluorescence measured after infusion of MnCI2 and 0.18 is a factor derived from measurements performed in cuvettes.20 The concentration of [Ca2+]; was then obtained as 1527 [Ca2+1] i=Kd(F-Fmin)/(Fmax-F) where F is the fluorescence measured and Kd is 250 nM. In some experiments the fluorescence ratio F400/ F430 was used for calibration. F430 is fluorescence at the in vivo isosbestic wavelength of indo-1.21 The F40J/F430 ratio cancels motion artifact and autofluorescence changes during ischemia.2 For most measurements including Fmax, the F400 and F400/F430 signals can be used interchangeably. However, F400/F430 cannot be used to measure Fmin because of the quenching effect of Mn21 on the F430 signal. Recordings at 400 nm were therefore obtained in all experiments for which a complete calibration was performed. pHi Recordings Recordings of pHi were obtained by perfusing hearts with 2.8 ,M BCECF AM. The fiberoptic apparatus used to measure the fluorescence of BCECF was similar to that used to record indo-1 fluorescence transients. Fluorescence excitation was provided by a 50 W halogen lamp filtered at 490±5 nm, with fluorescence emissions recorded at 530±5 nm. In some experiments, the excitation filter was manually switched between 490±5 and 440±5 nm, the latter being a frequency at which the 530 nm fluorescence emission does not change as a function of pH. Fluorescence excited at 440 nm did not change appreciably during prolonged (1-2-hour) periods of recording and remained constant during infusion of C02-rich saline, suggesting dye loss was minimal during periods of recording in the presence of probenecid (see Reference 13). BCECF AM was dissolved in a dimethyl sulfoxide-pluronic solution (25% wt/vol) and infused into the heart for 30 minutes followed by a 30-minute washout. The final concentration of BCECF AM in the loading solution was 2.8 4uM. This loading procedure caused fluorescence emissions to increase sevenfold to 15-fold (mean, 9.8±1.1-fold; n=5), as compared with autofluorescence (excitation frequency, 490 nm). At the end of each experiment, fluorescence emission was calibrated by exposing the heart to a high [K'] solution containing 10-5 M nigericin, a H+-K' antiporter, which clamps the pHi with buffer pH (pHO) when external and intracellular K' are the same. The calibration solution contained (mM) KCl 150, K2HPO4 2.5, CaCl2 1.0, MgCl2 1.0, glucose 10, and HEPES 20. The calibration solution was adjusted to four different pH values by addition of KOH (1N or 1ON) and infused into the heart until cellular fluorescence reached a new steady state (about 250 ml each). The mean pH values of the four calibration solutions were 7.26+0.07, 6.84±0.08, 6.35 ±0.05, and 5.79±0.09. A fluorescence versus pHi curve was obtained at the end of each experiment, and pHi values were derived by linear interpolation of fluorescence calibrations. 1528 Circulation Research Vol 69, No 6 December 1991 Downloaded from http://circres.ahajournals.org/ by guest on October 13, 2016 Simultaneous Calcium Transient and pHi Recordings In some experiments, indo-1 AM and BCECF AM were loaded simultaneously for 30 minutes followed by a 30-minute washout. Two sets of similar fiberoptic cables were used for recordings of calcium transients and pHi. These sets of cables were positioned so that they recorded from adjacent 1-cm regions of the left ventricular surface. Optical interference between the cable systems was absent because neither signal was affected by switching on or off the lamp providing excitation to the opposite set of cables. Indo-1 fluorescence was recorded only at 400 nm for these experiments since the 550 nm emissions could be contaminated by fluorescence energy transfer in which light emitted by indo-1 (490 nm) produced secondary excitation of BCECF (excitation, 490 nm; emission, 530 nm). This effect would not be present in the 400 nm emissions since the emission spectrum of BCECF falls off sharply at wavelengths less than 500 nm.14 Recordings at the isosbestic wavelength of indo-1 (430 nm) confirmed that the calcium transients recorded at single wavelengths were essentially free of motion artifact (not shown). Experimental Intervention Global ischemia was produced by complete cessation of coronary flow. The temperature of the heart during ischemia was maintained at 30+ 1°C by the use of a humidified warm-air convection system. Acidosis was produced by perfusion of the heart with a hypercarbic saline solution as described previously.2 The hypercarbic saline solution was equilibrated with oxygen and varying amounts of CO2 to obtain pH values at graded intervals between 6.3 and 7.4. The Pco2, Po2, and pH of the hypercarbic solutions were measured with a blood gas analyzer (Corning Instruments) before infusion into the heart. All recordings were displayed on a Gould-Brush strip-chart recorder. Chemicals Probenecid, nigericin, and bovine serum albumin were obtained from Sigma Chemical Co., St. Louis, Mo. Probenecid was initially dissolved as 100 mg/ml 1N NaOH. This solution was further diluted 1:1,000 with saline solution and was used throughout the experiment. Nigericin was initially dissolved in ethanol to yield a stock solution of 10-3 M, which was further diluted in 1 1 high [K'] solution to obtain a final concentration of 10-` M. Indo-1 AM and BCECF AM were obtained from Molecular Probes, Eugene, Ore. Statistics All data are presented as mean+SEM. Statistical significance was determined using Student's t test. Results Isolated perfused rabbit hearts loaded with indo-1 produce calcium transients that are very similar to those observed in isolated myocytes. Figure 1 shows 100F IT' E E 0L g 1.5 0 U- '-6 0 ,c u- i.o L 100_ 0 0 ll1 L' 0 sec 1 FIGURE 1. Calcium-dependent fluorescence transients recorded from the epicardial surface of a rabbit heart after infusion of indo-1 AM into the extravascular space. Binding of calcium to indo-1 causes an increase in fluorescence at 400 nm (F400, middle tracing) and a decrease in fluorescence at 550 nm (F550, bottom tracing). The fluorescence ratio, F400/ F550 (top tracing), shows calcium transients with a rapid upstroke and smooth decay. Movement artifact present in the individual tracings is canceled in the ratio. Recordings differ from those obtained by arterial loading insofar as the transients represent a larger percentage of the baseline fluorescence: 17% of end-diastolic fluorescence at 400 nm and 16% of end-diastolic fluorescence at 550 nm. beat-to-beat changes in indo-1 fluorescence recorded from the epicardial surface of the left ventricle. For this recording indo-1 AM was infused into the extravascular space within the field of the optical probe. Resulting calcium transients had rapid upstrokes and a slight distortion of the falling phase, which is due to motion artifact and is canceled in the ratio. Compared with those in arterially loaded hearts, calcium transients obtained by extravascular infusion of indo-1 AM are twofold to threefold larger in proportion of total fluorescence. Thus, the transients shown in Figure 1 represent 17% and 16%, respectively, of the end-diastolic fluorescence at 400 and 550 nm. Approximately one third of the diastolic fluorescence in Figure 1 is not calcium dependent (autofluorescence plus nondeesterified indo-1 AM), as shown by infusion of Mn'+ and ionomycin at the end of the experiment. The phasic change in calcium-dependent fluorescence of each beat is therefore about 25% of the total indo-1 fluorescence signal. A change of this magnitude would be expected if 1) indo-1-free acid is primarily confined to the cytoplasm of the cardiac myocytes; 2) values of [Ca'+]i in systole and diastole are Mohabir et al Ischemia and Hypercarbic Acidosis in Rabbit Hearts CONTROL m BRADYKININ 80 [ cm I E E C UC) IL 0 11' 0.75 U0 'I' 0.50 - .LU.ri.J.J LfLJ&.L F400 r~~~~~~r r ........................................ 1 0 sec 0 1 sec Downloaded from http://circres.ahajournals.org/ by guest on October 13, 2016 FIGURE 2. Effect of bradykinin (10-5 M) on calcium transients and contraction in a heart loaded with indo-1AMby the extravascular infusion technique. Bradykinin causes a parallel elevation of the systolic and end-diastolic level of the calcium transients, which is maximal about 30 seconds after the onset of the effect. There is no change in the amplitude or diastolic level of the contraction (top tracing). There is also no change in the amplitude or shape of calcium transients recorded at fluorescence 400 nm (F400, bottom tracing) or 550 nm (F550, not shown). The middle tracing shows calcium transients displayed as the F400/F550 ratio. Dotted lines in the right panel show original end-diastolic signals. consistent with those measured in isolated myocytes; and 3) resulting fluorescence changes are consistent with in vitro spectroscopy. For example, published spectra of indo-120 show a 26% increase in fluorescence at 400 nm as [Ca2+]i increases from 300 to 600 nM. Methods to Eliminate the Nonmyocyte Components of Indo-1 Fluorescence Endothelial cells are a major source of nonmyocyte fluorescence in hearts loaded with indo-1 AM by aortic perfusion.16 This conclusion is based on the ability of bradykinin to produce a large upward shift in the baseline level of the calcium transients, even though it has no effect on myocyte [Ca2+]1.16 To determine whether extravascular infusion of indo-1 AM prevents nonmyocyte uptake, we administered bradykinin (10-` M) after completion of the loading procedure. In one of 12 hearts, there was no response to bradykinin. In the other 11 hearts, a response was present, which was smaller than that in hearts loaded by aortic perfusion. As shown in Figure 2, the peak response to bradykinin (right panel) is typically one half the amplitude of the calcium transient. Bradykinin does not change the shape or net amplitude of calcium transients at 400 or 550 nm (bottom tracing). This suggests that effects of bradykinin are confined to nonmyocytes. Several strategies were used to eliminate the remaining bradykinin response, the most successful of which was infusion of low concentrations of ionomy- 0 0 LL CONTROL 75 [ 1529 BRADYKININ OL 075 0.55 1 _- 1 0 1 sec sec FIGURE 3. Absence of a bradykinin response in a heart that has been pretreated with 100 nM ionomycin for 5 minutes. Ionomycin elevates calcium transients in the fluorescence ratio (F40,/F550) but has no effect on ventricular pressure or on the net amplitude of calcium transients at 400 nm or 550 nm (signals not shown). Addition of 10-5 M bradykinin for 30 seconds in the continued presence of ionomycin has no effect on either the calcium transients or contraction. 0 cin (100 nM). Low concentrations of calcium ionophores cause endothelium-dependent relaxation in vascular smooth muscle resulting from elevation of endothelial cell [Ca2"]j, which leads to release of endothelium-derived relaxing factor.22 Figure 3 shows calcium transients and ventricular contraction in a heart that had been infused with 100 nM ionomycin for 5 minutes. Infusion of ionomycin caused a sustained upward displacement of the F4W/ F550 recording. Systolic and end-diastolic pressures were unaffected, suggesting that the changes in fluorescence were confined to nonmyocardial cells. These observations indicate that bradykinin and ionomycin act on the same population of cells and that ionomycin can prevent the bradykinin response by raising [Ca2+]i to a ceiling value. Block of the bradykinin response is reversible if ionomycin is removed from the perfusate within 5-10 minutes. However, prolonged infusion of ionomycin (45 minutes) causes permanent unresponsiveness to bradykinin that does not revert in ionomycin-free saline. The basis for this phenomenon is uncertain, but several factors point to loss of indo-1 from nonmyocytes. In one heart (used subsequently for Figure 4), ionomycin pretreatment caused reductions of 29% and 38% in baseline fluorescence at 400 and 550 nm. This improved the signal-to-noise ratio and caused a corresponding increase in the F4J/F550 phasic transient, but there was no increase in contraction strength. This relative increase in the transient component of fluorescence does not occur if ionomycin is omitted from the perfusate. Calibration of [Ca2`]i Transients in Bradykinin- Unresponsive Hearts Fluorescence transients that are not affected by bradykinin are considered myocyte specific and can be calibrated. Figure 4 shows changes in 400 nm fluorescence in a bradykinin-unresponsive heart infused with high calcium saline (100 mM CaCl2, zero 1530 Circulation Research Vol 69, No 6 December 1991 lonomycin, 100 mM Ca2+ Fmax 2 1000 + -. 3001--= m 100 0~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ 20 0 60 40 sec FIGURE 4. Calibration of [Ca2"]i transients in a heart rendered unresponsive to bradykinin. Superficial myocytes were loaded with indo-1 AM by extravascular infusion, which was followed with 100 nM ionomycin for 45 minutes. This procedure caused a relative increase in the transient component offluorescence (see text). Bradykinin was infused 15 minutes after washout of ionomycin, with no effect on fluorescence. Calibration was performed 30 minutes later as follows: First, the heart was infused with a 100 mM CaC12 solution containing 1.5 ,M ionomycin. This solution caused a sustained contracture and increased the fluorescence signal at 400 nm to a maximum level, F,.. Then the zero calcium level (Fmin) was obtained by infusion of 100 mM MnCl2 plus ionomycin (see text). The position of Fma,.. relative to the calcium transients and the resulting values of [Ca2+]i are similar to results obtained in single cardiac myocytes. Downloaded from http://circres.ahajournals.org/ by guest on October 13, 2016 sodium) containing ionomycin (1.5 ,uM). The highcalcium saline produces sustained contracture and elevation of the fluorescence signal to Fm,,. As in isolated myocytes,19 the displacement of Fm,, above the diastolic baseline is approximately three times the amplitude of the calcium transients. This result contrasts with findings in intact heart loaded by arterial infusion of indo-1 AM, for which the displacement of Fma above the baseline is 10 times larger than the calcium transients (Figure 3 of Reference 1). Calibration of indo-1 fluorescence in Figure 4 gives a peak [Ca2"]i value of 642 nM and a diastolic [Ca2+]i value of 333 nM. Similar results have been obtained in eight hearts for which the mean systolic [Ca2+]i is 626+34 nM and mean diastolic [Ca2+]i is 313+ 19 nM. Values are similar in one heart that did not require infusion of 100 nM ionomycin to become unresponsive to bradykinin. on [Ca2"]i Transients The effects of ischemia were studied in hearts loaded with indo-1 by the extravascular route that did not respond to bradykinin. Figure 5 shows the effect of 100 seconds of ischemia in such a heart where ionomycin (100 nM) is present before and during the recording. Ischemia produces an increase in the systolic and end-diastolic levels of the [Ca2"]i transients together with broadening of the transients and an increase in net amplitude (Figure 6). The increased amplitude of the calcium transients is discernible in single wavelength recordings (Figure 6, bottom tracing), which confirms that this change arises from the myocytes. Elevation of end-diastolic [Ca2"]i is also myocyte specific since this response cannot be mimicked by pharmacological stimulation of nonmyocytes (i.e., by bradykinin). Ninety seconds of ischemia increased peak systolic [Ca2"]i from 609±29 to 1,341±159 nM (p=0.005) Effects of Ischemia ISCHEMIA i REPERFUSE 75 E o ..... 0.85 _ o U- U- MEmb . _ 0.60L --------------- -------- .~~~ 0 0.5 1.5 1.0 2.0 2.5 min FIGURE 5. Effect of ischemia on calcium transients in a bradykinin-unresponsive heart. Ionomycin (100 nM) is present in the perfusate at the onset of ischemia and for 15 minutes before ischemia. Ionomycin prevented elevation of the calcium transients by bradykinin, as shown in Figure 3. Ischemia is produced by cessation of coronary perfusion for 90 seconds while the heart is beingpaced at 180 beats/min by an epicardial plunge electrode. Ischemia produces a prompt decline in systolic pressure along with progressive elevation of the calcium transients (shown by the fluorescence ratio, F4JF550). The net amplitude of the calcium transients is also increased. Reperfusion causes return of both signals to their original level but with a temporary increase in end-diastolic pressure that may be related to the persisting elevation of [Ca2"]j. The recording is interrupted to obtain fast time base records. Mohabir et al Ischemia and Hypercarbic Acidosis in Rabbit Hearts CONTROL CD ISCHEMIA E 0 1.2 r tEw 75 LW L I E 1531 z 0 W O_ c) W a: 0 1.1 k ° 0.85 D LL U11 0 W l,' o o N 0.60 -J 0 z 1.0 L F400 .._* \------ 0 10 5 15 min r 0 1 sec 0 1 sec Downloaded from http://circres.ahajournals.org/ by guest on October 13, 2016 FIGURE 6. Same experiment as Figure 5 but at a faster time base. Left panel: Recordings before ischemia. Right panel: Recordings at 80 seconds of ischemia. Besides elevation of the systolic and diastolic levels of the transients, the transients are broadened during ischemia and their net amplitude increases. These changes are seen in the fluorescence recording at 400 nm (F400, bottom tracing) as well as in the F40o/F550 ratio (middle tracing). Changes in the net amplitude and shape of the calcium transients must arise from the cardiac myocytes. Elevation of the end-diastolic level of the transients is also ascribed to the myocytes because changes in nonmyocyte [Ca2"]i are not demonstrable in the presence of ionomycin (same experiment as Figure 3). while increasing end-diastolic [Ca2"]i from 315±25 to 553±52 nM (p=0.006) (n=5). The rise in diastolic [Ca2+]i is unlikely to be an artifact of nonmyocyte stores of indo-1. If such stores existed, they would spuriously elevate Fmax (see Figure 4), so that systolic [Ca21]i before ischemia would be implausibly low. Another source of potential artifact besides ischemia is a change in autofluorescence. Autofluorescence changes have been measured in a previous study2 and found to be significantly less than changes in indo-1 fluorescence during ischemia. After 90 seconds of ischemia, the change in autofluorescence at 400 nm, measured before loading with indo-1, was 37% of the fluorescence change during a comparable trial after loading. Taking this value as typical, it is then possible to determine the net change in indo-1 fluorescence at 400 nm for a group of ischemic hearts. From this net fluorescence change, a corrected mean value for diastolic and systolic [Ca2+]i can be obtained. Resulting values for the five ischemic hearts mentioned above were 444 nM for end-diastolic [Ca2+]i and 965 nM for peak systolic [Ca2+]j. These values represent an increase of 41% and 58%, respectively, over the preischemic values. The effects of longer periods of ischemia were also examined. Figure 7 shows the peak systolic value of the calcium transient during 15 minutes of global ischemia in five hearts. The initial increase in the transient was maximal at about 2 minutes of ischemia FIGURE 7. Mean systolic fluorescence ratio in five hearts during 15 minutes ofglobal ischemia. The systolic fluorescence ratio from each heart is normalized to the corresponding ratio value at the onset of ischemia. Ischemia produces a prompt increase in peak systolic [Ca2"]i by about 2 minutes of ischemia. This is followed by a gradual decline in [Ca2+]i between 2 and 5 minutes and then a progressive secondary rise between 5 and 15 minutes. and was followed by a slow decline to an intermediate level (2-5 minutes). Then there was a secondary increase that reached or exceeded the 2-minute level by 15 minutes of ischemia. These results indicate that 15 minutes of global ischemia produces two phases of [Ca2+]i increase. The sequence of changes in Figure 7 was similar in hearts loaded with indo-1 AM by intravascular and extravascular infusion. However, the changes shown for the systolic fluorescence ratio are not representative of diastolic values or of time-averaged [Ca21]j. The reason for this is that block of conduction or stimulus capture reduces the frequency of calcium transients by one half after 3-5 minutes of ischemia. Reduced frequency of calcium transients causes [Ca2+]i to fall to a lower level at end diastole and also increases the duration of diastole as a fraction of the cardiac cycle. Thus, while time-averaged [Ca21]i has not been calculated from our data, the fall in this value between 2 and 5 minutes of ischemia must be more pronounced than the fall in peak [Ca2]1i. It is therefore possible that the timeaveraged [Ca2+]i measured at 5 minutes of ischemia would not be elevated compared with preischemic measurements.9,10 Effects of Ischemia on pH, Cytosolic acidification during ischemia may be a causal factor responsible for the associated increase in cytosolic calcium. To correlate the time course of changes in intracellular calcium transients with changes in pHi during ischemia, hearts were loaded with the fluorescent pHi indicator BCECF. Loading with BCECF had no significant effects on left ventricular developed pressure. Phasic fluorescence changes in the 530 nm emission signal were generally Circulation Research Vol 69, No 6 December 1991 1532 0C02 IC) 100[ v[ 722r C02 OFF . I 6.8 00 c 0 I 6.0[ 7.0 -. 0 2 1 !8 6.4 3 min FIGURE 8. Effects ofinfusion of an acidic, hypercarbic saline solution (pH 6.72) on left ventricular pressure (top tracing) and pHi in an isolated rabbit heart loaded with 2', 7'-bis(carboxyethyl)-5(6)-carboxy fluorescein. Perfusion with hypercarbic saline produced a rapid decrease in left ventricular pressure and pHI,. The pHi remained stable after 1 minute of perfusion with C02-rtich saline and retumed toward the normal value when perfusion with normal saline was resumed. 6..L 0 Downloaded from http://circres.ahajournals.org/ by guest on October 13, 2016 10 minutes, and 6.11±0.04 after 15 minutes. Similar values for the pHi decrease during ischemia have been observed using other methods.24-26 Simultaneous Recordings of Calcium Transients and pHi Figure 1lA shows the effects of intracellular acidification with CO2 on the calcium transient (middle tracing), left ventricular pressure (top tracing), and pHi (bottom tracing) in a heart loaded with both indo-1 and BCECF. Acidosis (pH. 6.88) caused a rapid decrease in contraction strength along with a decrease in pHi to 6.85. However, this level of intracellular acidification did not produce any elevation of the calcium transient. The pHi of 6.85 achieved in Figure 1lA is similar to values obtained after 2 minutes of ischemia (6.83 ±0.02 in Figure 10). This observation suggests that the decrease in pH, cannot explain the elevation of the calcium transients that occurs during the first 2 minutes of ischemia. In contrast, a reduction of pHi of the magnitude shown would be sufficient to reduce contraction strength during the initial minutes of ischemia. The experiment in Figure 1lA shows an excellent temporal correlation between pHi and the reversible decrease in contraction strength. Furthermore, the absence of any change in the calcium transients suggests that the ISCHEMIA I1 6 I[ 7 ..................... --_ L 0 1 2 3 4 min 15 FIGURE 10. Effects of prolonged ischemia on cytosolic pH (mean+±SEM) in four isolated rabbit hearts. Cytosolic pH values for each heart were determined by calibration with a high [K'] solution and nigericin at the end of the experiment. Ischemia caused a progressive decline in cytosolic pH which reached a value of 6.11+±.04 after 15 minutes. less than 3% of the total signal, which is substantially smaller than the fluctuations related to pH. The ability of BCECF to monitor pHi in the intact heart could be confirmed by perfusion of the heart with C02-rich saline. As shown in Figure 8, perfusion with hypercarbic saline (pH 6.16) produced a rapid decrease in contractility, which occurred synchronously with the increase in BCECF fluorescence. Calibration of the fluorescence recording shows that pH, reached a steady-state value of 6.0 after about 1 minute of perfusion with hypercarbic saline and returned to baseline value when perfusion with normal saline solution was resumed. Of particular importance is the fact that very small changes in pH, (less than 0.1 unit) can substantially diminish contraction strength. Figure 9 shows the effects of 15 minutes of global ischemia on left ventricular pressure (top tracing) and pHi (bottom tracing) in an isolated rabbit heart. The pHi of the heart under normal conditions was 7.08±0.04 (n=10), which is in good agreement with the pHi recorded in cardiac muscle by other methods.5 When the heart was made ischemic, both pHi and contraction strength promptly declined with a similar time course, suggesting that they are causally related. Figure 10 shows the mean pHi values in four hearts subjected to 15 minutes of global ischemia. The mean control pHi (t=0) is 7.03+0.06. During global ischemia, there was a monotonic decrease in pHi, reaching values of 6.83+0.02 after 2 minutes, 6.32±0.01 after 1 I 10 DURATION OF ISCHEMIA (min) 5 14 FIGURE 9. Effect of a 15-minute episode of ischemia on left ventricular pressure (top tracing) and pHI (bottom tracing). Ischemia produced a prompt decrease in left ventricular pressure and a progressive decline in pHI,. pHI, decreased to 5.9 after 15 minutes of ischemia. pHi values were derived from a calibration curve obtained at the end of the experiment. The calibration procedure in15 volved the use of a high [K'] solution containing nigericin, which was adjusted to various pH values. Mohabir et al Ischemia and Hypercarbic Acidosis in Rabbit Hearts ranged from 6.55 to 6.76 (mean, 6.65 ±0.05). Thus the pHi threshold for calcium transient elevation in these hearts is bounded by the mean values of 6.65±0.05 and 6.83±0.03. The existence of a pHi threshold for calcium transient elevation is further shown by the delay in calcium transient elevation that occurs when pHi barely exceeds the threshold value. The steady-state pHi achieved in Figure liB is 6.76, which is only slightly more acidic than the pHi value of 6.83, which did not elevate the calcium transients in Figure 1lA. The greater acidification in Figures 11B and 12 produces elevation of both systolic and diastolic [Ca2"]i along with broadening of the peak (Figure 12). However, there is a delay in the effects of pHi on the calcium transients so that no elevation of the transients occurs until 45 seconds after pHi has begun to decline. Furthermore, changes in the calcium transient occur slowly so that an additional 2.5 minutes is required for the full effect to become apparent (Figure 12). These observations confirm that the degree of acidification observed during the first 2 minutes of ischemia (Figure 10) does not account for the concomitant elevation of the calcium transients. Also, the disparity between the time course of changes in pHi and indo-1 fluorescence confirms that the latter does not reflect a direct effect of protons on the fluorescence properties of indo-1. TABLE 1. Threshold pHi Change Associated With Elevation of Calcium Transients No [Ca2"]i elevation [Ca2"]i elevation Heart No. pHi pHi pH. pH., 1 6.40 6.55 6.78 6.79 2 6.60 6.70 6.80 6.89 3 6.31 6.60 6.51 6.77 4 6.76 6.75 6.90 6.88 6.51 6.65 6.75 6.83 0.10 0.05 0.08 0.03 For each heart, the right two columns show the lowest pH. and pH, values that failed to produce elevation of the calcium transients. The left two columns show the highest pH,, and pH, values that do produce elevation of the calcium transient. Mean SEM Downloaded from http://circres.ahajournals.org/ by guest on October 13, 2016 decrease in contraction strength may be due to a direct effect of pHi on the myofilaments. The result in Figure 11A suggests that for any given heart, there is a threshold change in pHi at which elevation of the calcium transients first occurs. This possibility has been explored systematically in four hearts loaded with both indicators and then infused with a series of four to six increasingly hypercarbic solutions whose pH values differed by 0.15-0.40 pH units. For the four hearts, the lowest pHi that failed to elevate the calcium transients ranged from 6.77 to 6.89 (mean, 6.83+0.03; Table 1). In the same hearts, the highest pHi value at which elevation of the calcium transients was discernible Discussion The principal objective of these experiments was to compare calibrated measurements of [Ca2+]i and pHi FIGURE 11. Panel A: Effects of hypercarbic saline (pH 6.76, Pco2 130, Po2 504) on left ventricular pressure (top tracing), cytosolic calcium transients (F400, middle tracing), and intracellular pH (bottom tracing) in a heart loaded simultaneously with indo-1 and 2', 7'-bis(carboxyethyl)-5(6)-carboxyfluorescein. Perfusion with this CO2 mixture decreased left ventricular pressure and pHI (to 6.85). However, the change in pH, was insufficient to cause an elevation of the calcium transients. Panel B: Effects of C02-enriched saline (pH 6.75) on the left ventricular pressure (top tracing), calcium transient (F4e, middle tracing), and pH, (bottom tracing). Perfusion with C02-enriched solution decreased left ventricular pressure and pHi (to 6.76) and caused delayed elevation of the calcium transient. Elevation of the calcium tran- A C02 [0 m100 _ C02 OFF _F E F400 -- 6.0 f7 -- -- w- 11 ---rl. 1 -, 7.0- 30 0 60 90 sec 120 B COO.j: I 100 E C02 OFF [_ 0 E uu Ae -_. sients associated with a 34% inin the left ventricular developed pressure. Resumption ofperfusion with normal saline caused all recordings to return to normal within 8 minutes. crease 0 1 2 min 4 5 1533 6 8 was Circulation Research Vol 69, No 6 December 1991 1534 the effect of bradykinin-induced fluorescence changes. In rare cases extravascular loading is sufficient to eliminate the bradykinin response. C02 CONTROL cD 100[< F400 6.0 7.0 0 0.5 sec 1.0 0 0.5 1.0 sec FIGURE 12. Same experiment as Figure I1B but with faster speed. With pHI 6.76 the systolic and diastolic level of the calcium transient (F400) is elevated. The transient is also broader and its decay ends more abruptly. sweep Downloaded from http://circres.ahajournals.org/ by guest on October 13, 2016 during global ischemia in the rabbit heart. A threepart strategy has been used. First, methods were developed for calibrating the indicators indo-1 and BCECF in the intact heart. Second, BCECF was used to determine the time course of cytosolic acidification during global ischemia. Third, [Ca2"]i and pHi were monitored simultaneously in hearts acidified with hypercarbic saline to determine whether the degree of acidification seen with ischemia could explain quantitatively the rise in [Ca'+1i. The usefulness of this approach is evident from the temporal disparity in the two measurements and from the existence of a threshold pHi that must be surpassed for [Ca'+]i to rise. Calibration of Indo-1 in the Intact Heart A major difficulty in interpreting the indo-1 fluorescence signals in the intact heart has been the lack of a successful calibration technique. Without plausible measurements of systolic and diastolic [Ca'+]i it is difficult to prove that calcium-dependent fluorescence changes are confined to the cytoplasm of the cardiac myocytes. The two most obvious sources of nonmyoplasmic indo-1 would be nonmyocardial cells, such as endothelial cells,16 and organelles, such as nuclei or mitochondria.27 Conversely, if calibration of systolic and diastolic [Ca'+Ii gives values comparable to those in single myocytes, then most if not all the indo-1 in the heart must be localized within the cytoplasm of cardiac myocytes. Our present work suggests that calibration of myocyte calcium transients is not possible in hearts loaded with indo-1 AM by arterial perfusion. The reason for this is significant uptake of indo-1 AM by cells in the vessel wall that are sensitive to bradykinin. These cells include endothelial cells and possibly other cells, such as smooth muscle cells. Nonmyocyte fluorescence can be minimized by using an extravascular loading technique. Extravascular loading increases the magnitude of calcium transients relative to total fluorescence and to F.., and also minimizes Potential Sources of Artifact With Indo-1 Two other sources of artifact must be considered in interpreting indo-1 results: a change in myoglobin screening and mitochondrial uptake of indo-1 AM. In the case of myoglobin screening, deoxygenation of myoglobin would increase the perceived fluorescence at 400 nm and decrease the fluorescence at 550 nm. The importance of this effect would depend on light penetration through the tissue. Several observations indicate that changes in screening are not responsible for effects of ischemia on indo-1 fluorescence. First, ischemic trials performed in the absence of indo-1 do not change the F40/ F550 ratio (Figure 4B of Reference 2). If myoglobin screening were important, the effects of ischemia on the indo-1 fluorescence and autofluorescence ratios should be similar. This point can be made even more clearly if the heart is perfused with cell-impermeant indo-1-free acid, so that indo-1 fluorescence greatly exceeds autofluorescence. Ischemia cannot change the calcium saturation of indo-1 under these conditions, and we observe no significant change in the F400 fluorescence level or in the F400/F550 ratio. This confirms that ischemia does not alter the screening of indo-1 fluorescence in our experiments. Finally, the effect of ischemia on 520 nm emissions has been studied in hearts loaded with indo-1 AM; 520 nm is an isosbestic wavelength for the myoglobin screening effect (R. Balaban, personal communication, 1989). Ischemia produces a decrease in fluorescence at 520 nm, similar to that observed at 550 nm. This observation further shows that the effect of ischemia on indo-1 fluorescence is not an artifact of tissue screening. A second source of potential artifact is trapping of indo-1 AM in mitochondria. Although previous studies indicate that very little of the Mn2'-quenchable fluorescence resides in mitochondria (Reference 2), it is still possible that an increase in mitochondrial free calcium could contribute to elevation of the F400/ F550 ratio. Such an event would be of physiological importance insofar as it would represent a net transfer of calcium from other organelles or from the extracellular space. Nonetheless, it is clear from the shape of the transients that at least part of the elevation in baseline during ischemia is due to a rise in cytosolic calcium. Transients recorded during ischemia are falling faster at the onset of the next stimulus than are the preischemic transients (see Figure 6). It follows that free calcium in the cytosolic compartment at end diastole is farther away from the resting level during ischemia than during control transients. Incomplete reuptake of calcium eventually leads to [Ca'+]i alternans, in which systolic and diastolic calcium fluctuate from beat to beat.2 These observations confirm that elevation of the baseline of the Mohabir et al Ischemia and Hypercarbic Acidosis in Rabbit Hearts calcium transients during ischemia is at least partly due to elevation of [Ca2+]i. Downloaded from http://circres.ahajournals.org/ by guest on October 13, 2016 Time Course of the [Ca2+]i Increase During Ischemia Our recordings indicate that intracellular calcium increases very early during cardiac ischemia.1 2'9-11'28 We previously reported that brief periods of ischemia produce elevation of calcium transients that reaches a plateau after 90 seconds.1'2 In these studies, ischemia caused an increase in both systolic and diastolic levels of the transients. The rise in [Ca2+]i occurred at a time when contraction strength was falling. A similar observation has been made in ischemic ferret hearts loaded with aequorin by subepicardial injections.28 In that model, an increase in systolic and diastolic [Ca2+]i begins within 2 minutes and coincides with decay of contraction strength. An increase in time-averaged [Ca2+]i during the first 10 minutes of ischemia has also been recorded using the calciumsensitive nuclear magnetic resonance probe 5F BAPTA.9,10 An increase in [Ca2+]i within the first 5 minutes was not detected with this technique but might have been missed owing to the length of time required for signal acquisition and to the transient fall in [Ca2+]i that is seen in Figure 7. In the present study, we have extended our experiments with indo-1 to longer periods of ischemia. We found that with prolonged ischemia, there is partial decline of the calcium transients from the level observed at 90 seconds, followed by a slow increase between 5 and 15 minutes of ischemia. The observation of a progressive increase in [Ca2+]i between 5 and 15 minutes of ischemia is consistent with the SF BAPTA measurements. Cytosolic Acidification as a Potential Cause of the [Ca2+J1 Increase During Ischemia There is evidence that the amplitude of calcium transients in cardiac muscle fibers can be increased by cytosolic acidification achieved with either C02 or lactic acid.2'67 Initial results with aequorin failed to show an increase in diastolic [Ca2+]i during acidification,67 but results with ion-selective electrodes8 as well as indo-12'29 show that acidification can increase the diastolic or resting [Ca2+]i with approximately the same time course as the increase in systolic [Ca2+]i. The likelihood that sufficient acidification would occur to elevate [Ca2 ]i during ischemia is well established from previous studies. Couper et a130 have measured changes in extracellular pH in ischemic rabbit ventricular myocardium and found that extracellular pH can change by 0.5 units during 90-second ischemic trials at a pacing rate of 75 beats/min. Changes in pH. are rate dependent and could occur more rapidly in hearts beating at 180 beats/min. Case et aP31 have measured accumulation of CO2 in ischemic canine myocardium and found that a doubling of myocardial Pco2 can occur during the first 2 minutes of ischemia, with an eightfold increase during the first 8 minutes. CO2 accumulation is believed to be more important than lactate accumulation in 1535 the ischemic heart because lactate accumulates too slowly to account for the fall in pHi.32 The role of cytosolic acidity can be studied most effectively by direct measurements of pHi. BCECF fluorescence is a particularly useful method for making these measurements because recordings are obtained instantaneously and can be compared with analogous recordings of [Ca21]i. Our measurements show that ischemic myocardium becomes detectably acidic within 15 seconds and that pHi declines monotonically by about 1.0 unit after 10-15 minutes of ischemia. The time course and magnitude of the decrease in pHi are comparable to what has been recorded by 31P nuclear magnetic resonance spectroscopy in ischemic hearts containing no indicator.24-26 Correlation of Cystolic Acidification With Elevation of Calcium Transients The present experiments suggest that elevation of the calcium transients does not occur unless pHi falls below a threshold value of approximately 6.75. Furthermore, there is a delay between the fall in pHi and the change in [Ca21]i. In cases for which the degree of acidification barely exceeds the threshold value, [Ca2"]i continues to rise for several minutes after pHi has reached a steady value (Figure 12). These observations are in agreement with in vitro measurements in which pH was found to have no direct effect on the fluorescence of indo-1 over the range of pH values studied in our experiments.2 There are three ways in which cytosolic acidification could produce an increase in [Ca21]i. First, it has been suggested that acidosis enhances the release of calcium from the sarcoplasmic reticulum.7 Alternately, acidosis may cause net uptake of calcium from the extracellular space. According to this scheme, intracellular acidosis would cause an increase in intracellular sodium via the Na+-H+ exchange.33 The resultant increase in [Nat]i would increase intracellular calcium via the Na+-Ca2' exchange.34 Either of the above mechanisms would be consistent with the time delay between cytosolic acidification and elevation of the calcium transients. A third mechanism would be a simple exchange of calcium for protons at cytosolic binding sites.35 This mechanism seems less likely, since a simple exchange of ions at binding sites ought to occur rapidly and should not be associated with a time delay. A major conclusion from the simultaneous indo-1 and BCECF recordings is that cytosolic acidification during the first 2 minutes of ischemia is not sufficient to explain the concomitant elevation of the calcium transients. The mean value of pHi observed at 2 minutes of ischemia in Figure 10 is 6.85, which is above the range of values that is associated with elevation of calcium transients (see Table 1). Furthermore, the peak values of the calcium transients during 15 minutes of ischemia (Figure 7) have a triphasic time course, which differs from the monotonic decrease in pHi during ischemia (Figure 10). This result would not be expected if the early eleva- 1536 Circulation Research Vol 69, No 6 December 1991 Downloaded from http://circres.ahajournals.org/ by guest on October 13, 2016 tion of the calcium transients were a simple consequence of cytosolic acidity. Based on the above results, some other factor must be responsible for producing the increase in [Ca2"] during the first 2 minutes of ischemia. One substance that might mediate this increase is endothelin,36 which is also released by hypoxia and is capable of increasing [Ca2+]i in various cell types. Endothelin can be detected in the serum of patients with recent myocardial infarction37 and has been shown to increase the calcium current and [Ca2+]i in cardiac myocytes.38 The temporary decrease in [Ca21]i after the first 2 minutes of ischemia (Figure 7) could be a consequence of conduction block or could represent "desensitization" of the stimulus producing the early increase. The temporary decrease in [Ca2]]ireaches its nadir at 4-5 minutes of ischemia, which is about the time when pHi crosses the threshold for elevation of calcium transients (Figure 6, Table 1). The secondary increase in [Ca2+]i could therefore be a consequence of progressive acidification. In our study, the disparity noted by Jacobus et al is less apparent. In Figure 11, for example, the acute change in pHi associated with a 50% reduction in developed pressure is 0.1 unit. The mean value obtained in four hearts exposed to hypercarbic saline is 0.14±0.01 unit. This reduction in pHi is similar to what is seen in the first 2 minutes of ischemia. Thus, for a given pHi value, ischemia and acidosis produce similar impairment of contraction. In spite of this similarity, we cannot conclude that acidosis is the only factor producing contractile failure during ischemia. Analysis is complicated by the elevation of the calcium transients during ischemia, which is greater, at least initially, than that produced by acidosis alone. Potential Role of pH, in Ischemic Contractile Failure It is well recognized that ischemia produces a decrease in contractility. The fact that there is a decrease in contractility at a time when [Ca2+]i is elevated suggests that the ability of the myofilaments to produce tension is inhibited during ischemia (see Reference 3 for review). One of the factors that could inhibit the response of the myofilaments to calcium is intracellular acidification. Katz and Hecht39 proposed that intracellular acidification is the cause for decreased tension development during ischemia. Using skinned cardiac cells, Fabiato and Fabiato4 showed that acidosis alters myofilament sensitivity to calcium. Part of this inhibitory effect of acidosis results from competition between hydrogen ions and calcium for the calcium binding sites on troponin C.40 Our experiments support this proposal by showing an excellent temporal correlation between changes in contraction and changes in pHi. In addition, very small changes in pHi (0.1 unit or less) are found to have substantial effects on contraction (see Figure lIA). Thus, the small changes in pHi that occur during the first 2 minutes of ischemia, while not sufficient to affect the calcium transients, could still inhibit contraction. The role of cytosolic acidity in ischemic contractile failure has been investigated by Jacobus et a125 using 31P nuclear magnetic resonance. In their study, left ventricular developed pressure was correlated with pHi during acidification of rabbit hearts with CO2 to determine the magnitude of the change in pHi associated with a 50% decline in developed pressure. The mean change in pHi that produced this effect was 0.22 units. In contrast, when prolonged periods of subtotal ischemia were produced, the steady-state change in pHi associated with a reduction in developed pressure of 50% was 0.09 units. 2. Lee HC, Mohabir R, Smith N, Franz MR, Clusin WT: Effect of ischemia on calcium-dependent fluorescence transients in rabbit hearts containing indo 1: Correlation with monophasic action potentials and contradiction. Circulation 1988;78: 1047-1059 3. Allen DG, Orchard CH: Myocardial contractile function during ischemia and hypoxia. Circ Res 1987;60:153-163 4. Fabiato A, Fabiato F: Effects of pH on the myofilaments and the sarcoplasmic reticulum of skinned cells from cardiac and skeletal muscle. J Physiol (Lond) 1978;276:233-253 5. Poole-Wilson PA: Measurement of myocardial intracellular pH in pathological states. JMol Cell Cardiol 1978;10:511-526 6. Orchard CH: The role of the sarcoplasmic reticulum in the response of ferret and rat heart muscle to acidosis. J Physiol (Lond) 1987;384:431-449 7. Orchard CH, Houser SR, Kort AA, Bahinski A, Capogrossi MC, Lakatta EG: Acidosis facilitates spontaneous sarcoplasmic reticulum Ca2' release in rat myocardium. J Gen Physiol 1987;90:145-165 8. Bers DM, Ellis D: Intracellular calcium and sodium activity in sheep heart Purkinje fibres: Effect of changes of external sodium and intracellular pH. Pflugers Arch 1982;393:171-178 9. Marban E, Kitakaze M, Kusuoka H, Porterfield JK, Yue DT, Chacko VR: Intracellular free calcium concentration measured with 19F NMR spectroscopy in intact ferret hearts. Proc Natl Acad Sci U SA 1987;84:6005-6009 10. Steenbergen C, Murphy E, Levy L, London RE: Elevation in cytosolic free calcium concentration early in myocardial isch- Acknowledgments We would like to thank Dagmar Truckses, Gordon Grant, and David Profitt for assistance in conducting the experiments. References 1. Lee HC, Smith N, Mohabir R, Clusin WT: Cytosolic calcium transients from the beating mammalian heart. Proc NatlAcad Sci USA 1987;84:7793-7797 emia in perfused rat heart. Circ Res 1987;60:700-707 11. Allen DG, Lee JA, Smith GL: The consequences of simulated ischaemia on intracellular Ca2' and tension in isolated ferret ventricular muscle. J Physiol (Lond) 1989;410:297-323 12. Paradiso AM, Negulescu PA, Machen TE: Na'/HW and Cl-/ HCO3- exchange in gastric glands. Am J Physiol 1986;250: G524-G534 13. Paradiso AM, Tsien RY, Demarest JR, Machen TE: Na+-H+ and Cl--HCO3- exchange in rabbit oxyntic cells using fluores- cence microscopy. Am J Physiol 1987;253:C30-C36 14. Rink TJ, Tsien RY, Pozzan T: Cytoplasmic pH and free Mg2` in lymphocytes. J Cell Biol 1982;95:189-196 15. Di Virgilio F, Steinberg JA, Silverstein SC: Inhibition of fura-2 sequestration and secretion with organic anion transport blockers. Cell Calcium 1990;11:57-62 16. Lorell BH, Apstein CS, Cunningham MJ, Schoen FJ, Weinberg EO, Peeters GA, Barry WH: Contribution of endothelial Mohabir et al Ischemia and Hypercarbic Acidosis in Rabbit Hearts 17. 18. 19. 20. 21. 22. 23. Downloaded from http://circres.ahajournals.org/ by guest on October 13, 2016 24. 25. 26. 27. 28. cells to calcium-dependent fluorescence transients in rabbit hearts loaded with indo-1. Circ Res 1990;67:415-425 Almers W, Neher E: The Ca signal from fura-2 loaded mast cells depends strongly on the method of dye loading. FEBS Lett 1985;192:13-18 Josephson RA, Silverman HS, Lakatta EG, Stern MD, Zweier JL: Study of the mechanisms of hydrogen peroxide and hydroxyl free radical induced cellular injury and calcium overload in cardiac myocytes. J Biol Chem (in press) Lee HC, Clusin WT: Cytosolic calcium staircase in culturedmyocardial cells. Circ Res 1987;61:934-939 Hesketh TR, Smith GA, Moore JP, Metcalfe JC: Free cytoplasmic calcium concentration and mitogenic stimulation of lymphocytes. J Biol Chem 1983;258:4878-4882 Peeters GA, Hlady V, Bridge JHB, Barry WH: Simultaneous measurement of calcium transients and motion in cultured heart cells. Am J Physiol 1987;253:H1400-H1408 Grynkiewicz G, Poenie M, Tsien RY: A new generation of Ca2' indicators with greatly improved fluorescence properties. JBiol Chem 1985;260:3440-3450 Singer HA, Peach MJ: Calcium- and endothelial-mediated vascular smooth muscle relaxation in rabbit aorta. Hypertension 1982;4(suppl II):II-19-II-25 Bailey IA, Williams SR, Radda GK, Gadian DG: Activity of phosphorylase in total global ischemia in the rat heart. Biochem J 1981;196:171-178 Jacobus WE, Pores IH, Lucas SK, Kallman CH, Weisfeldt ML, Flaherty JT: The role of intracellular pH in the control of normal and ischemic myocardial contractility: A 31P nuclear magnetic resonance and mass spectrometry study, in Nuccitelli R, Deamer DW (eds): Intracellular pH: Its Measurement, Regulation and Utilization in Cellular Function. New York, Alan R Liss, Inc, 1982, pp 537-565 Ochi S, Ogawa Y, Imai H, Nakazawa M, Imai S: Effects of beta blockers on the fall in pH in the early phase of ischemia in the isolated perfused rat heart: A nuclear magnetic resonance study. J Cardiovasc Pharmacol 1988;11:326-331 Spurgeon HA, Stern MD, Baartz G, Raffaeli S, Hansford RG, Talo A, Lakatta EG, Capogrossi MC: Simultaneous measurement of Ca2 , contraction, and potential in cardiac myocytes. Am J Physiol 1990;258:H574-H586 Kihara Y, Grossman W, Morgan JP: Direct measurement of changes in intracellular calcium transients during hypoxia, 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. 1537 ischemia, and reperfusion of the intact mammalian heart. Circ Res 1989;65:1029-1044 Kohomoto 0, Barry WH: The effects of intracellular acidosis on [Ca+]i, contraction, and 45Ca influx in cultured chick embryo ventricular myocytes (abstract). Circulation 1988; 78(suppl II):II-152 Couper GS, Weiss J, Hiltbrand B, Shine KI: Extracellular pH and tension during ischemia in the isolated rabbit ventricle. Am J Physiol 1984;247:H916-H927 Case RB, Alexis F, Castellana FS: Rate of rise of myocardial pCO2 during early myocardial ischemia in the dog. Circ Res 1979;45:324-330 Ichihara K, Haga N, Abiko Y: Is ischemia-induced pH decrease of dog myocardium respiratory or metabolic acidosis? Am J Physiol 1984;246:H652-H657 Piwinca-Worms D, Jacob R, Horres CR, Lieberman M: Na/H exchange in cultured chick heart cells pHi regulation. J Gen Physiol 1985;85:43-64 Mullins LJ: The generation of electric currents in cardiac fibers by Na/Ca exchange. Am J Physiol 1979;237:C103-C110 Vaughan-Jones RD, Lederer WJ, Eisner DA: Ca2' ions can affect intracellular pH in mammalian cardiac muscle. Nature 1983;301:522-524 Yanagisawa M, Kurihara H, Kimura S, Tomobe Y, Kobayashi M, Mitsui Y, Yazaki Y, Goto K, Masaki T: A novel potent vasoconstrictor peptide produced by vascular endothelial cells. Nature 1988;332:411-415 Miyauchi T, Yanagisawa M, Tomizawa T, Sugishita Y, Suzuki N, Fujino M, Ajisaka R, Goto K, Masaki T: Increased plasma concentrations of endothelin-1 and big endothelin-1 in acute myocardial infarction. Lancet 1989;2:53-54 Lauer MR, Gunn MD, Clusin W: Effect of endothelin on cytosolic calcium and membrane current in single ventricular myocytes (abstract). Circulation 1989;80(suppl II):II-194 Katz AM, Hecht HH: The early "pump" failure of the ischemic heart. Am J Med 1969;47:497-502 Blanchard EM, Solaro RJ: Inhibition of the activation and troponin calcium binding of dog cardiac myofibrils by acidic pH. Circ Res 1984;55:382-391 KEY WORDS * ischemia * calcium transient * intracellular pH indo-1 * BCECF a Downloaded from http://circres.ahajournals.org/ by guest on October 13, 2016 Effects of ischemia and hypercarbic acidosis on myocyte calcium transients, contraction, and pHi in perfused rabbit hearts. R Mohabir, H C Lee, R W Kurz and W T Clusin Circ Res. 1991;69:1525-1537 doi: 10.1161/01.RES.69.6.1525 Circulation Research is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1991 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7330. Online ISSN: 1524-4571 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circres.ahajournals.org/content/69/6/1525 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation Research can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation Research is online at: http://circres.ahajournals.org//subscriptions/