Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
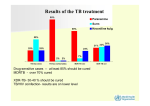
Management of Tuberculosis (TB) and Multidrug-Resistant TB (MDR TB) Monica Avendano, MD, FRCPC Associate Professor of Medicine University of Toronto Medical Director, TB Service West Park Healthcare Centre, Toronto Tuberculosis is a Social Disease with a Medical Aspect. Sir William Osler in 1902 (1849-1919) Worldwide Trends & the Burden of TB Disease TB is still one of the leading causes of death in low-income and middleincome countries. TB remains a threat to public health in industrialized countries. The worldwide burden is still growing. Risk Factors which Perpetuate Worldwide TB Ongoing Exposure to TB Increasing Poverty: -Lack of or poor housing -Poor nutrition -Over crowding -No access or erratic access to healthcare Wars and Natural Disasters Mass Migrations usually from poor resources settings to industrialized settings Tuberculosis in the World Incidence: 9.5 million new cases/year Prevalence: 14 million cases 95% of cases in resource poor settings 1.1 millions co-infection TB/ HIV (12% HIV Positive have TB) 1.7 millions deaths/year 98% deaths in poor resource countries WHO 2010 Tuberculosis in Canada (Demographically and Geographically Focused) 1,600 Cases in 2009 TB Rate - 4.7/100.000 65% of cases in Foreign Born personsRate 14/100.000 21% in First Nation People- Rate 28/100.000 Rate in Nunavut 174/100.000 75% of cases are in large urban centres in Ontario, BC and Quebec Socially marginalized groups Rate in Atlantic Region 1/100.000 Management of TB • Medical Management Diagnosis Treatment Follow-up • Psychosocial Management Stigma Multicultural issues Financial implications Impact on family life Management of TB Diagnosis Suspect TB/Think TB Clinical (presenting symptoms, duration of symptoms, previous TB) Diagnostic Imaging (X-Rays, CT Scans, MRI’s) Bacteriology (smears, cultures) Pathology of biopsy specimens Epidemiological Factors Management of TB Obtain adequate clinical specimen Drug susceptibility in first isolate At least 3 bactericidal drugs Adequate duration of treatment: beyond the time of sputum conversion and amelioration of symptoms Adequate follow-up: prescribing the drugs is just the beginning Attention to psychosocial factors Treatment of TB Goals 1. Sterilize the lesion 2. Avoid development of resistance Clinical Principles 1. Treat with multiple drugs 2. Adequate dosages 3. Sufficient duration 4. Expert monitoring Drug Susceptibility in TB Fully susceptible to all first line drugs Mono-Resistant: resistant to a single first line drug (Most frequently to Isoniazid) Poly-Resistant: resistant to 2 or more first line drugs but not to Isoniazid and Rifampin Multidrug-Resistant (MDR TB): resistant to Isoniazid and Rifampin Extensively Drug-resistant (XDR TB): MDR TB with additional resistance to a quinolone and an injectable Anti-TB Drugs Group 1 - Isoniazid, Rifampin, Pyrazinamide,Ethambutol Group 2 - Amikacin, Kanamycin, Capreomycin Group 3 - F-Quinolones Group 4 - Ethionamide, Cycloserine. PAS,Prothionamide Group 5 - Clofazimine,Imipenem, Thioacetazone, Clavulin, Macrolides, Linezolid Duration of TB Treatment Drugs Duration INH/RMP/PZA + EMB x 2 months INH/RMP x 4 months 6 months INH/RMP + EMB No INH or No RMP 9 months 18 – 24 months Poly-Resistant TB Case Study KL, 44 year old female, born in Congo. Lived in Russia for 3 months looking after sister in a TB ward Arrived in Canada as a refuge claimant 3 years prior to her diagnosis of TB No previous history of TB Gave a 1 year history of right sided chest pain and cough 3 weeks of fever, chills, malaise and weight loss Seen by community physician who diagnosed pneumonia Biaxin x 7 days; Levofloxacin x 7 days Not better Stopped working as a PSW in a seniors home Went to an ER Abnormal CXR: bilateral UL’s cavities Referred to the WPHC’s TB Clinic Poly-resistant TB Case Study Admitted with presumptive diagnosis of TB Induced Sputum: AFB+, AMTD + Treatment with the 4 drugs from Group 1 Culture grew in 4 weeks M. TB resistant to Isoniazid, Ethambutol, Pyrazinamide,Streptomycin, Ofloxacin and Ethionamide POLY- RESISTANT TB Poly-resistant TB Case Study Treatment modified : Rifampin iv, Amikacin iv, Imipenem iv, Clarithromycin, PAS and Clofazimine PAS discontinued due to increased TSH Bacteriologic conversion after 5 months of treatment Treated for 2 years after bacteriologic conversion Completed treatment January 2011 Last seen March 2011. Remains well, CXR and CT Scan show scarring MDR TB • > 450,000 cases identified every year • 150,000 deaths/year from a disease that could and should be curable • MDR TB is MAN MADE -Mismanagement of Fully susceptibleTB or INH resistant TB -Poor quality of drugs -Drugs shortages erratic supply - Patients not taking drugs correctly • XDR TB results from failure to properly manage MDR TB MDR TB Case Study (1) LW,19 year old male, born in China Arrived in Canada as a landed immigrant In China Pulmonary TB treated for 2 years with frequent changes in his medications (Rifampin,Isoniazid, Ethambutol , Ofloxacin and Amikacin) Because of persistent disease Treatment Failure, admitted to hospital (3 months) Left Upper Lobectomy. Came to Canada 2 months after discharge from the Chinese hospital MDR TB Case Study(1) In Canada Attended school in Toronto (grade 9), from November until June the following year Chest X-Ray in March (for surveillance purposes) reported abnormal. Not investigated Presented in July with productive cough, weight loss, night sweats and fatigue of 3 months duration Referred by community physician to the TB Clinic at WPHC. Abnormal Chest Radiography Admitted to WPHC from the clinic with presumptive diagnosis of MDR TB MDR TB Case Study(1) On admission Cachectic, febrile, cough +++ Sputum Smears 4+, AMTD + Initial Treatment : Moxifloxacin iv, Amikacin iv, Clofazimine, Cycloserine and PAS Culture positive in 3 weeks MDR TB with additional resistance to Ethambutol and Rifabutin MDR TB Case Study(1) Slow response to the treatment At West Park for 7 months Regular follow-ups in clinic after discharge Completed 32 months of treatment in January 2011 (24 months after bacteriologic conversion) Follow-up every 3 months for the first year after treatment completion: CXR, bacteriologic update (induced sputum) and Chest CT Scan if CXR shows even minimal changes Last clinic visit April 2011. Remains well. MDR TB CASE STUDY (2) 22 years old man, Tibetan born, lived in India for 10 years, came to Canada January 2008 as a refugee claimant No previous history of TB Smoker, ETHOL drinker, “party boy” September 2009: Malaise, poor appetite, anal pain radiated to left lumbosacral area and left gluteus Unable to walk, febrile, not responding to “Tibetan medicines” November 15, 2009 , went to ER. Admitted to acute care Hospital Diagnosed: Sacral Osteomyelitis Pus aspirated, grew anaerobes and Gram negative organisms. Treated with IV Moxifloxacin and Flagyl MDR TB Case Study (2) In Acute Care: Chest X-Ray abnormal. Sputum AFB +++ CT Scan of Chest Posterior Segment RUL infiltrate Bronchoscopy Smear + December 1st,2009, Started anti-TB Treatment: Oral Rifampin, Ethambutol and Moxifloxacin December 15, 2009: Isoniazid and B6 added Stools with mucus and blood Totally unable to walk and sit down December 21, 2009: MDR TB with additional resistance to Ethambutol, Ethionamide, Streptomycin and Rifabutin December 22, 2009: Transferred to WPHCC MDR TB Case (2) On Admission to WPHC: Febrile, cachectic, large right thigh abscess (sacral abscess drained through the rectum and down through the abdominal muscles sheet) Stools grew TB Initial Phase of Treatment (6 months): IV Amikacin, Moxifloxacin and Imipenem, plus oral Pyrazinamide (x 3 months),Clofazimine,Cycloserine, Linezolid, and B6 Continuation Phase of Treatment: Oral Moxifloxacin, Cycloserine, Clavulin B6, and Clofazimine Bacteriologic conversion May 2010 Resolution of abscesses MDR TB Case (2) Discharged July 30, 2010 after 7 months in hospital Follow up every 3 months for 1 year after discharge December 2010, significant improvement, able to ambulate with a walker, gaining weight Last seen in Clinic April 11, 2011 - Weight gain 23 ½ kilos -Able to walk without a gait aid -Chest x-ray clear Plan is to continue treatment until May 2012 MDR TB Management Treatment should be individualized and based on drug susceptibility studies Patient to receive all the drugs to which the infecting M.TB is susceptible. When available drugs need to be given iv If there is past history of TB and drugs previously received are known, give at least 3 drugs (bactericidal) never used before If drug susceptibility still unknown give at least 3 bactericidal drugs, but no Rifampin or Isoniazid Treatment for 2 years following bacteriologic conversion DOT mandatory Well structured and strict follow-up Surgery in selected cases Management of MDR TB Prolonged Hospitalization Significant psycho-social issues Requires increased number of drugs Poor tolerance to the drugs Increased drug- associated toxicity Long term Follow-Up is necessary Increased health care costs MDR TB in Ontario Affects mainly foreign born individuals in Canada for less than 5 years Significant number of patients have previous history of TB People from countries with high burden of TB and Drug Resistant TB will continue to migrate to Canada MDR TB Control Extraordinary measures are needed in countries with the highest rates of TB and MDR TB: rapid detection, access to drugs and steady drugs supply and effective and expert care. The only reasonable approach is strengthening TB Control worldwide to prevent MDR TB and XDR TB Tuberculosis anywhere is Tuberculosis everywhere