Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Hygiene hypothesis wikipedia , lookup
Neonatal infection wikipedia , lookup
Carbapenem-resistant enterobacteriaceae wikipedia , lookup
Autoimmune encephalitis wikipedia , lookup
Multiple sclerosis research wikipedia , lookup
Infection control wikipedia , lookup
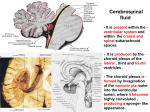
ORIGINAL ARTICLE Corynebacterium striatum meningitis: report of two adult cases Mustafa Sünbül, Şener Barut, Şaban Esen, Cafer Eroğlu and Hakan Leblebicioğlu From the Department of Clinical Microbiology and Infectious Diseases, Ondokuz Mayis University, School of Medicine, Samsun, Turkey Correspondence to: Mustafa Sünbül, MD, Department of Clinical Microbiology and Infectious Diseases, Ondokuz Mayis University, School of Medicine, 55139 Samsun, Turkey. Tel: + 90 362 4576000/2722; Fax: +90 362 4576041; E-mail: [email protected] Microbial Ecology in Health and Disease 2000; 12: 57–59 Corynebacterium striatum is a known saprophytic cutaneous bacterium. However, during the last decade, this organism has been increasingly recognized as a human pathogen. This organism has occasionally been reported as a cause of serious infection in man, however, there are few reports about shunt infections. We describe the clinical and laboratory findings in two patients with C. striatum meningitis after cerebrospinal fluid (CSF) shunt. The two patients had a ventricular external drainage. C. striatum were isolated in CSF from both cases. The patients were treated with intravenous vancomycin, followed by shunt replacement. One patient died on the fifth day of antibiotic therapy. The other patient recovered completely. Key words: Corynebacterium, ventricular external drainage, menigitis. INTRODUCTION Corynebacterium species are members of the normal skin flora and generally found in the environment (1). Except for Corynebacterium diphteriae, Corynebacterium species are usually considered to be contaminants when recovered in the clinical laboratory (2). However, during the last few years Corynebacterium species have been increasingly isolated from infectious sites such as blood, catheter tips, urine and cerebrospinal fluid (CSF) as the numbers and survival of severely immunocompromised patients increase as well as the numbers and types of medical devices used in both immunocompromised and immunocompetant patients increase (3). There are few reports of meningitis due to Corynebacterium species in the literature. These are mainly caused by Corynebacterium JK pathogen and related to ventriculoperitoneal shunt infections (4, 5). Up to date, only two reports of central nervous system (CNS) infections due to C. striatum have been published (1, 6). We report two cases of CNS infections due to C. striatum from our hospital with external ventricular drainage. Case 1 A 17 year old man was admitted to the emergency unit of our hospital on 8th November 1998 with the complaint of unconsciousness. As he had pulmonary arrest in the emergency unit he was intubated there. Cranial computerized tomography (CCT) detected a linear fracture on the left © Taylor & Francis 2000. ISSN 0891-060X side of the frontal bone, cerebral contusion and intraventricular hemorrhage. His pupils were myotic and gave weak reaction to light. The day after admission a ventriculostomy was made and external ventricular drainage was established. He was then transferred to the intensive care unit. After 12 days, the ventricular drain was removed. It was inserted again 5 days after as the patient had an hypotensive attack and unisocori developed after removal of ventricular drain. He became febrile two days after reinsertion. Laboratory tests of blood showed a white blood cell count (WBC) of 17600/mm3 and a creatinin phosphokinase activity of 1135 U/dl (N:200 U/dl). The CSF sample was obtained from the drain. The analysis of CSF revealed a WBC count of 220/mm3 (95% neutrophils). The glucose level was 97 mg/dl (simultaneous blood glucose 283 mg/dl), protein 229 mg/dl and chloride 88.8 mEq/L (N:120 – 130 mEq/L). After coccobasillary Gram positive rods were demonstrated on the Gram staining of CSF, intravenous ampicillin and ceftazidim were administered. After 24 hour incubation of a CSF specimen the culture yielded pure growth on sheep blood agar of a Gram positive rod. The microorganism which had an appearance of grayish white and smooth colonies was catalase positive, reduced nitrate and was methyl red positive. This bacterium was identified as C. striatum by using the API Coryne (bioMerieux, France) system. Biochemical characteristics of strain 1 and 2 are shown Table I. Susceptibility testing was performed by disk diffusion technique. Results Microbial Ecology in Health and Disease 58 M. Sünbül et al. of antibiotic susceptibility regarding strain 1 and 2 are shown in Table II. When the bacterium was identified, ampicillin and ceftazidime were stopped and vancomycin (50 mg/kg/gün) therapy was started. On the fourth day of vancomycin therapy the CSF culture of ventricular external drainage yielded C. striatum. On the fifth day of therapy the patient was died. Case 2 A 58-year old women was admitted to neurosurgery department with the complaints of headache, nausea and vomiting. On her physical examination Babinski’s sign was found positive on the left. Magnetic resonance (MR) examination revealed a mass lesion on the left thalamus and temporamandibular region. The patient was operated in neurosurgery department on 17th November 1998. Subtotal mass excision was made. Pathologic diagnosis was reported as oligodendroglioma. The patient developed hemiplegia and aphasia in the postoperative period, and CCT revealed a residual mass lesion in the temporaparietal region and dilatation of ventriculi. An external drainage was placed into the lateral ventricule. Administration of ceftriaxon was continued during the external drainage period since it was started prophylactically before the operation. After insertion of the drain, aphasia disappeared but on the third day patient became febrile. On the fifth day of drainage, the patient was assessed by the infectious disease consultant. During the physical examination she was conscious and oriented. The body temperature was 37.3°C, pulse rate 90/min and arterial blood pressure 140/80 mmHg. She had neck stiffness Table I Biochemical characteristics of strains by API Nitrate reduction Pyrasinamidase Pyrolidonyl arylamidase Alkalen phosphatase Beta glucorinidase Beta galactosidase Alpha glucosidase N acetyl beta glucosaminidase Esculin Urease Gelatine (hydrolysis) Glucose Ribose Xylose Mannitol Maltose Lactose Sucrose Glycogen Catalase Strain 1 Strain 2 Positive Positive Negative Positive Negative Negative Negative Negative Negative Negative Negative Positive Negative Negative Negative Negative Negative Positive Negative Positive Positive Positive Negative Positive Negative Negative Negative Negative Negative Negative Negative Positive Negative Negative Negative Negative Negative Positive Negative Positive Table II Antimicrobial susceptibility patterns of the strains Penicillin Trimethoprim-sulfamethoxazole Ampicillin Norfloxacin Cefuroxime Erythromycin Vancomycin Amoxicillin-clavulanate Fusidic acid Ofloxacin Clindamycin Gentamicin Strain 1 Strain 2 Resistant Resistant Resistant Resistant Resistant Resistant Resistant Susceptible Susceptible Susceptible Susceptible Susceptible Susceptible Susceptible Resistant Resistant Resistant Susceptible Susceptible Susceptible Susceptible Susceptible Intermediate Susceptible and positive Kerning sign and hemiplegia at the right side. WBC of 6900/mm3, hemoglobin 11 gr/dl, platelet 490000/ mm3. Biochemical tests of blood were normal. A CSF sample obtained from the external drainage demonstrated 270/mm3 (98% neutrophils) and 12000/mm3 erythrocytes. Protein level of CSF was 150 mg/dl, the glucose content was 56 mg/dl (blood glucose 92 mg/dl) and chloride 111 mEq/L (N:120 – 130 mEq/L). Cocobasillary Gram positive bacteria were seen on the Gram staining of CSF. Ceftriaxon was stopped and vancomycin (50 mg/kg/day) was started immediately as the treatment of nosocomial Gram positive meningitis. Culture of the CSF yielded abundant growth of Gram positive bacteria which had no hemolysis on blood agar plate; positive catalase and methyl red tests and reduced nitrate. The bacterium was identified as C. striatum by using API Coryne (bioMerieux, France) system (see Table I). The isolate was resistant to penicillin, ampicillin, trimethoprim-sulfamethoxazole, and susceptible to vancomycin and teicoplanin (see Table II). Molecular characteristics of strain 1 and 2 were studied by using arbitrarily primed polymerase chain reaction (AP PCR). Both strains were showed the same pattern (Fig. 1). One day after the assessment of patient, the external ventricular drain was removed. The patient became afebrile within the second day of vancomycin treatment. She improved clinically on subsequent days. Vancomycin was given for 14 days after which she was discharged. DISCUSSION C. striatum is a member of the normal flora that usually colonizes the anterior nares, the skin of the face and the upper part of the body (1, 3). Nondiphtheria corynebacteria cause infections in either immunocompromised patients or patients to whom applied catheters and other medical devices. During recent years, the number of these patients has increased in hospitals and there have been some developments on the identification of coryneform bacteria. Re- Corynebacterium striatum meningitis Fig. 1. It was shown in arbitrarily primed PCR results of strain 1 and 2. Line 1: Molecular weight marker, line 2: strain 1(1/5 DNA dilution). Line 3: strain 2 (1/5 DNA dilution). Line 4: strain 1. Line 5: strain 2. ports of infection caused by definite Nondiphtheria corynebacteria have shown an increase (3, 7). Up to now, meningitis of Corynebacterium species have been mainly due to Corynebacterium JK. Almost all of these infections occured in patients with ventriculoperitoneal shunts (4, 5). Several cases of C. striatum infection have been reported; however, most of these cases were bacteremia or respiratory tract infections (1, 7). To our knowledge, two new reports of CNS infection due to C. striatum have also been published (1, 6). In our report we present two cases of CNS infection due to C. striatum in which the patients had an external ventricular drainage. The fact that there was direct communication between the skin and the CSF through the drainage catheter could explain how microorganisms had easily reached to CSF and caused meningitis. We state that C. striatum has a potential to cause meningitis especially in patients with external ventricular drainage. Drainage was applied twice to the first patient. This 59 patient died. The fact that the patient had severe respiratory failure, conscious and nutritional problems associated with the intraventricular hemorrhage could explain why he died. In addition, it could be a reason that the drainage had not been removed immediately after infection had been diagnosed. The corynebacteria strains were identified by using API Coryne system. We also applied catalase, nitrate reduction and metil red tests to the strains. The possibility of C. striatum was especially increased by the positive methyl red test. Apart from the C. xerosis, colony morphology of the strains was whitish, moist and smooth (7). Their growth was completed by 48 to 72 hours. These features also contributed to the identification of the bacteria (7). Since antibiotic susceptibility, biochemical and molecular characteristic are almost same, these two cases may be considered to be cross infection. As a conclusion, C. striatum is being increasingly described as a potential pathogenic Corynebacterium species. Its presence in clinical specimens should not be overlooked, especially in samples from patients with underlying medical conditions. It has a potential to colonize prosthetic devices or catheters and may cause severe infections of sterile body sites such as meningitis. Clinical microbiologists should give attention to such situations. REFERENCES 1. Weis K, Labbe AC, Laverdiere M. Corynebacterium striatum meningitis: Case report and review of an increasingly important Corynebacterium species. Clin Infect Dis 1996; 23: 1246–8. 2. The aerobic Gram positive bacilli. In: Koneman EW, Allen SD, Janda WM, Schreckenberger PC, Winn WC (eds). A color atlas and textbook of diagnostic microbiology 5th edition. New York, 1997; 651 – 708. 3. Brown AE. Other Corynebacteria and Rodococcus. In: Mandell GL, Bennett JE, Dolin R eds., Principles and practise of infectious diseases.4th edition. New York, 1995; 1872 – 80. 4. Greene KA, Clark RJ, Zabramski JM. Ventricular CSF shunt infections associated with Corynebacterium jeikeium: Report of three cases and review. Clin Infect Dis 1993; 16: 139 – 41. 5. Keren GK, Geva T, Bogokovsky B, Rubinstein E. Corynebacterium group JK pathogen in cerebrospinal fluid shunt infection: Report of two cases. J Neurosurg 1988; 68: 648 – 50. 6. Hoy CM, Kerr K, Livingston JH. Cerebrospinal fluid-shunt infection due to Corynebacterium striatum. Clin Infec Dis 1997; 25: 1486 – 7. 7. Funke G, Von Graevenitz A, Clarridge III JE, Bernard KA. Clinical microbiology of Coryneform bacteria. Clin Microbiol Rev 1997; 10: 125 – 59.