Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
West Nile fever wikipedia , lookup
Hepatitis C wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Onchocerciasis wikipedia , lookup
Neglected tropical diseases wikipedia , lookup
Chagas disease wikipedia , lookup
Gastroenteritis wikipedia , lookup
Hepatitis B wikipedia , lookup
Sexually transmitted infection wikipedia , lookup
Marburg virus disease wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Oesophagostomum wikipedia , lookup
Neonatal infection wikipedia , lookup
Carbapenem-resistant enterobacteriaceae wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Schistosomiasis wikipedia , lookup
Meningococcal disease wikipedia , lookup
Leptospirosis wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
Lymphocytic choriomeningitis wikipedia , lookup
Neisseria meningitidis wikipedia , lookup
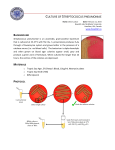
Streptococcus pneumoniae Chapter 23 Streptococcus pneumoniae S. pneumoniae was isolated independently by Pasteur and Steinberg more than 100 years ago. – Also called “pneumococcus” Pneumococcal disease is still a leading cause of morbidity and mortality. PHYSIOLOGY AND STRUCTURE Gram + coccus 0.5 to 1.2 μm in diameter, oval or lancet shaped, and arranged in pairs and short chains (Figure 23-9). Older cells decolorize readily and appear gram-negative. PHYSIOLOGY AND STRUCTURE S. pneumoniae has fastidious nutritional requirements and can grow only on enriched media supplemented with blood products. α-hemolytic on blood agar if incubated aerobically and may be β-hemolytic if grown anaerobically. – The α-hemolytic appearance results from production of an enzyme that degrades hemoglobin, pneumolysin, which produces a green product. Figure 23-9 Gram stain of Streptococcus pneumoniae. PHYSIOLOGY AND STRUCTURE S. pneumoniae, like all streptococci, lacks catalase. S. pneumoniae grows poorly in media with high glucose concentrations. – Fermentation → lactic acid rapidly reaches toxic levels in such preparations. PHYSIOLOGY AND STRUCTURE Virulent strains of S. pneumoniae are covered with a complex polysaccharide capsule. It is these polysaccharides that are used for the serologic classification of strains; currently, 90 serotypes are recognized. Purified capsular polysaccharides from the most commonly isolated serotypes are used in the pneumococcal vaccine. Pathogenesis Not very well understood Primary damage and disease come from our immune response and not toxins, etc. Virulence factors – Table 23-6 Epidemiology 5-75% of people are colonized Most infections are caused by endogenous spread from the colonized nasopharynx or oropharynx to distal site (e.g., lungs, sinuses, ears, blood, meninges) Person-to-person spread through infectious droplets is rare Typically a secondary infection (after the flu, etc.) Young children and the elderly are at greatest risk for meningitis Although the organism is ubiquitous, disease is more common in cool months Figure 23-10 - The incidence of carriage & associated disease is highest during the cool months. Epidemiology Most infections are caused by endogenous spread from the colonized nasopharynx or oropharynx to distal site (e.g., lungs, sinuses, ears, blood, meninges) Person-to-person spread through infectious droplets is rare Individuals with antecedent viral respiratory tract disease or other conditions that interfere with bacterial clearance from respiratory tract are at increased risk for pulmonary disease Young children and the elderly are at greatest risk for meningitis Although the organism is ubiquitous, disease is more common in cool months CLINICAL DISEASES - Pneumonia 500,000 cases per year Acute onset, consisting of a severe shaking chill and sustained fever Symptoms of a viral respiratory tract infection 1 to 3 days prior. Cough with blood-tinged sputum Chest pain (pleurisy). Lobar pneumonia Rapid recovery following the initiation of appropriate antimicrobial therapy, with complete resolution in 2 to 3 weeks. CLINICAL DISEASES - Sinusitis and Otitis Media Over 7 million cases per year Acute infections of the paranasal sinuses and middle ear. Usually preceded by a viral infection of the upper respiratory tract, – polymorphonuclear leukocytes (PMN) infiltrate and obstruct the sinuses and ear canal. Middle ear infection (otitis media) is primarily seen in young children, but bacterial sinusitis can occur in patients of all ages. Figure from other text CLINICAL DISEASES - Meningitis 6000 cases per year Infection of the central nervous system following – – – bacteremia infections of the ear or sinuses head trauma that causes a communication between the subarachnoid space and the nasopharynx. Bacterial meningitis can occur in patients of all ages but is primarily a pediatric disease. Mortality and severe neurologic deficits are 4 to 20 times more common in patients with meningitis caused by S. pneumoniae than in those with meningitis resulting from other organisms. CLINICAL DISEASES - Bacteremia 55,000 cases per year Occurs in 25% to 30% of patients with pneumococcal pneumonia and in more than 80% of patients with meningitis. In contrast, bacteria are generally not present in the blood of patients with sinusitis or otitis media. Endocarditis can occur in patients with normal or previously damaged heart valves. Treatment, Prevention, and Control Penicillin is the drug of choice for susceptible strains – In cases of allergy to penicillin or penicillin-resistnats other drugs are used; – – – – Antibiotic resistance is increasingly common Cephalosporins Erythromycin Chloramphenicol Vancomycin Immunization is recommended for all children younger than 2 years of age and for adults at risk for disease