Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
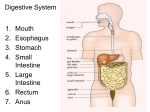
DIGESTIVE SYSTEM ALSO KNOWN AS GI SYSTEM: GASTROINTESTINAL SYSTEM AGE RELATED CHANGES 1. FLOW OF SALIVA DECREASES • Difficulty chewing/swallowing (dysphagia) AGE RELATED CHANGES 2. TASTE BUDS DECREASE -Appetite decreases AGE RELATED CHANGES 3. WEAKENED GAG REFLEX • Risk of Choking AGE RELATED CHANGES 4. REDUCED DIGESTIVE JUICES • Food more difficult to digest affecting absorption INTRODUCTION DIGESTIVE SYSTEM IS RESPONSIBLE FOR THE PHYSICAL AND CHEMICAL BREAKDOWN OF FOOD SO IT CAN BE TAKEN INTO THE BLOOD STREAM AND USED BY BODY CELLS AND TISSUES. SYSTEM INCLUDES THE ALIMENTARY CANAL AND ACCESSORY ORGANS ALIMENTARY CANAL LONG MUSCULAR TUBE BEGINS AT THE MOUTH AND INCLUDES THE PHARYNX, ESOPHAGUS, STOMACH, SMALL INTESTINES, LARGE INTESTINES, RECTUM AND ANUS Alimentary Canal Structures of the GI System Mouth/Oral Cavity Pharynx Esophagus Stomach Small Intestine Large Intestine Rectum Anus •MOUTH OR ORAL CAVITY PHARYNX OR THROAT TUBE THAT CARRIES BOTH AIR AND FOOD CARRIES THE AIR TO THE TRACHEA OR WINDPIPE AND FOOD TO THE ESOPHAGUS ESOPHAGUS MUSCULAR TUBE BEHIND THE TRACHEA RELIES ON A RHYTHMIC, WAVELIKE INVOLUNTARY MOVEMENT OF ITS MUSCLES, CALLED PERISTALSIS, TO MOVE THE FOOD IN A FORWARD DIRECTION STOMACH RECEIVES THE FOOD FROM THE ESOPHAGUS HOLDS FOOD APPROXIMATELY 3-4 HOURS. FOOD TURNS NTO SEMI LIQUID CALLED CHYME SMALL INTESTINE COILED SECTION OF THE ALIMENTARY CANAL ABOUT TWENTY FEET LONG AND ONE INCH IN DIAMETER. ABSORPTION DONE BY VILLI THREE SECTIONS – DUODENUM – JEJUNUM – ILEUM VILLI FINGERLIKE PROJECTONS THAT LINE WALL OF SMALL INTESTINE ALLOW FOOD TO BE ABSORBED OR TAKEN INTO BLOOD DUODENUM FIRST NINE TO TEN INCHES JEJUNUM ABOUT EIGHT FEET LONG FORMS THE MIDDLE SECTION OF THE SMALL INTESTINE ILEUM FINAL TWELVE FEET CONNECTS WITH THE LARGE INTESTINE SMALL INTESTINE OVERVIEW Nutrients are ABSORBED from the small intestine into the blood stream by the VILLI LARGE INTESTINE ABOUT FIVE FEET LONG AND ABOUT TWO INCHES IN DIAMETER FUNCTIONS REABSORPTION OF WATER TRANSPORTATION OF THE WASTE PRODUCTS OUT OF THE ALIMENTARY CANAL SECTIONS OF LARGE INTESTINE (COLON) 1. 2. 3. 4. ASCENDING COLON TRANSVERSE COLON DECENDING COLON SIGMOID COLON RECTUM FINAL SIX TO EIGHT INCHES of alimentary canal STORAGE AREA FOR WASTES ANUS: Evacuation of waste ACCESSORY ORGANS INCLUDE THE LIVER, GALLBLADDER, PANCREAS AND APPENDIX LIVER LARGEST GLAND IN THE BODY LOCATED UNDER THE DIAPHRAGM IN THE UPPER RIGHT QUADRANT OF THE ABDOMEN FUNCTIONS OF LIVER SECRETES BILE REMOVES TOXINS FROM BODY PRODUCES CHOLESTEROL GALLBLADDER SMALL MUSCULAR SAC LOCATED UNDER THE LIVER STORES BILE PANCREAS FISH-SHAPED ORGAN LOCATED BEHIND THE STOMACH PRODUCES PANCREATIC JUICES AND INSULIN DISEASES OF THE DIGESTIVE SYSTEM APPENDICITIS ACUTE INFLAMMATION OF THE APPENDIX USUALLY DUE TO AN OBSTRUCTION AND INFECTION GALLBLADDER CONDITIONS CHOLECYSTITIS-INFLAMMATION OF THE GALLBLADDER CHOLELITHIASIS: GALLSTONES SYMPTOMS FREQUENTLY OCCUR AFTER EATING FATTY FOODS – INDIGESTION, N&V – PAIN UNDER RIB…WHAT SIDE? – JAUNDICE TREATMENT LOW FAT DIET SURGERY LASER TO BREAK UP GALLSTONES CIRRHOSIS CHRONIC DESTRUCTION OF LIVER CELLS ACCOMPANIED BY THE FORMATION Of SCAR TISSUE CAUSES: ALCOHOLISM MALIGNANCY: CANCERS SYMPTOMS DEPEND ON LOCATION: obstruction Indigestion Vomiting Change in stools Blood in stools (old/new) TREATMENT FOR CANCERS SURGERY: COLOSTOMY- CREATION OF ARTIFICAL OPENING IN ABDOMINAL WALL AND BRINGING SECTION OF COLON TO IT FOR ELIMINATION OF STOOL ILEOSTOMY- CREATION OFARTIFICIAL OPENING AND BRINGING SECTION OF ILEUM THROUGH IT HEPATITIS VIRAL INFLAMMATION OF THE LIVER TYPE A OR INFECTIOUS HEPATITIS – HIGHLY CONTAGIOUS – TRANSMITTED IN FOOD OR WATER THAT HAS BEEN CONTAMINATED BY THE FECES OF AN INFECTED PERSON TYPE B/TYPE C – TRANSMITTED BY BLOOD AND SERUM – MORE SERIOUS THAN TYPE A AND CAN LEAD TO CHRONIC HEPATITIS OR CIRRHOSIS OF THE LIVER SYMPTOMS FEVER, LOSS OF APPETITE N&V FATIGUE ENLARGED LIVER JAUNDICE ULCER OPEN SORE ON THE LINING OF THE DIGESTIVE TRACT SYMPTOMS BURNING PAIN INDIGESTION HEMATEMESIS (BLOODY VOMITUS) DARK,TARRY STOOL TREATMENT MEDICATION DIET MODIFICATION ANTIBIOTICS NPO POSSIBLY NG TUBE ULCERATIVE COLITIS SEVERE INFLAMMATION OF THE COLON WITH THE FORMATION OF ULCERS AND ABSCESSES THOUGHT TO BE CAUSED BY STRESS, ALLERGIC REACTIONS TO FOOD, OR AN AUTOIMMUNE REACTION SYMPTOMS WATERY, FREQUENT STOOLS WITH BLOOD, PUS, AND MUCUS WEIGHT LOSS DEHYDRATION FLARE-UPS ARE COMMON TREATMENT DIRECTED TOWARD CONTROLLING INFLAMMATION REDUCE STRESS MAY NEED SURGERY GI BLEED INTERNAL BLEEDING IN DIGESTIVE TRACT: OCCULT BLOOD- HIDDEN BLOOD/NOT SEEN WITH NAKED EYE UPPER GI BLEED- COMING FROM STOMACH AND STRUCTURES ABOVE LOWER GI BLEED-COMING FROM INTESTINES AND STRUCTURES BELOW BLOOD IN GI SYSTEM NEW: BRB OLD: BLACK, TAR LIKE “COFFEE GRINDS” GI BLEED: SYMPTOMS LOWER GI BLEED: (Intestine to rectum) RECTAL BLEEDING (BRB/BLACK TARRY STOOLS) HYPOTENSION DIAPHORETIC GI BLEED: SYMPTOMS UPPER GI BLEED: (Stomach to mouth) VOMITING BLOOD (BRB/COFFEE GRINDS) HYPOTENSION DIAPHORETIC DIAGNOSTIC TEST for OCCULT BLOOD HEMACULT BLOOD TEST: USED TO DETECT BLOOD IN STOOL AND EMESIS LOWER BOWEL CONDITIONS CONSTIPATION- fecal material is hard, dry or sticky DIARRHEA- 3 or more loose stools w/in a certain amount of time Factors that Affect Bowel Function Bed rest Immobility Inadequate exercise Decreased fluid intake Change in environment Abdominal Distention As food moves through tract, gas is formed and is normally expelled from body. If not passed, it accumulates in intestines, enlarging the abdomen C. difficile Bacteria transmitted on HCW hands after they touch feces or contaminated surfaces (faucets, side rails) and can be transmitted to other patients. Feeding Tubes 1. 2. Nasogastric Tube (NG) –goes from nose to stomach Gastrostomy Tube (GT)- goes directly into stomach Nasogastric Tube (NG) Always NPO for tube feedings because of the reasons they are on tube feedings! HOB at least 30 degrees or higher RN inserts NG tube and checks for placement Nasogastric Tube Can be used for: Tube feedings called GAVAGE (mostly short term feedings) Or Suctioning out contents of stomach called LAVAGE GastrostomyTube (GT) Tube for feedings that goes directly into abdomen through a surgical incision. More for long-term feedings HOB at least semi-fowlers