Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
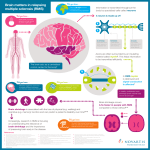
Multiple Sclerosis Nanik “Nayri” Hatsakorzian Pharm.D/MPH Candidate 2014 Touro University – California College of Pharmacy Overview Pathophysiology Forms of MS Hallmark signs and symptoms Diagnosis Current treatments Pathophysiology Chronic inflammatory demyelinating disorder that mostly affects Caucasian young women in their reproductive age. Massive destruction of myelin. MS lesions, is seen upon extravasation of activated leukocytes from the peripheral circulation through BBB into CNS. Autoreactive T-cells recognizing self myelin antigens. Myelin basic protein (MBP) - primed T-cells. The contact between MBPprimed T-cells and microglia leads to induction of NO Excessive NO derived from inducible nitric oxide synthase (iNOS) in glial cells leading to demyelination Persistent oxidative stress is seen even in remission MS patients Oliveira SR, Kallaur AP, Simao AN, et al. Oxidative stress in multiple sclerosis patients in clinical remission: Association with the expanded disability status scale. J Neurol Sci. October 15, 2012; 321(1-2):49-53 Rossi B, Angiari S, Zenaro E, et al. Vascular inflammation in central nervous system diseases: adhesion receptors controlling leukocyteendothelial interactions. J Leukoc Biol. April 2011; 89(4):539-56 Oxidative stress evaluated by tert-butyl hydroperoxide-initiated chemiluminescence (CLLOOH) in patients with relapsing/remittent multiple sclerosis. Oliveira SR, Kallaur AP, Simao AN, et al. Oxidative stress in multiple sclerosis patients in clinical remission: Association with the expanded disability status scale. J Neurol Sci. October 15, 2012; 321(1-2):49-53 Pathophysiology Metalloproteinases (MMPs) & tissue inhibitors of metalloproteinases (TIMPs) MMP/TIMP balance, mRNA stability, and translational TIMP-1/MMP-3 ratio imbalance impairs wound healing, arthritis and cancer metastasis MMP levels are low and well controlled in normal resting adult tissue, and up regulated during development, cell signaling, and remodeling (i.e. wound healing, ovulation, bone growth, angiogenesis) Inflammatory stimuli increase MMP levels leading to tumor invasion and metastasis, RA, periodontal diseases, and atherosclerosis Hove VI, Lemmens K, Van de Velde S, et al. Matrix metalloproteinase-3 in the central nervous system: a look on the bright side. J Neurochem. November 2012; 123(2):203-16 MMP-3: A double edged sword MMP-3 is able to degrade MBP and is up-regulated in the brain prior to the onset of disease, in and around lesions, and in serum of MS patients MMP-3 is highly expressed in astrocytes of corpus callosum suggesting re-myelination via releasing IGF, and removing myelin debris. Time, space, and cell type specific MMP-3 expression seem to have dual function. Acute injury might lead to degeneration whereas later stages of injury up-regulation of MMP-3 might contribute to axonal sprouting, re-myelination and reactive synaptogenesis. Hove VI, Lemmens K, Van de Velde S, et al. Matrix metalloproteinase-3 in the central nervous system: a look on the bright side. J Neurochem. November 2012; 123(2):203-16 Pathophysiology Endothelial adhesion molecules detected in relapse MS patients and have been associated with disease severity and the spreading of the lesions. P – and E – selectin are found in MS lesions and in RR MS patients Monocytes were also identified in the CNS parenchyma and it is believed to play a role in exacerbating MS by providing a source of pro-inflammatory cytokines. Rossi B, Angiari S, Zenaro E, et al. Vascular inflammation in central nervous system diseases: adhesion receptors controlling leukocyte-endothelial interactions. J Leukoc Biol. April 2011; 89(4):539-56 Forms of MS Relapsing-remitting MS: Clearly defined relapses with full recovery or with residual deficit upon recovery. No disease progression during the periods between disease relapses Primary-progressive MS: Disease progression from onset with occasional plateaus and temporary minor improvements Secondary-progressive MS: Initial RR disease course followed by progression with or without occasional relapses, minor remissions, and plateaus Progressive relapsing MS is characterized by progressive disease from onset, with clear acute relapses with or without full recovery. Progression continues during the periods between disease relapses Barten LJ, Allington DR, Procacci KA, Rivey MP. New approaches in the management of multiple sclerosis. Drug Design, Development and therapy. 2010:4 343-366 Hallmark signs & symptoms Visual disturbances (optic neuritis, optic nerve dysfunction, diplopia) Muscle weakness and bladder and bowel dysregulation Trouble with coordination, balance, ataxia Numbness Pins and needles Thinking and memory problem Barten LJ, Allington DR, Procacci KA, Rivey MP. New approaches in the management of multiple sclerosis. Drug Design, Development and therapy. 2010:4 343-366 Diagnosis McDonald criteria Added MRI in 2001, latest update is 2010 About 5% of patients with clinically defined MS show no lesions at the time of diagnosis Cerebrospinal fluid analysis. Oligoclonal bands seen in 90-95% of patients with MS Visual Evoked Potential (VEP) Recording of the nervous system’s electrical impulses. Can provide evidence of scarring National Multiple Sclerosis Society. Diagnosing MS. Accessed on October 14, 2012. http://www.nationalmssociety.org/about-multiplesclerosis/what-we-know-about-ms/diagnosing-ms/index.aspx Treatments Anti-inflammatory Glucocorticoids IV Methylprednisolone Immunomodulatory Betaseron (Interferon-β-1b) and Avonex (Interferon-β-1a) Copaxone (Glatiramer acetate) Tysabri (Natalizumab) Gilenya (Fingolimod) Anti-neoplastic agents Novantrone (Mitoxantrone) Novel treatment Aubagio (Teriflunomide) Corticosteroids IV methylprednisolone Acute attacks or exacerbation 1 gram daily for 3 days, then 21 day tapering oral treatment Pregnancy and lactation Enters breast milk IVMP exposed Pregnant women can contact OTIS Autoimmune Diseases Study Barten LJ, Allington DR, Procacci KA, Rivey MP. New approaches in the management of multiple sclerosis. Drug Design, Development and therapy. 2010:4 343-366 Ontaneda D, Rae-Grant AD. Management of acute exacerbations in multiple sclerosis. Ann Indian Acad Neurol. Oct 2009; 12(4):264-272 Betaseron (Interferon β-1b) Reduce attack rates For RRMS and SPMS only Beneficial effects are seen on MRI MoA is not known exactly, but include enhancement of suppressor T cell activity, reduction of pro-inflammatory cytokines, down regulation of antigen presentation, and reduced trafficking of lymphocytes into the central nervous system. Barten LJ, Allington DR, Procacci KA, Rivey MP. New approaches in the management of multiple sclerosis. Drug Design, Development and therapy. 2010:4 343-366 Goodin DS, Frohman EM, Garmany GP, et al. Disease modifying therapies in multiple sclerosis: Subcommittee of the American Academy of Neurology and the MS Council for Clinical Practice Guidelines. Neurology. January 2002; 58(2); 169178 Clinical pearls RRMS: initial 0.0625 mg (0.25 mL) SQ every other day. Gradually increase dose by 0.0625 mg every 2 weeks Target dose: 0.25 mg (1 mL) every other day SPMS: initial 0.125 mg (0.5 mL) SQ every other day for 2 weeks. Target dose: 0.25 mg every other day Reconstituted solution should be used immediately after reconstitution or within 3 hours if refrigerated Caution Hepatotoxicity Increased risk of infection Injection site reaction, necrosis may occur, injection competency should be evaluated Bone marrow suppression Neuropsychiatric disorders Caution with seizure patients Copaxone (Glatiramer acetate) Reduces attack rates in RRMS patients Beneficial effects are seen on MRI Pregnancy category B MoA: a random polypeptide made up of four amino acids (Lglutamic acid, L-lysine, L-alanine, and L-tyrosine). Antigenically similar to myelin basic protein; induce and activate T-lymphocyte suppressor cells specific for a myelin antigen and Interferes with the antigen-presenting function Barten LJ, Allington DR, Procacci KA, Rivey MP. New approaches in the management of multiple sclerosis. Drug Design, Development and therapy. 2010:4 343-366 Goodin DS, Frohman EM, Garmany GP, et al. Disease modifying therapies in multiple sclerosis: Subcommittee of the American Academy of Neurology and the MS Council for Clinical Practice Guidelines. Neurology. January 2002; 58(2); 169-178 Clinical Pearls RRMS: 20 mg SQ daily Should be refrigerated Not for IV administration Not for patients with mannitol allergy Caution Transient chest pain may occur Injection site lipoatrophy Common post injection systemic reactions include: anxiety, chest pain, dysphagia, flushing, palpitation, urticaria. Can occur several months after initiation as well Tysabri (Natalizumab) MoA: Monoclonal antibody against α-4 integrin molecules. It blocks α4β1 integrin limiting adhesion and transmigration of leukocytes. It also blocks T-lymphocytes migration into the CNS Decrease frequency of relapse and improve measures of disease severity. FDA approval for patients who failed IFNβ or glatiramer therapy Combination treatment with IFNβ-1α therapy reduced MRI activity by 80-90% and clinical activity by 50-70% Clinical trials that study combination therapy (three-armed trial) are not available. Barten LJ, Allington DR, Procacci KA, Rivey MP. New approaches in the management of multiple sclerosis. Drug Design, Development and therapy. 2010:4 343-366 Goodin DS, Cohen BA, et al. Assessment: The use of natalizumab (Tysabri) for the treatment of multiple sclerosis (an evidence-based review): Report of the therapeutics and technology assessment subcommittee of the American Academy of Neurology. Neurology 2008;71;766 Clinical Pearls 300 mg infused over 1 hour every 4 weeks Patient has to be in hospital setting Caution Patient has to be enrolled in Tysabri Outreach Unified Commitment to Health (TOUCH) prescribing program due to association with Progressive Multifocal Leukoencephalopathy PML (a rare demyelinating neurological disorder caused by the reactivation of the JC virus) On January 2012 FDA require patients to test for anti-JC virus antibodies, risk factor to PML. AND since August 2012, FDA mandates patients to re-test every 6 months even if the results are negative. U.S.Food and Drug Administration. Drug Safety Communication: New risk factor for progressive Multifocal Leukoencephalopathy (PML) associated with Tysabri (natalizumab). Accessed on October 14, 2012. http://www.fda.gov/drugs/drugsafety/ucm288186.htm Gilenya (fingolimod) Approved for RRMS after interferon and glatiramer Reduce frequency of exacerbation and delays disability MoA: sphingosine-1- phosphate receptor modulator. Internalizes S1P on lymphocytes, preventing the egress from the LN to the peripheral tissue inhibiting demyelination and neurodegeneration Goodin DS, Frohman EM, Garmany GP, et al. Disease modifying therapies in multiple sclerosis: Subcommittee of the American Academy of Neurology and the MS Council for Clinical Practice Guidelines. Neurology. January 2002; 58(2); 169-178 U.S. Food and Drug Administration. Drug Safety Communication: Revised recommendations for cardiovascular monitoring and use of multiple sclerosis drug Gilenya (fingolimod). Accessed on October 14,2012. http://www.fda.gov/Drugs/DrugSafety/ucm303192.htm Clinical Pearls 0.5 mg PO daily Baseline ECG Caution Bradycardia and AV block; caution with β-blockers and/or Ca channel blockers Infections 72% Decrease pulmonary function test Increase liver transaminase concentration within 3-4 months Most common side effects include: HA, influenza, diarrhea, back pain, elevation of ALT, and cough Novantrone (Mitoxantrone) Second/third line agents approved for RRMS and SPMS patients MoA: Related to anthracyclines; cross links DNA and cause strand breakage. Inhibits RNA & DNA synthesis. Cell cycle non specific 12 mg/m2 IV every 3 months Maximum lifetime dose due to cardiomyopathy, leukemia, leucopenia, and infection (140 mg/m2 ; ~ 11 doses) Barten LJ, Allington DR, Procacci KA, Rivey MP. New approaches in the management of multiple sclerosis. Drug Design, Development and therapy. 2010:4 343-366 Goodin DS, Frohman EM, Garmany GP, et al. Disease modifying therapies in multiple sclerosis: Subcommittee of the American Academy of Neurology and the MS Council for Clinical Practice Guidelines. Neurology. January 2002; 58(2); 169-178 Clinical Pearls Patients should be in hospital setting IV only Irritant, and must be diluted Caution Discontinue when LVEF <50 % or when clinically significant reduction in LVEF is seen Effects of cardiotoxicity may be delayed; it is seen even after completion of therapy Patients undergo annual LVEF evaluation following discontinuation to monitor delayed cardiotoxicity Do not administer when neutrophils < 1500 cells/mm3 Severe bone marrow suppression Increase risk of developing secondary acute myelogenous leukemia (AML) in patients with cancer or MS Marriot JJ, Miyasaki JM, Gronseth G, et al. Evidence Report: The efficacy and safety of mitoxantrone (Novantrone) in the treatment of multiple sclerosis: Report of the therapeutics and Technology Assessment subcommittee of the American Academy of Neurology. Neurology. 2010; 74;1463 Aubagio (Teriflunomide) Significant reduction in active lesions in both RRMS & SPMS patients MoA: inhibits pyrimidine synthesis resulting in antiproliferative and anti-inflammatory effects. It may reduce activated lymphocytes in the CNS Active metabolites of leflunomide, inhibits T-cell activation by blocking interaction with antigen-presenting cells T ½ life 18-19 days; enterohepatic recycling contribute to long T ½ life 7 mg or 14 mg PO daily Daily Med. Aubagio (teriflunomide) tablet, film coated. Accessed on October 16, 2012. http://dailymed.nlm.nih.gov/dailymed/lookup.cfm?setid=4650d12c-b9c8-4525-b07f-a2d773eca155 Clinical pearls Caution Should discontinue when ALT elevation >3x ULN & administer Cholestyramine 8 grams every 8 hours for 11 days or activated charcoal 50 grams every 12 hours for 11 days Contraindicated with severe hepatic impairment Contraindicated in women of childbearing age if non compliant with contraceptive use Pregnancy category X Avoid other immunosuppressant medications Most common side effects include: HA, elevated ALT, hypophosphatemia, hyperkalemia, alopecia, neutropenia, influenza, nausea and vomit. References 1 of 2 Barten LJ, Allington DR, Procacci KA, Rivey MP. New approaches in the management of multiple sclerosis. Drug Design, Development and therapy. 2010:4 343-366 Daily Med. Aubagio (teriflunomide) tablet, film coated. Accessed on October 16, 2012. http://dailymed.nlm.nih.gov/dailymed/lookup.cfm?setid=4650d12c-b9c84525-b07f-a2d773eca155 Goodin DS, Cohen BA, et al. Assessment: The use of natalizumab (Tysabri) for the treatment of multiple sclerosis (an evidence-based review): Report of the therapeutics and technology assessment subcommittee of the American Academy of Neurology. Neurology 2008;71;766 Goodin DS, Frohman EM, Garmany GP, et al. Disease modifying therapies in multiple sclerosis: Subcommittee of the American Academy of Neurology and the MS Council for Clinical Practice Guidelines. Neurology. January 2002; 58(2); 169178 Hove VI, Lemmens K, Van de Velde S, et al. Matrix metalloproteinase-3 in the central nervous system: a look on the bright side. J Neurochem. November 2012; 123(2):203-16 Lexi-Comp, Inc. (Lexi-Drugs TM). Lexi-comp, Inc; October 14, 2012 References 2 of 2 Marriot JJ, Miyasaki JM, Gronseth G, et al. Evidence Report: The efficacy and safety of mitoxantrone (Novantrone) in the treatment of multiple sclerosis: Report of the therapeutics and Technology Assessment subcommittee of the American Academy of Neurology. Neurology. 2010; 74;1463 National Multiple Sclerosis Society. Diagnosing MS. Accessed on October 14, 2012. http://www.nationalmssociety.org/about-multiple-sclerosis/what-we-know-aboutms/diagnosing-ms/index.aspx Ontaneda D, Rae-Grant AD. Management of acute exacerbations in multiple sclerosis. Ann Indian Acad Neurol. Oct 2009; 12(4):264-272 Oliveira SR, Kallaur AP, Simao AN, et al. Oxidative stress in multiple sclerosis patients in clinical remission: Association with the expanded disability status scale. J Neurol Sci. October 15, 2012; 321(1-2):49-53 Rossi B, Angiari S, Zenaro E, et al. Vascular inflammation in central nervous system diseases: adhesion receptors controlling leukocyte-endothelial interactions. J Leukoc Biol. April 2011; 89(4):539-56 U.S.Food and Drug Administration. Drug Safety Communication: New risk factor for progressive Multifocal Leukoencephalopathy (PML) associated with Tysabri (natalizumab). Accessed on October 14, 2012. http://www.fda.gov/drugs/drugsafety/ucm288186.htm U.S. Food and Drug Administration. Drug Safety Communication: Revised recommendations for cardiovascular monitoring and use of multiple sclerosis drug Gilenya (fingolimod). Accessed on October 14,2012. http://www.fda.gov/Drugs/DrugSafety/ucm303192.htm