Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
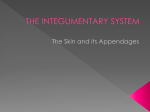
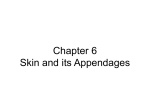
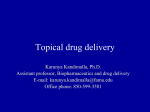
CLINICAL systems of life Anatomy and function of the skin Part 2 – The epidermis Stratum corneum Stratum lucidum Stratum granulosum Stratum spinosum Stratum basale Basement membrane Dermis Fig 1. The layers of the epidermis Author Sandra Lawton, MSc, RGN, OND, ENB 393, RN (Child), is nurse consultant in dermatology, Queen’s Medical Centre, Nottingham University Hospitals NHS Trust. The epidermis is the outer layer of the skin varying in thickness from 0.1mm to 1.4mm (Gawkrodger, 1992) (Fig 1). It consists of a number of layers: l Stratum corneum; l Stratum lucidum; l Stratum granulosum; l Stratum spinosum; l Stratum basale; l Basement membrane. It contains no blood vessels and is dependent on 28 the underlying dermis for nutrient delivery and waste disposal through the dermo-epidermal junction. The epidermis is defined as a stratified squamous epithelium, consisting primarily of keratinocytes in progressive stages of differentiation (Revis and Seagle, 2006). Its prime function is to act as a physical and biological barrier to the environment, preventing penetration by irritants and allergens and loss of water while maintaining internal homeostasis (Gawkrodger, 1992; Cork, 1997). Layers of epidermis The epidermis is composed primarily of layers of densely packed keratinocytes that produce the protein keratin and are the major cells of the epidermis. NT 8 August 2006 Vol 102 No 32 www.nursingtimes.net keywords n Skin n Epidermis n Anatomy and physiology Keratinocytes are formed by division in the stratum basale (basal or germinative layer). As the keratinocytes move up through the stratum spinosum (prickle cell layer) and stratum granulosum (granular layer), they differentiate to form a rigid internal structure of keratin, microfilaments and microtubules (keratinisation). The outer layer of the epidermis, the stratum corneum (horny layer), is composed of layers of flattened dead cells (corneocytes) that have lost their nucleus. These cells are then shed from the skin (desquamation). The complete process from formation to desquamation takes approximately 28 days (Hill, 1994) (Fig 2). Between these cells (corneocytes) there is a complex mixture of lipid and proteins (Cork,1997). These intercellular lipids are broken down by enzymes from keratinocytes to produce a lipid mixture of ceramides (phospholipids), fatty acids and cholesterol. These molecules are arranged in a highly organised fashion, fusing with each other and the corneocytes to form the skin’s lipid barrier against water loss and penetration by allergens and irritants (Holden et al, 2002). The stratum corneum can be visualised as a brick wall, with the corneocytes forming the bricks and the lamellar lipids forming the mortar. Corneocytes contain a water-retaining substance – natural moisturising factor – and so attract and hold water. The high water content of the corneocytes causes these cells to swell, thereby keeping the stratum corneum pliable and elastic, and preventing the formation of fissures and cracks (Cork, 1997; Holden et al, 2002). This is an important consideration when applying topical medications to the skin. Percutaneous absorption Percutaneous absorption refers to the absorption of topical medications and other substances through the epidermal barrier into the underlying tissues and structures, which then transfer to the systemic circulation. Three elements play a role in percutaneous absorption – the features of normal skin, changes in skin barrier function and vascular changes. The stratum corneum (horny layer) regulates the amount and rate of percutaneous absorption (Rudy and Parham-Vetter, 2003). Two of the most important factors affecting percutaneous absorption are skin hydration and environmental humidity. In healthy skin with normal hydration, medicaments can only penetrate the stratum corneum (horny layer) by passing through the tight, relatively dry, lipid barrier between cells. When skin hydration is increased or the normal skin barrier is impaired, as a result of skin disease, excoriations, erosions, fissuring or prematurity, percutaneous absorption will be enhanced (Rudy and ParhamVetter, 2003). NT 8 August 2006 Vol 102 No 32 www.nursingtimes.net Fig 2. The process of desquamation Desquamation 1,000 cells/cm2/hour Stratum corneum 15–20 cell layers References Butcher, M., White, R (2005) The Structure and Functions of the Skin. In: White, R. (Eds). Skin Care in Wound Management: Assessment, prevention and treatment. Aberdeen: Wounds UK. t Two weeks t t Two weeks t Other epidermal cells Keratinocytes make up about 95% of the epidermal cells, the others being melanocytes, Langerhan cells and Merkel Cells (Butcher and White, 2005). Melanocytes – are found in the stratum basale (basal or germinative layer) and are interspersed among the keratinocytes along the basement membrane (dermo-epidermal junction) at a ratio of one melanocyte to 10 basal cells. They produce the pigment melanin, which is manufactured from the amino acid tyrosine, packaged into melanosomes, transported and delivered into the cytoplasm of the keratinocytes (Graham-Brown and Bourke, 1998). The key function of melanin is protection, absorbing ultraviolet radiation and protecting us from its harmful effects. Skin colour is determined not by the numbers of melanocytes but by the number and size of the melanosomes (Gawkrodger ,1992). Skin colour is also influenced by ultraviolet light, genetic factors and hormonal influences (Hill, 1994). Langerhan’s cells – are antigen-presenting cells in the stratum spinosum (prickle cell layer). They represent one part of the body’s immune system and are constantly on the lookout for antigens (microorganisms and foreign proteins) in order to trap them and present them to T helper lymphocytes, thus activating an immune response (Graham-Brown and Bourke 1998, Butcher and White, 2005). Merkel Cells – are only present in very small numbers and are found in the stratum basale (basal or germinative layer). They are closely associated with terminal filaments of cutaneous nerves and seem to have a role in sensation, especially in areas such as palms, soles and genitalia (Gawkrodger, 1992; Butcher and White, 2005). n Cork, M. (1997) The importance of skin barrier function. Journal of Dermatological Treatment; 8: Suppl 1, 7–13. Gawkrodger, D.J. (1992) An Dermatology: An Illustrated Colour Text. Edinburgh: Churchill Livingstone. Graham-Brown, R., Bourke, J.F. (1998) Mosby’s Color Atlas and Text of Dermatology. London: Mosby. Hill, M.J. (1994) Skin Disorders. St Louis: Mosby. Holden, C. et al (2002) Advised best practice for the use of emollients in eczema and other dry skin conditions. Journal of Dermatological Treatment; 13: 3, 103–106. Revis, D.R., Seagle, M.B. (2006) Skin Anatomy emedicine. Available: www.emedicine.com/ plastics/topic389.htm. Rudy, S., Parham-Vetter, P. (2003) Percutaneous absorption of topically applied medication. Dermatology Nursing; 15: 2, 145–152. This article has been double-blind peer-reviewed. For related articles on this subject and links to relevant websites see www.nursingtimes.net 29