Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Coronary artery disease wikipedia , lookup
Electrocardiography wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Cardiac surgery wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Myocardial infarction wikipedia , lookup
Jatene procedure wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
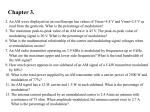
Oxygen Supplementation and Cardiac-Autonomic Modulation in COPD* Matthew N. Bartels, MD, MPH; John M. Gonzalez, BS; Woojin Kim, BS; and Ronald E. De Meersman, PhD Study objectives: Patients with COPD have an increased sympathetic modulation and reduced baroreflex sensitivity (BRS). Therefore, we studied the effects of breathing 31% supplemental oxygen (SuppO2) on autonomic modulation in a group of COPD patients. Design: We measured autonomic modulation before and during the administration of SuppO2 on 51 patients with COPD using time-frequency analysis of R-R intervals and BP before and after intervention. This was done via a counterbalanced crossover design. The BRS index was determined using the sequence method. Results: Significant differences were seen in oxygen saturation levels following breathing with SuppO2 ([mean ⴞ SD] 96.4 ⴞ 1.5%) when compared to those seen after breathing with compressed air (CA) (92.8 ⴞ 2.9%; p < 0.0001). Significant increases were seen in the natural log-transformed high-frequency modulation (HFln) (SuppO2, 10.8 ⴞ 1.3 natural logarithm [ln] ms2/Hz; CA, 10.6 ⴞ 1.3 ln ms2/Hz; p < 0.028) and BRS (SuppO2, 3.3 ⴞ 2.2 ms/mm Hg; CA, 2.8 ⴞ 1.8 ms/mm Hg) following the supplemental oxygen treatment (p < 0.015). The lowfrequency/high-frequency ratio of heart rate variability revealed significant differences between the two treatments (SuppO2, 2.7 ⴞ 1.2; CA, 3.1 ⴞ 1.3; p < 0.008). The analysis of BP variability data revealed significant decreases in the HFln (CA, 6.9 ⴞ 1.0 mm Hg2/Hz; SuppO2, 6.5 ⴞ 1.2 mm Hg2/Hz; p < 0.0001). Hemodynamic data also revealed a decrease in mean heart rate after breathing SuppO2 compared with that after breathing CA (CA, 87.3 ⴞ 13.3 beats/min; SuppO2, 85.0 ⴞ 12.4 beats/min; p < 0.0004). The arterial pulse pressure significantly decreased when breathing SuppO2 compared with that when breathing CA (CA, 57.2 ⴞ 13.5 mm Hg; SuppO2, 53.3 ⴞ 13.0 mm Hg; p < 0.0023). Conclusion: Oxygen supplementation in COPD patients significantly and favorably alters autonomic modulation. (CHEST 2000; 118:691– 696) Key words: autonomic modulation; baroreflex sensitivity; chronic obstructive lung disease; COPD; oxygen supplementation Abbreviations: BRS ⫽ baroreceptor sensitivity; CA ⫽ compressed air; HFln ⫽ log-transformed high-frequency modulation; ln ⫽ natural logarithm; SatO2 ⫽ oxygen saturation; SBP ⫽ systolic BP; SuppO2 ⫽ 31% supplemental oxygen; TF ⫽ time-frequency and hypercapnia have been shown to H ypoxia increase sympathetic nerve activity. Saito et al 1 demonstrated that the degree of hypoxia correlated with the degree of muscle nerve activity. Other *From the Human Performance Laboratory, Presbyterian Hospital of the New-York Presbyterian Hospital, New York, NY; and the Department of Rehabilitation Medicine, College of Physicians and Surgeons of Columbia University, New York, NY. This research was supported in part through the Rehabilitation Medicine Scientist Development Program Fellowship, NIH-1K12-HD01097– 01A1, 1998 –2000. Manuscript received November 16, 1999; revision accepted April 11, 2000. Correspondence to: Matthew N. Bartels, MD, MPH, 180 Fort Washington Ave, Harkness Pavilion, Room 184, Suite 199, New York, NY 10032; e-mail: [email protected] studies have suggested that hypercapnia also leads to increases in muscle sympathetic traffic and that combined hypercapnia and hypoxia synergistically increase sympathetic activity2,3 through impaired baroreceptor-cardiac reflex control.4 Disruption of autonomic reflexes with increased sympathetic modulation, loss of vagal activity, and altered baroreceptor sensitivity (BRS) have been shown to be major risk factors for cardiac morbidity and mortality.5–7 Since patients with COPD experience hypoxia and hypercapnia and since prior preliminary research has demonstrated reduced BRS in COPD patients,8 we studied a group of patients with severe COPD to evaluate their autonomic modulation in response to breathing 31% supplemental oxygen (SuppO2). CHEST / 118 / 3 / SEPTEMBER, 2000 Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21952/ on 05/15/2017 691 Table 1—Patient Characteristics* Characteristics Values (n ⫽ 51) Age, yr Height, cm Weight, kg BMI, kg/m2 63.18 ⫾ 7.92 168.01 ⫾ 9.80 65.79 ⫾ 16.91 23.84 ⫾ 4.14 *Values given as a mean ⫾ SD. BMI ⫽ body mass index. Materials and Methods Subjects Fifty-one patients with COPD were enrolled in the study. See Tables 1 for the subject characteristics and Table 2 for pulmonary profile data. All studies were carried out in the Human Performance Laboratory of the College of Physicians and Surgeons of Columbia University. All procedures were approved by the Human Subject Committee of Columbia University. Following the signing of the consent form, subjects were prepared for the data collection protocol. Subjects were recruited sequentially from the patients referred for exercise testing. All enrolled subjects had received established medical diagnoses of COPD with no other active respiratory disease. All subjects were instructed to maintain their normal daily routine and medications on the day of data collection but to refrain from taking any short-acting bronchodilators on the morning of data collection. Subjects were randomized to the order of the treatments. Design A counterbalanced crossover design after randomization was used. Table 2—Pulmonary Profile Data* Characteristics MVV L/min % Normal FEV1 L % Normal FVC L % Normal DLCO mL/min/mm Hg % Normal MIP CM H2O % Normal MEP CM H2O % Normal MEP Arterial pH Paco2, mm Hg Pao2, mm Hg Values (n ⫽ 51) 30.55 ⫾ 15.26 30.54 ⫾ 14.53 0.73 ⫾ 0.35 28.94 ⫾ 11.68 1.90 ⫾ 0.79 54.55 ⫾ 18.03 6.99 ⫾ 3.45 30.22 ⫾ 12.42 60.76 ⫾ 16.94 82.20 ⫾ 92.70 117.08 ⫾ 35.35 75.00 ⫾ 26.40 7.42 ⫾ 0.03 42.24 ⫾ 8.64 65.14 ⫾ 11.87 *Values given as a mean ⫾ SD. MVV ⫽ maximum voluntary ventilation; FVC ⫽ forced vital capacity; Dlco ⫽ Diffusing capacity of the lung for carbon monoxide; MIP ⫽ maximum inspiratory pressure; MEP ⫽ maximum expiratory pressure; % Normal ⫽ percent of standard predicted for normal values. Statistical Analysis Paired t test comparisons were made between the two treatments for all dependent variables. Due to the number of t tests performed, we subjected all analyses to a Bonferroni correction, and p ⬍ 0.0125 was considered to be significant. Data Acquisition Preparatory Phase: Subjects were seated, at rest, and postabsorptive for at least 4 h and had refrained from consuming alcohol and caffeinated beverages for at least 12 h prior to the test. A multilead ECG was attached to the subject (model Max-1; Marquette Medical Systems; Milwaukee, WI). Respiration was recorded via amplified signals recorded from a thermistor (YSI reusable temperature probe; Yellow Springs, OH) placed under the subject’s nostril. A radial artery pulse sensor for BP was attached to the subject’s wrist to record beat-to-beat BP (model 7000; Colin Medical Instruments; San Antonio, TX). The BP was measured with the BP cuff at heart level on the right arm. Pulse oximetry was recorded using an index finger pulse oximeter (Sat-Trak Pulse Oximeter 767589 –103; SensorMedics; Yorba Linda, CA). The data were gathered while the subject was seated in an upright position. The environment in which they were seated was quiet with dimmed lighting, and subjects equilibrated to the environmental conditions for 15 min prior to the initiation of any data collection. Data Collection: To remove bias, a Venturi mask was placed on the subject and either SuppO2 or compressed air (CA) was delivered to the subject in a random order. There were two data-gathering protocols. Protocol 1 comprised the following: 15 min of equilibration while breathing O2; 5 min of data collection while breathing O2; followed by 15 min of equilibration while breathing CA; and 5 min of data collection while breathing CA. Protocol 2 comprised the following: 15 min of equilibration while breathing CA; 5 min of data collection while breathing CA; followed by 15 min of equilibration while breathing O2; and 5 min of data collection while breathing O2. Randomization to a protocol was based on the patient’s hospital identification number (odd number, protocol 1; even number, protocol 2). The total test duration was approximately 40 min (two trials with 15 min of equilibration on a new gas mixture in between). All data collection epochs were 5 min in duration, which is in accordance with the standards put forth by the Task Force on Standards of Heart Rate Variability Procedures.9 Data gathering sessions included ECG recordings using lead II and lead V5, beat-by-beat BP recordings, oxygen saturation (SatO2) levels, and respiration. During data collection, the subjects were instructed to breathe at a rate of 12 breaths/min for all collection periods. Breathing was regulated through the use of a pacing light that cycled 12 times a minute. All biopotentials were channeled through an interface board (BNC 2080; National Instruments; Austin TX) and were fed into a 12-bit analog-todigital converter (DAQCard-700; National Instruments) and then into a computer (Vision Book Plus; Hitachi; San Jose, CA) with a high-speed processor (Pentium; Intel; San Jose, CA). Postacquisition data analyses were carried out separately. All data were stored on the hard drive of the computer and were backed up daily using cartridges for exterior computer drives (Zip drive, Jaz drive; Iomega; Roy, UT). Data Analysis Time-Frequency Analysis: The current investigation used time and frequency or the Wigner-Ville distribution to decompose heart rate variability. This analysis is preferred over the traditional frequency spectral analysis due to the nonstationary nature 692 Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21952/ on 05/15/2017 Clinical Investigations of respiration in COPD patients. Specifically, the Wigner-Ville distribution decomposes a signal expressed as a function of time into a signal expressed as a function of both time and frequency. In this approach, the signal is divided into a series of short windows, and the Fourier transform then is calculated for each section. The problem with this approach is that as the time window is made shorter the frequency resolution decreases, resulting in a lessened ability to accurately determine the frequency content. In other words, there is a tradeoff between time resolution and frequency resolution. The time-frequency (TF) methods used herein do not suffer from the resolution problems described above and produce a distribution that is accurate in both time and frequency. The TF analysis employed herein, namely, the Wigner-Ville distribution, uses a modified Fourier transform applied to overlapping sections of the time signal to develop a joint density function that is dependent on both time and frequency. It has been shown to provide a reliable estimate of spectral powers without generating undesirable cross-terms. Furthermore, the Wigner-Ville distribution provides the most accurate estimate and the highest resolution.10,11 For a more detailed description on the Wigner-Ville distribution method of analysis, we refer the reader to Novak.12 Due to the skewness of the data, a log transformation was performed. BRS Assessment: The spontaneous beat-by-beat interactions of systolic BP (SBP) and R-R interval reflect true baroreflex events rather than random interactions.13 The R-R intervals were delineated via a peak detection algorithm described in previous work from our laboratory.14 The spontaneous baroreflex response was determined from the beat-to-beat changes in the R-R interval and SBP by a modification of the technique of Bertinieri et al.15 Linear regression was performed on any episode of three consecutive beats with R-R interval lags in the same direction (either up or down), and the resultant data yield an evaluation of the baroreflex sensitivity.13 Verification of the correct breathing frequency of 12 breaths/min was made by visually counting the respiratory trace on the computer display panel as well as by spectrally decomposing the respiratory wave. BP Variability Analysis TF analysis was performed in a similar fashion to the heart rate variability analysis. In this technique, the systolic peaks are detected via a peak detection algorithm and then are interpolated and spectrally decomposed via the Wigner-Ville distribution. Mean Heart Rate Analysis: Using the peak detection algorithm described in the article by Volterrani et al,8 the mean interbeat intervals were calculated for the sample and were averaged to arrive at a mean heart rate. Mean Pulse Pressure Analysis: Using the peak detection algorithm described in the article by De Meersman et al,14 the mean SBP and diastolic BP were calculated as SBP-diastolic BP from an average of the entire sample. Figure 1. Comparison of the HFln of heart rate while breathing SuppO2 and while breathing CA. CA, 2.8 ⫾ 1.8 msec/mm Hg; p ⬍ 0.015) following the SuppO2 treatment. See Figure 1 for HFln data and Figure 2 for BRS data. The low-frequency modulation/HFln ratio of heart rate variability revealed significant differences between the two treatments (SuppO2, 2.7 ⫾ 1.2; CA, 3.1 ⫾ 1.3; p ⬍ 0.008) (Fig 3). The analysis of BP variability data revealed that there was a significant decrease in the logtransformed HFln (CA, 6.9 ⫾ 1.0 modulations/mm Hg2/Hz; SuppO2, 6.5 ⫾ 1.2 ln mm Hg2/Hz; p ⬍ 0.0001) (Fig 4). The log-transformed low-frequency modulation of BP variability did not reveal any significant differences. Hemodynamic data revealed a decrease in mean heart rate while breathing SuppO2 compared to that while breathing CA (CA, 87.3 ⫾ 13.3 beats/min; SuppO2, 85.0 ⫾ 12.4 beats/min; p ⬍ 0.0004) (Fig 5). The arterial pulse pressure significantly decreased during breathing with SuppO2 vs breathing with CA (CA, 57.2 ⫾ 13.5 mm Hg; SuppO2, 53.3 ⫾ 13.0 mm Hg; p ⬍ 0.0023) (Fig 6). Results Significant differences were seen in SatO2 levels following breathing with SuppO2 compared to those following breathing with CA (mean [⫾ SD] SuppO2, 96.4 ⫾ 1.5%; CA, 92.8 ⫾ 2.9%; p ⬍ 0.0001). For the autonomic parameters, significant increases were seen in the natural log-transformed high-frequency modulation (HFln) (SuppO2, 10.8 ⫾ 1.3 natural logarithm [ln] ms2/Hz; CA, 10.6 ⫾ 1.3 ln ms2/Hz; p ⬍ 0.028) and BRS (SuppO2, 3.3 ⫾ 2.2 ms/mm Hg; Figure 2. BRS on a beat-to-beat basis while breathing SuppO2 and while breathing CA. CHEST / 118 / 3 / SEPTEMBER, 2000 Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21952/ on 05/15/2017 693 Figure 3. Comparison of the ratio of natural log-transformed low-frequency modulation (LFln) to HFln of heart rate while breathing SuppO2 and CA. Figure 5. Comparison of the mean heart rate while breathing SuppO2 and CA. Discussion The results of this investigation indicate that oxygen supplementation in COPD patients significantly and favorably alters autonomic modulation. Specifically, following breathing with SuppO2 there is an augmentation in high-frequency cardiac modulation, an increased BRS, a decrease in heart rate, a decrease in high-frequency BP modulation, and a decrease in the mean pulse pressure. The increase in high-frequency cardiac modulation is representative of an increase in vagal tone. The lack of change in low-frequency modulation may be due to the presence of high sympathetic tone and the use of sympathetic agonists in many of these patients. The decrease in high-frequency modulation in BP is also consistent with improved vagal tone and with a possible modulation of the sympathetic tone.16 Highfrequency BP modulation is known to be dependent on a combination of sympathetic and vagal tone, while low-frequency modulation is more purely sympathetic. Since there is little alteration of the lowfrequency component of BP variability, there is also probably little change in the sympathetic component of the high-frequency modulation. This leaves the vagal component of the high-frequency modulation as the most likely cause of the significant change seen in the high-frequency modulation. The decreases in pulse pressure and heart rate support these findings. This autonomic modulation may be due to a combination of factors, including reduced work of breathing, increased chemoreceptor sensitivity, and a reduction in pulmonary artery pressures. Although the change in arterial pulse pressure was small, it is in the range of values found to correlate favorably with improved outcomes in a population of patients with cardiac disease.17,18 The heart rate is improved significantly, and larger heart rate changes have been shown to improve cardiac morbidity.19 However, the significance of this small change is Figure 4. Comparison of the log-transformed HFln of BP while breathing SuppO2 and CA. Figure 6. Comparison of the mean arterial pulse pressure while breathing SuppO2 and CA. 694 Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21952/ on 05/15/2017 Clinical Investigations unclear,20 other than as a marker of increased vagal tone. The BRS is in the range of high-risk patients in a population of patients with cardiac disease. These numbers are in the range of poor outcome expectations as seen in the recent Autonomic Tone and Reflexes After Myocardial Infarction trial.21 The improvement in the BRS is approximately 17%, which is within the range that has been shown to improve outcomes in cardiac patients.22 Although we are concerned with a different population in this study, the ability to induce a change with treatment may imply an improvement as well for individuals with COPD. As hypercapnia and hypoxemia are strong stimulants to sympathetic activity, a higher basal autonomic tone could be expected between the subjects who were frankly hypoxemic (Pao2, ⱕ 60) and/or hypercapnic (Paco2, ⱖ 45) and those subjects who were less affected. The hypoxemic/hypercapnic group also may be expected to have different responses to the treatment with supplemental oxygen. Unfortunately, the number of subjects who fell into the severely affected group was too small to allow for a clear evaluation of these differences. The collection of more subjects in both the hypercapnic and hypoxemic groups should be undertaken to look at these issues. Since the subject’s respiratory rate, inspiratory time, and expiratory time were controlled for in this experiment, we would not expect significant changes in the work of breathing or in arterial CO2 levels after SuppO2 administration. For this reason, we would not expect this to cause stimulation of the chemoreceptors, which would affect autonomic modulation. Pulmonary hypertension has been shown to be, at least in part, responsible for the attenuation of baroreflex responses in COPD patients.4 It is for this reason that we speculate that the normalization of BRS in these individuals is partially due to a reduction in pulmonary arterial tension following breathing with SuppO2. The improved central venous SatO2 level during SuppO2 administration might decrease the level of pulmonary arterial vasoconstriction and right ventricular wall stress, in turn causing a decrease in sympathetic tone. This might happen via the nitric oxide-mediated pathway, which causes a direct relaxation of the pulmonary artery smooth muscle in the presence of increased oxygen tension. Since chronic hypoxemia and its associated pulmonary hypertension have been shown to be major causes of morbidity and mortality,23 these findings of improved autonomic modulation have particular clinical relevance. The long-term oxygen treatment trial and nocturnal oxygen treatment trial demonstrated the long-term benefits of SuppO2 in the reduction of mortality in individuals with severe hypoxemia. Although the mechanisms of the reduction of mortality are not totally clear, these results established supplemental oxygen as the standard of care for these individuals.24,25 While these studies failed to demonstrate a reduction in pulmonary hypertension and cor pulmonale in patients with chronic hypoxemia, there appeared to be a reduction of the progression of pulmonary hypertension. This may have occurred via a reduction of hypoxic vasoconstriction and a reduction in basal vascular tone with the prevention of vascular smooth muscle hypertrophy.26,27 Our findings of increased vagal modulation may be an indication of a possible mechanism to describe the clinical finding mentioned above. In conclusion, this study demonstrates that SuppO2 in COPD patients significantly and favorably alters autonomic modulation. The exact mechanism by which this happens is not clear; however, future research involving measurements of pulmonary arterial pressures, nitric oxide levels, and endtidal CO2 levels might hold the answer. These findings may be of special value in further supporting evidence of a cardioprotective role of SuppO2 in patients with COPD. ACKNOWLEDGMENT: We thank the VIDDA foundation for its continued support. References 1 Saito M, Mano T, Abe H, et al. Responses in muscle sympathetic activity to acute hypoxia in humans. J Appl Physiol 1986; 55:493– 498 2 Somers VK, Mark AL, Abboud FM. Potentiation of sympathetic nerve responses to hypoxia in borderline hypertensive subjects. Hypertension 1988; 11:608 – 612 3 Somers VK, Mark AL, Abboud FM. sympathetic activation by hypoxia and hypercapnia: implications for sleep apnea. Clin Exp Hypertens 1988; A10(suppl):413– 422 4 Bhattachaya J, Cunningham DJC, Howson MG, et al. The effects of mild hypoxia with constant PACO2 and ventilation on the setting and sensitivity of the baroreceptor-cardiacdepressor reflex in man. J Physiol 1973; 234(suppl):112p– 114p 5 Bigger JT Jr, Kleiger RE, Fleiss JL, et al. Components of heart rate variability measured during healing of acute myocardial infarction. Am J Cardiol 1988; 61:208 –215 6 Billman GE, Hoskins RS. Time-series analysis of heart rate variability during submaximal exercise: evidence for reduced cardiac vagal tone in animals susceptible to ventricular fibrillation. Circulation 1989; 80:146 –157 7 Bilmann GE, Schwartz PJ, Stone HL. Baro-receptor reflex control of heart rate: a predictor of sudden cardiac death. Circulation 1982; 66:874 – 880 8 Volterrani M, Scalvini S, Mazzuero G, et al. Decreased heart rate variability in patients with chronic obstructive pulmonary disease. Chest 1994; 106:1432–1437 9 Task Force of the European Society of Cardiology and North American Society of Pacing and Electrophysiology. Heart rate variability: standards of measurement, physiological interpretation, and clinical use. Circulation 1996; 93:1043–1065 CHEST / 118 / 3 / SEPTEMBER, 2000 Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21952/ on 05/15/2017 695 10 Kitney RI. Techniques for studying short-term changes in cardiorespiratory data. In: di Rienzo M, ed. Computer analysis of cardiovascular signals. Washington, DC: IOS Press, 1995; 41–52 11 Novak P. Time/frequency mapping of the heart rate, blood pressure and respiratory signals. Med Biol Eng Comput 1993; 31:103–110 12 Novak V. Slow cardiovascular rhythms at tilt and syncope. J Clin Neurophysiol 1995; 12:64 –71 13 Blaber AP, Yamamoto Y, Hughson RL. Methodology of spontaneous baroreflex relationship assessed by surrogate data analysis. Am J Physiol 1995; 268 (suppl):H1682–H1687 14 De Meersman R, Reisman S, Daum R, et al. Influence of respiration on metabolic, hemodynanic, psychometric, and R-R interval spectra. Am J Physiol 1995; 269(suppl):H1437–H1440 15 Bertinieri G, Dirienzo M, Cavallazzi A, et al. Evaluation of baroreceptor reflex by blood pressure monitoring in unanesthetized cats. Am J Physiol 1988; 254(suppl):H377–H383 16 Murphy CA, Sloan, RP, Myers MM. Pharmacologic responses and spectral analyses of spontaneous fluctuations in heart rate and blood pressure in SHR rats. J Auton Nerv Syst 1991; 36:237–250 17 Smuylan H, Safar ME. Systolic blood pressure revisited. J Am Coll Cardiol 1997; 29:1407–1413 18 Madhavan S, Ooi WL, Cohen H, et al. Relation of pulse pressure and blood pressure reduction to the incidence of myocardial infarction. Hypertension 1994; 23:395– 401 19 SaCunha R, Pannier B, Benetos A, et al. Association between high heart rate and high arterial rigidity in normotensive and hypertensive subjects. J Hypertens 1997; 15(suppl):1423–1430 20 La Rovere MT, Specchia G, Mortara A, et al. Baroreflex sensitivity, clinical correlates, and cardiovascular mortality among patients with a first myocardial infarction: a prospective study. Circulation 1988; 78:816 – 824 21 La Rovere MT, Bigger JT Jr, Marcus FI, et al. Baroreflex sensitivity and heart-rate variability in prediction of total cardiac mortality after myocardial infarction: ATRAMI (Autonomic Tone and Reflexes After Myocardial Infarction) Investigators. Lancet 1998; 351:478 – 484 22 Pagani M, Somers V, Furlan R, et al. Changes in autonomic regulation induced by physical training in mild hypertension. Hypertension 1988; 12:600 – 610 23 Weitzenblum E, Mammosser M, Ehrhart M. Evolution and prognosis of pulmonary hypertension in chronic obstructive pulmonary diseases. Herz 1986; 11:147–154 24 Medical Research Council Working Party. Long term domiciliary oxygen therapy in chronic hypoxic cor pulmonale complicating chronic bronchitis and emphysema. Lancet 1981; 1:681– 685 25 Nocturnal Oxygen Therapy Trial Group. Continuous or nocturnal oxygen therapy in hypoxemic chronic obstructive airways disease: a clinical trial. Ann Intern Med 1980; 93:391– 398 26 Fletcher EC, Luckett RA, Goodnight-White S, et al. A double-blind trial of nocturnal supplemental oxygen for sleep desaturation in patients with chronic obstructive pulomonary disease and a daytime PaO2 above 60 mm Hg. Am Rev Respir Dis 1992; 145:1070 –1076 27 Stewart AG, Howard P. Indications for long term oxygen therapy. Respiration 1992; 59(suppl):8 –13 696 Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21952/ on 05/15/2017 Clinical Investigations