Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Coronary artery disease wikipedia , lookup
Myocardial infarction wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Jatene procedure wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Atrial septal defect wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
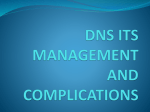
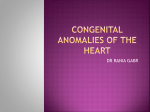
Am J Physiol Heart Circ Physiol 280: H2639–H2648, 2001. Compression of interventricular septum during right ventricular pressure loading GREGORY S. NELSON,1 EZZELDIN Y. SAYED-AHMED,2 CAROL A. GIBBONS KROEKER,1 YI-HUI SUN,1 HENK E. D. J. TER KEURS,1 NIGEL G. SHRIVE,1 AND JOHN V. TYBERG1 1 Departments of Medicine, Physiology and Biophysics and Civil Engineering, University of Calgary, Calgary, Alberta T2N 4N1, Canada; and the 2Department of Civil Engineering, Ain Shams University, Cairo 11331, Egypt Received 19 July 2000; accepted in final form 24 January 2001 (17) suggested in 1914 that displacement of the septum during diastole might explain how the filling of one ventricle influenced the performance of the other. The development of echocardiography led to renewed interest in septal mechanics, as Popp et al. (33) observed, in patients with right ventricular (RV) volume overload (RVVO), that the septum moved leftward during diastole, findings supported later by others (4, 11, 14, 23, 37). Observations consistent with those described during RVVO also occurred during RV pressure overload (RVPO). Stool et al. (40) constricted pulmonary arteries in dogs and observed a gradual increase in RV end-diastolic pressure and a decrease in left ventricular (LV) septum-to-free wall diameter, inferred to be the result of a leftward shift of the septum. Other studies (3, 30) later reported similar findings. To define the determinants of septal position and motion better, Kingma et al. developed an open-chest canine model and investigated the effects of both RVVO and RVPO on the position and motion of the septum, as determined by sonomicrometry and twodimensional (2-D) echocardiography (24). Both RVVO and RVPO progressively increased end-diastolic RV septum-to-free wall diameter and complementarily decreased the respective LV diameter, in agreement with previous studies (3, 4, 14, 30, 37, 40, 43). Furthermore, they showed that the end-diastolic septal position (as reflected by the septum-to-free wall diameters) was precisely proportional to transseptal pressure (TSP ⫽ LVP-RVP). Normally, end-diastolic TSP is ⬃3 mmHg positive and the septum is concave to the LV. However, RVVO and RVPO reduced or reversed end-diastolic TSP and shifted the septum leftward, flattening and sometimes inverting it. Visner et al. (47) and Feneley et al. (15) confirmed those results in their studies of conscious dogs as well as Thompson et al.’s (45) study of human patients. These studies seemed to suggest that the septum behaved like a passive compliant membrane (e.g., a sail) between two liquid-filled chambers in that its diastolic position could be predicted by TSP. Dong et al. (13) related septal short-axis radius of curvature (R; 2-D echo) and midwall septal segment length (SSL; sonomicrometry) to LVP, RVP, and ventricular septum-to-free wall diameter (2-D echo) during pulmonary artery (PA) and aortic constrictions in anesthetized dogs. Over a wide range of TSP (0 ⫾ 7 mmHg), they demonstrated that changes in ventricular diameters, as measured by Kingma et al. (24), were proportional to changes in SSL, which were also linear functions of TSP. Thus echo-measured changes in Address for reprint requests and other correspondence: J. V. Tyberg, Depts. of Medicine and Physiology and Biophysics, Health Sciences Centre, 3330 Hospital Dr. NW, Calgary, Alberta T2N 4N1 Canada (E-mail: [email protected]). The costs of publication of this article were defrayed in part by the payment of page charges. The article must therefore be hereby marked ‘‘advertisement’’ in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. finite element analysis; interventricular septum; mechanics; compressive stress HENDERSON AND PRINCE http://www.ajpheart.org 0363-6135/01 $5.00 Copyright © 2001 the American Physiological Society H2639 Downloaded from http://ajpheart.physiology.org/ by 10.220.33.6 on May 13, 2017 Nelson, Gregory S., Ezzeldin Y. Sayed-Ahmed, Carol A. Gibbons Kroeker, Yi-Hui Sun, Henk E. D. J. Ter Keurs, Nigel G. Shrive, and John V. Tyberg. Compression of interventricular septum during right ventricular pressure loading. Am J Physiol Heart Circ Physiol 280: H2639–H2648, 2001.—The interventricular septum, which flattens and inverts in conditions such as pulmonary hypertension, is considered by many to be an unstressed membrane, in that its position is assumed to be determined solely by the transseptal pressure gradient. A two-dimensional finite element model was developed to investigate whether compression and bending moments (behavior incompatible with a membrane) exist in the septum during diastole under abnormal loading, i.e., pulmonary artery (PA) constriction. Hemodynamic and echocardiographic data were obtained in six open-chest anesthetized dogs. For both control and PA constriction, the measured left ventricular and right ventricular pressures were applied to a residually stressed mesh. Adjustments were made to the stiffness and end-bending moments until the deformed and loaded residually stressed mesh matched the observed configuration of the septum. During PA constriction, end-bending moments were required to obtain satisfactory matches but not during control. Furthermore, substantial circumferential compressive stresses developed during PA constriction. Such stresses might impede septal blood flow and provoke the unexplained ischemia observed in some conditions characterized by abnormal septal motion. H2640 SEPTAL COMPRESSION DURING RV LOADING METHODS Experimental Preparation Six mongrel dogs of either sex were anesthetized, initially with thiopental sodium (25 mg/kg iv), and subsequently with an infusion of fentanyl citrate (25 mg 䡠 kg⫺1 䡠 h⫺1), intubated, and ventilated (70% NO2-30% O2 mixture) with the use of a constant-volume respirator (model 607, Harvard Apparatus; Millis, MA). A large bore cannula was introduced into the external jugular vein for administration of fluids. A midline sternotomy was performed, and the ventrolateral surface of the pericardium was incised transversely (⬃5-cm long) along the base of the heart and retracted for instrumentation. To manipulate TSP and achieve septal flattening and inversion, an inflatable silicone occluder (In Vivo Metric; Healdsburg, CA) was placed around the main PA. The heart was then repositioned into the pericardium, and the pericardial margins were reapproximated with several sutures. Care was taken to avoid decreasing the pericardial volume (39). LV and RV pressures were measured with 8-Fr micromanometer-tipped catheters with reference lumina (model SPC-485, Millar Instruments; Houston, TX) inserted through a carotid artery and internal jugular vein, respectively. A liquid-filled catheter was inserted into the aorta via a femoral artery to monitor pressure. The liquid-filled catheters were attached to transducers (model P23ID, Statham Gould; Oxnard, CA) and referenced to the level of the right atrium. Before the data were collected, pressures measured by the micromanometers were matched to those measured from the liquid-filled catheters to correct for baseline drift. After the animals underwent surgical preparation, they were allowed to stabilize for 30 min. Body temperature was maintained throughout the experiment with the use of a heating pad, and an electrocardiogram (lead II) was recorded to monitor cardiac rhythm and rate. All of the conditioned hemodynamic signals were amplified (model VR16, Electronics for Medicine/Honeywell; White Plains, NY), passed through a lowpass filter (100 Hz), and digitized at 200 Hz. Echocardiographic Frame Acquisition The interventricular septum was imaged (30 frames/s) echocardiographically (model V3400, Diasonics; Salt Lake City, UT) in an LV minor-axis view by using a 5.0-MHz transesophageal probe held on the surface of the RV free wall. We were careful to maintain consistency during recording of the ultrasound images. Referencing to the level of the tips of the papillary muscles (these served as “internal landmarks”) helped ensure that the same short-axis slice was imaged in each of the six dogs. Furthermore, to account for the effect of ventricular torsion during the cardiac cycle, the imaging probe was rotated slightly, so that the same degree of anterior and posterior septal insertion points was viewed in each recording run. A video frame synchronizer (Odessa Computer Systems; Calgary, Canada) was used to match the echocardiographic frames (recorded on 1⁄2-in. videotape) to be analyzed with the corresponding hemodynamic data. Experimental Protocol Hemodynamic and echocardiographic data were obtained simultaneously and continuously for 30 s (including a 10-s control period) with the respirator turned off. Attempts were made to obtain complete flattening or inversion of the septum in each PA constriction run. Between interventions, an in- Downloaded from http://ajpheart.physiology.org/ by 10.220.33.6 on May 13, 2017 ventricular diameters reflect changes in the length of the septum. Second, by plotting curvature (1/R) versus TSP, they confirmed that the septum becomes flat only when TSP approximates ⫺5 mmHg, consistent with the results of other studies (1, 25). Beyar et al. (6) demonstrated the importance of the fact that the septum is a thick-walled structure, specifically that bending moments are important. Only when their model accounted for bending moments did it duplicate two critical features of the experimental results: 1) that the septum is not flat at TSP ⫽ 0 mmHg, and 2) that midwall SSL continues to become shorter after septal inversion, whereas end-diastolic TSP becomes progressively negative. Although those authors had expected reextension of SSL at greater negative values of TSP, the observed result was consistent with the midwall SSL because it was subjected to compressive stress. If SSL had been measured near the LV endocardium, it would have relengthened, consistent with the extension stress borne by the LV endocardial fibers during inversion. Thus, in contrast to the implication of the previous echocardiographic studies (24, 25, 43, 45), in which the septum behaved like a passive compliant membrane, the septum seemed to behave more like a thick-walled structure subject to lateral pressure and end-bending moments. That stress patterns are highly dependent on local ventricular wall curvature was suggested by Gould et al. (16). Later, Heethaar et al. (20) used a finite element (FE) model to study the stress gradients in both single LV and in combined RV-LV models. The myocardium was assumed to be isotropic, homogeneous, and linearly elastic. During diastole, the LV had the largest stresses at the endocardial surface and, in the combined RV-LV model, there was a large stress concentration at the septum-RV junction. Compressive stresses were also found in the septum. Pao et al. (32), also by using the FE approach, modeled a cross section of an isolated LV in diastole (reconstructed from roentgenographic recordings) and assumed that the myocardium was homogeneous, isotropic, and linearly elastic. Endocardium-to-epicardium circumferential stress gradients occurred only in the anterior and posterior walls. In the septum and LV free wall, the gradient was reversed but of smaller magnitude. Furthermore, the model showed that some circumferential compressive stresses developed near the LV septal surface, where the wall curvatures were small and convex inward. As described above, the motion pattern of the interventricular septum during pathophysiological (abnormal) loading conditions is complex. No study has thoroughly investigated this unique structure under such severe conditions from a structural mechanics viewpoint. Accordingly, the goal of our study was to further elucidate the structural behavior patterns of the septum under both normal and abnormal loading. Specifically, we developed a two-dimensional (2-D) FE model of the interventricular septum to test the hypothesis that secondary to PA constriction, compressive stress and bending moments do develop in the septum. H2641 SEPTAL COMPRESSION DURING RV LOADING terval of 10–15 min was allowed to elapse for hemodynamic stabilization. Hemodynamic and Echocardiographic Data Analysis Hemodynamic data were subsequently analyzed with the use of commercial software (CVSOFT, Odessa Computer Systems). With the use of image-analysis software developed in our laboratory (CVIMAGE5, Odessa Computer Systems), septal midwall points were identified on the 2-D echocardiograms. A midwall line was constructed by connecting these points and by smoothing (2). From this line, we made radiusof-curvature measurements. Finally, thickness (normal to the midwall line) was measured. FE Model and Analysis Fig. 1. A: finite element (FE) mesh used to model the interventricular septum composed of 120 plane-stress elements arranged in 6 layers of 20 elements. Truss elements (thick line) were used at both ends of the mesh (left side, posterior insertion point; right side, anterior insertion point) to allow for application of end-bending moments. These truss elements were made sufficiently stiff so that rigid-body rotation about the midnodes at the ends of the mesh could be achieved. B: two different constitutive relationships were investigated: neo-Hookean (linear stress-strain) and sarcomere forcelength (nonlinear stress-strain) relationship (10), implemented via an Arruda-Boyce energy function. Bending Moment ⫽ 冉 冊 RV ⫺ LV T 2 2 6 Downloaded from http://ajpheart.physiology.org/ by 10.220.33.6 on May 13, 2017 Model. A 2-D FE model of the interventricular septum was developed, with the use of the FE program Abaqus (version 5.6, Hibbitt, Karlsson and Sorenson; Pawtucket, RI), to investigate the difference in structural behavior between control and PA constriction-loading conditions. The model will be described only briefly here because a more detailed description has been published (29). FE mesh constitutive relations. The FE mesh consisted of 120-plane stress elements arranged in 6 layers of 20 elements (Fig. 1A). Truss elements were used at both ends of the mesh to allow for application of end-bending moments. These truss elements were made sufficiently stiff so that rigid-body rotation about the midnodes at the ends of the mesh could be achieved. Two different constitutive relationships (Fig. 1B) were investigated: 1) neo-Hookean (linear stress-strain) and 2) a sarcomere force-length (nonlinear stress-strain) relationship (10), implemented via an Arruda-Boyce energy function. Both models were made hyperelastic to account in part for any large strains associated with the PA constriction cycle. Large deformation was also accounted for by invoking geometric nonlinearity into the analysis. In so-called linear geometric problems, equilibrium equations may be written with respect to the original undeformed configuration because the deformations are minimal (i.e., the configuration remains essentially unchanged) (8). However, when the deformations become large, as occurs during abnormal loading (i.e., PA constriction), equilibrium equations must be written with respect to the deformed geometry. Residual stress. Earlier investigators (31) have ignored the residually stressed (RS) state of completely relaxed in situ ventricular myocardium. We accounted for residual stress in each dog by applying bending moments at the ends of the initial unstressed mesh such that the resulting stress distribution closely matched that calculated by Guccione et al. (18). The parameters of the calculated RS state were saved to an input file and incorporated into each loading step in the form of an initial stress condition. Accounting for sarcomere length changes during diastole. To analyze images other than those at end diastole, the geometry of the RS mesh was adjusted according to values of sarcomere length (SL) idealized from the measurements of Rodriguez et al. (35) and Guccione et al. (19). In the cardiac cycle, SL increases during diastole. Hence, the geometry of the mesh had to be adjusted to account for diastolic SL changes. On the basis of these studies (19), it was estimated that SL increased 17% from its end-systolic value to its end-diastolic value (15% linearly to the point of minimum LV pressure when the LV fills rapidly and, perhaps, actively, and a further 2% linearly to the point of minimum LV pressure when the LV fills less rapidly and passively. Thus, for each frame analyzed, the radius-of-curvature of the enddiastolic RS mesh was reduced accordingly. Furthermore, because we assumed the septum maintains constant crosssectional area in the plane of the model, each radius-ofcurvature reduction coincided with a proportional increase in thickness. Loading conditions. Measured LV and RV pressures were applied to the RS mesh and then end-bending moments were adjusted until conformity to the observed configuration of the septum was judged to be satisfactory. For both the neoHookean (linear) and nonlinear models, adjustments in material stiffness were also required for satisfactory matches to be obtained. Computational requirements: linear versus nonlinear model. The approximate time required to reach convergence for the neo-Hookean (linear) model was 15 min, whereas for the sarcomere force-length (nonlinear) model, 2 h were required with the use of an Origin 2000 computer (Silicon Graphics; Mountain View, CA). Because the results obtained from both models were so similar (see Stress Plots and Bending-Moment Diagrams), we accepted results with the use of the neo-Hookean relationship for the multiple analyses for each of the six dogs analyzed. Bending-moment diagrams. Bending-moment diagrams were constructed by calculating the bending moment per unit thickness along the length of the septum by using the expression H2642 SEPTAL COMPRESSION DURING RV LOADING where RV is the circumferential stress at the RV septal surface, LV is the circumferential stress at the LV septal surface, and T is the thickness. Statistical Analysis Hemodynamic and geometric data (presented as means ⫾ SE unless stated otherwise) were plotted with the use of SigmaPlot 4.0 for Windows (Jandel Scientific; San Rafael, CA) as a function of time to illustrate the temporal trends of these parameters during control and PA constriction observations. All statistical testing was performed with the use of SigmaStat 2.0 for Windows statistical software (Jandel) on a Pentium IBM-compatible computer. RESULTS TSP and Septal Geometry Fig. 2. Diastolic transseptal pressure gradient (TSP ⫽ LVP ⫺ RVP) plotted as a function of time from end systole (ES) to end diastole (ED) (pooled data from all 6 dogs). Compared with control data, TSP during pulmonary artery (PA) constriction was substantially lower (and negative) throughout diastole. In particular, TSP was reduced near 0 mmHg at ES, dropped to a maximum negative value (approximately ⫺10 mmHg) shortly thereafter, approached a minimum negative value near mid-diastasis, and then tended to become slightly more negative toward ED. Fig. 3. Curvature (1/R) of the midportion of the septum plotted against time. During the control period (pooled data from all 6 dogs), the curvature of the septum decreased from ES to ED. During PA constriction (data from each dog plotted individually), the curvature of the septum was reduced (i.e., the septum was flattened) compared with the control data. Inversion was observed in only 3 of the 6 dogs. In those dogs, inversion was first observed midway through diastole (i.e., near mid-diastasis). control data. Although TSP was lowered to a similar degree during PA constriction in all dogs, inversion was observed in only three dogs. In those dogs, inversion was first observed midway through diastole (i.e., near mid-diastasis). Shear Modulus and End-Bending Moments Once the measured loading was applied (LVP and RVP) and changes in SL were accounted for (via changes in mesh geometry), adjustments in shear modulus (G) (material stiffness for neo-Hookean formulation) and end-bending moments were required to make the RS mesh conform satisfactorily to the observed shape of the septum. In Fig. 4, G is plotted as a function of time for both control and PA constriction Fig. 4. Neo-Hookean shear modulus, G, plotted as a function of time for both control and PA constriction cycles during diastole. For both conditions, G decreased rapidly after ES, reached a minimum value midway through diastole and then tended to increase slightly toward ED. Downloaded from http://ajpheart.physiology.org/ by 10.220.33.6 on May 13, 2017 The diastolic (end systole to end diastole) transseptal pressure gradient (TSP ⫽ LVP-RVP) is plotted in Fig. 2 (pooled data from all six dogs). Compared with control data, TSP during PA constriction was substantially lower (and negative) throughout diastole. In particular, TSP was reduced near 0 mmHg at end systole, dropped to a maximum negative value (approximately ⫺10 mmHg) shortly after, approached a minimum negative value near middiastasis, and then tended to become slightly more negative toward end diastole. Curvature (1/R) of the midportion of the septum is plotted against time in Fig. 3. During the control period (pooled data from all six dogs), the curvature of the septum decreased from end systole to end diastole. During PA constriction (data from each dog plotted individually), the curvature of the septum was reduced (i.e., the septum was flattened) compared with the SEPTAL COMPRESSION DURING RV LOADING H2643 cycles during diastole. In both loading conditions, G decreased rapidly after end systole, reached a minimum value midway through diastole and then tended to increase slightly toward end diastole. End-bending moments are plotted as a function of time in Fig. 5. Only the PA constriction data are presented, because no end-bending moments were required to make the control data RS meshes conform. For all six dogs, greater end-bending moments (at both insertion points) were required near end systole, compared with those required for the rest of diastole. Larger end-bending moments were required at the anterior insertion point (i.e., right side of the mesh, see Fig. 1A) than at the posterior insertion point (i.e., left side of the mesh). To illustrate the difference in septal structural behavior between control and PA constriction loading, representative principal-stress vector plots and corresponding bending-moment diagrams at mid-diastasis are presented in Fig. 6. To minimize end effects, the two columns of elements on either side of each mesh are not shown. All of the arrows are equally scaled, the magnitude being represented by the size of the paired arrowheads and the distance between them. Whether the stress is tensile or compressive is represented by the direction of the arrowheads, where divergent means tensile and convergent means compressive. Both during control (see Fig. 6A; linear model) and PA constriction observations (see Fig. 6, B and C; linear and nonlinear model, respectively), the radial compressive stresses that developed at the LV and RV surfaces were equal to the applied LV and RV pressures (this was true for all dogs, in each loading condition, and at every point in diastole). The circumferential stresses, which developed in the control state, were small in magnitude (they were similar to the Fig. 6. To illustrate the difference in septal structural behavior between control and PA-constriction loading, representative principal-stress vector plots (A, B, and C, top) and corresponding bendingmoment diagrams (A, B, and C, bottom) at middiastasis are presented. To minimize end effects, the 2 columns of elements on either side of each mesh are not shown. All arrows are equally scaled, the magnitude being represented by the size of the paired arrowheads and the distance between them. Whether the stress is tensile or compressive is represented by the direction of the arrowheads, divergent meaning tensile, convergent meaning compressive. See text for further details. Fig. 5. End-bending moments plotted as a function of time. Only the PA constriction data are presented, because no end-bending moments were required to make the control-data RS meshes conform. For all 6 dogs, greater end-bending moments (at both insertion points) were required near ES, compared with those required for the rest of diastole. Larger end-bending moments were required at the anterior insertion point than at the posterior insertion point. residual stresses) relative to PA constriction, where much larger circumferential compressive stresses clearly developed. These compressive stresses became less circumferentially oriented in more lateral elements. In these elements, the compressive stresses appeared to be aligned towards the “supports” of the mesh (i.e., the midnodes of each end boundary). Note how the stress distributions for the linear and nonlinear PA constriction models (see Fig. 6, B and C) are practically identical. Downloaded from http://ajpheart.physiology.org/ by 10.220.33.6 on May 13, 2017 Stress Plots and Bending-Moment Diagrams H2644 SEPTAL COMPRESSION DURING RV LOADING DISCUSSION Compared with the stresses that developed during the control cycle, the substantial circumferential compressive stresses, which developed in the PA constriction-loading conditions (Fig. 6), suggests an archlike behavior of the septum under these severe conditions. Recall that the arch is a structural system in which the primary internal force is axial compression (7). Like an arch, the septum bears the PA constriction loading by distributing the net “downward” thrust of the load laterally, through a pattern of compressive stress towards its “supports,” which, although not shown, seem to be the RV insertions. Pao et al. (32) and Heethaar et al. (20) have suggested compression in the septum. However, the archlike distribution of stresses shown here, with specifically, maximum compression occurring at the RV septal surface, is a novel finding. Furthermore, we have found with the model that this behavior is sustained during diastole in all dogs analyzed, whereas many previous investigators have limited their analyses to end diastole only. A degree of circumferential tension developed on, and slightly below, the LV septal surface during PA constriction when flattening and/or inversion was observed. This observation is consistent with that made in a previous study from our laboratory, in which Fig. 7. To represent the stress and strain data quantitatively, circumferential stress (A) and corresponding strain (B) values at middiastasis (pooled data from all 6 dogs) are plotted. Values were obtained by averaging the principal stresses and strains at the centroid of each of the 2 midlayer elements for all 6 layers across the wall. During control, the circumferential stresses that developed were roughly equivalent to the residual stress distribution (thick line). Corresponding strains, which developed during control, were small (i.e., all ⬍5%). For PA constriction, markedly different stress and strain patterns were observed. Circumferential stress distribution, which developed was much larger and oppositely oriented, relative to control. septal segment length (SSL) was measured with the use of sonomicrometry crystals that were positioned circumferentially, approximately halfway between the RV and LV septal surfaces (12). It was a surprise to find that SSL did not lengthen, even with extreme degrees of septal inversion. It had been assumed that the septum behaved like a thin-walled membrane and it therefore was reasoned that large negative values of TSP would relengthen the segment, but this was never observed. However, as was speculated at the time, because the crystals had not been placed very close to the LV septal surface, lengthening perhaps should not have been expected. Downloaded from http://ajpheart.physiology.org/ by 10.220.33.6 on May 13, 2017 The bending-moment diagram for the control example revealed only slightly positive values for nearly every element along the mesh (see Fig. 6A). In contrast, significantly different bending-moment distributions were observed for both PA constriction examples (Fig. 6, B and C). Bending moments at the ends of the meshes were positive and much larger than during control observations, they crossed zero near elementpositions 5 and 14, and the most-negative bending moment was achieved near the midpoint of the mesh. The linear and nonlinear PA constriction models showed practically identical bending-moment diagrams as the stress results did. Finally, to represent the stress and strain data quantitatively for the linear model, transseptal circumferential stress and corresponding strain plots at middiastasis are shown in Fig. 7 (pooled data from all six dogs). The values were obtained by averaging the principal stress at the centroid of each of the two midlayer elements for all six layers across the wall. During control, the circumferential stresses that developed were roughly equivalent to the residual stress distribution (they were virtually superimposable), both showing an approximately ⫺3 to ⫹3 mmHg stress variation, from LV to RV septal surfaces, respectively. The corresponding strains that developed during control were small (i.e., all ⬍5%). For PA constriction, markedly different stress and strain patterns were observed. The circumferential stress distribution that developed was much larger and oppositely oriented relative to control, showing an LV to RV septal surface range of ⫹10 to ⫺28 mmHg and corresponding strains of ⫹9 to ⫺17%. SEPTAL COMPRESSION DURING RV LOADING ture rather than the predominant circumferential stress. For the control example, the circumferential stress gradient from the LV septal surface to the RV septal surface was compressive to tensile. Therefore, the bending moment was calculated as positive. Consequently, the bending moment calculated for both inverted septum examples varied from positive to negative to positive because the circumferential stress gradient reversed at two locations. For element positions 3 and 4, the bending moment was positive (consistent with all end-bending moments at the posterior insertion point, see Fig. 5) because the stress gradient across the septum was compressive-to-tensile. From element positions 5-14, the bending moment was negative because the stress gradient reversed, becoming tensile-to-compressive. Finally, for element positions 15–18, the bending moment became positive again (consistent with all end-bending moments at the anterior insertion point, Fig. 5) because the stress gradient again became compressive-to-tensile. These results make sense from a structural mechanics viewpoint. If one considers a beam with fixed ends, subject to uniformly distributed loading (Fig. 8A) the deformation and corresponding bending moment diagram (Fig. 8B) are similar to those obtained by the model. Specifically, flattening or inversion is greatest near the middle of the septum, the zero-moment points coincide with the points of inflection, and the maximum (absolute) bending moment is achieved at the ends (i.e., at the RV insertions). This analogy suggests that the model is predicting the structural behavior correctly, but perhaps more importantly, also confirms the necessity and importance of including bending effects in the model. We speculate that the substantial circumferential compressive stresses predicted by the model during PA constriction may pertain to a number of clinical situations. In several diseases, in which the TSP is decreased or reversed (e.g., mitral stenosis, primary pulmonary hypertension, and pulmonary thromboembolic disease), and septal flattening and inversion is observed, there may be chest pain that is indistinguish- Fig. 8. A: beam with fixed ends is subject to uniformly distributed loading. B: deformation and corresponding bending-moment diagram are similar to those obtained by the model (see Fig. 6). See text for further details. Downloaded from http://ajpheart.physiology.org/ by 10.220.33.6 on May 13, 2017 PA constriction increased RV diastolic pressure and, as venous return to the LV was reduced, tended to decrease LV diastolic pressure. The resultant changes in TSP progressively flattened the septum and, in some cases, produced a modest septal inversion in that it became measurably concave with respect to the LV. These rather subtle changes in the shape of the septum should not be misconstrued when similar magnitudes and temporal trends of TSP during PA constriction (see Fig. 2) appear to have produced strikingly different changes in curvature (1/R) (see Fig. 3). For both the linear and nonlinear models, there was a requirement that material stiffness be slightly greater during PA constriction than for the corresponding control. It is unlikely that this difference in material stiffness resulted from changes in endosarcomeric (e.g., titin) or extracellular matrix (e.g., collagen) proteins because the PA was constricted for ⬍30 s. It is more likely that material stiffness increased owing to an increase in coronary venous pressure. In isolated, perfused dog hearts, Watanabe et al. (48) raised coronary venous pressure by increasing RA/RV pressure, and showed LV end-diastolic pressure (LVEDP; an indicator of LV stiffness) increased significantly at the same LV volume. They also showed that coronary venous pressure was more effective in raising LVEDP than coronary arterial pressure in the range tested. They suggested that this apparent increase in stiffness was related to an increase in intramyocardial blood volume (26), as opposed to either increased pressure or flow. Similarly, Resar et al. (34) have shown that transverse stiffness increased at least twofold as a result of an increase in coronary arterial perfusion pressure from 20 to 80 mmHg. Therefore, coronary venous congestion after PA constriction may explain the increase in material stiffness predicted by our model. The requirement for substantial end-bending moments during PA constriction (they were not required during control) near end systole (Fig. 5) relative to the rest of diastole is consistent with the septum being much stiffer during this part of the cycle. Like the pattern of time-varying elastance derived from a pressure-volume loop (42), G for both control and PA constriction decreased from end systole to a near-stable value for the remainder of diastole (Fig. 4). Furthermore, the requirement for greater end-bending moments at the anterior insertion point (compared to the posterior insertion point) reflects asymmetric flattening and inversion of the septum. Specifically, the curvature of the septum was greatest near the anterior insertion point, and thus greater end-bending moments were required in order for conformity to be obtained in this region of the septum. Whether this asymmetry is due to anatomic differences in the two insertion points or because of some artificially imposed boundary (e.g., the dog was in the supine position during echocardiographic recording) has yet to be determined. The bending-moment diagrams shown in Fig. 6 illustrate that bending moment depends on the circumferential stress gradient, which develops across the struc- H2645 H2646 SEPTAL COMPRESSION DURING RV LOADING able from that associated with myocardial ischemia. This has usually been attributed to RV ischemia, despite the absence of coronary arterial stenoses. In addition, in the presence of left bundle branch block, which also alters septal motion, thallium perfusion studies are often “falsely positive,” suggesting relative septal ischemia even though the coronary arteries are shown to be normal (5). The demonstration of substantial circumferential compressive stresses (equal to about ⫺20 mmHg) in the septum leads to a hypothesis that must be tested rigorously: such stresses could increase resistance to diastolic blood flow to a degree sufficient to cause ischemia. Perfusion studies utilizing either Doppler Flowire or contrast echocardiography techniques will be required to test this hypothesis. The desire to develop a model sufficiently complex to detect structural differences in the septum between control and PA constriction-loading conditions and yet be practical resulted in the use of a 2-D FE model with plane stress elements. Perhaps the most significant limitation of such a model is that fibers, which render the myocardium anisotropic, cannot be incorporated. To attempt to account for the effect of myocardial fibers, one could vary the stiffness in different directions across the mesh, i.e., incorporation of a parabolic variation in circumferential elastic modulus (41). Varying the stiffness, however, would require more material parameters than for the isotropic neo-Hookean hyperelasticity used here, making the problem more difficult to solve numerically. Another significant limitation pertains to the constitutive relation employed in our model. Many attempts have been made to describe an appropriate constitutive relation for the passive myocardium (21). As a first approximation to the material properties of the septum, however, a neo-Hookean (i.e., linear stress-strain) strain-energy function was used. Over the normal working range of rat (38) and cat (9) trabeculae, SL varies between 1.55 and 2.40 m. Rodriguez et al. (35) and Guccione et al. (19) have shown that SL varies between 1.70 and 2.40 m in the intact, normal canine LV. Slack length of the sarcomere (SL0) has been shown to be ⬃1.85 m (44). Between SL of 1.60 m (15% negative strain) and 2.20 m (20% positive strain), the sarcomere force-length relationship is practically linear, i.e., the stiffness is nearly constant (38). The stiffness increases steeply ⬍1.60 m and ⬎2.20 m. Thus the material properties of the septum have been approximated with the use of a neo-Hookean strain-energy function over this range. Furthermore, Rodriguez et al. (35) and Guccione et al. (19) showed that SL ⫽ 2.20 m occurred at an LVEDP of ⬃15 mmHg. Because LVEDP never exceeded 12 mmHg under our control loading conditions, it is assumed that SL did not exceed 2.20 m. During PA constriction, the maximum circumferential compressive strain achieved at mid-diastasis was ⬎⫺15% (Fig. 7). The maximum circumferential tensile strain achieved was ⬃10%. We acknowledge Junyi Yi, Gerald Groves, and Cheryl Meek for excellent technical assistance, and Linda Malley for echocardiographic recording. This study was supported Medical Research Council of Canada (Ottawa) Operating Grant MT-12886 (to J. V. Tyberg and N. G. Shrive) and an accompanying Studentship Award (to G. S. Nelson). REFERENCES 1. Agata Y, Hiraishi S, Misawa H, Takanashi S, and Yashiro K. Two-dimensional echocardiographic determinants of interventricular septal configuration in right and left ventricular overload. Am Heart J 110: 819–825, 1985. 2. Akima H. A method of bivariate interpolation and smooth surface fitting based on local procedures. Comms ACM 17: 18–31, 1974. 3. Badke FR. Left ventricular dimensions and function during right ventricular pressure overload. Am J Physiol Heart Circ Physiol 242: H611–H618, 1982. Downloaded from http://ajpheart.physiology.org/ by 10.220.33.6 on May 13, 2017 Study Limitations Most of the strain values calculated for PA constriction, therefore, fall within the relatively linear region of the force-length relation. Indeed, the similarity between the results from the neo-Hookean and forcelength relation models is because both positive and negative strains were consistently ⬍20%, and therefore the steep part of the force-length relation had no impact on the analysis. It therefore seems reasonable to assume that the neo-Hookean material relation employed in the model holds both for analysis of the control condition and for PA constriction. However, in this context, it is important to recall that the objective of this work was not to determine stress magnitudes precisely but rather to understand and elucidate the structural principles under which the septum operates. In anesthetized open-chest dog preparations, it is well known that hearts typically operate at smaller volumes than normal (22, 36) and the effects of gravity are undoubtedly different from those when the chest is intact. Thus it is possible that the septum was loaded a little differently to a closed-chest preparation, but it is highly unlikely that this would have altered the dramatic change observed in the stress pattern. Although not commonly adopted in analyses of the heart, principal stresses have been used to describe the mechanics of other biological structures, such as bone (46), ligament (28), and cartilage (27). It is recognized that the principal stresses indicated by the model cannot be satisfactorily interpreted without accounting for fiber orientation, but in general, remain an excellent mechanism for showing how load is transferred through the structure. In conclusion, geometric parameters (radius-of-curvature and thickness) of the interventricular septum were derived from a septal midwall line. Local myocardial deformation gradients, as determined by Rodriguez et al. (35) and Guccione et al. (19), cannot be obtained with the use of echocardiography. This limitation of echocardiography is particularly relevant in the PA constriction-loading condition, where the model suggests substantial circumferential compression, and where steep transmural deformation gradients seem to occur. Measurement of SSL with the use of sonomicrometry (13) might allow better determination of such gradients. SEPTAL COMPRESSION DURING RV LOADING 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. 45. JL. Septal geometry in the unloaded living human heart. Circulation 74: 463–468, 1986. Lindner JR, Skyba DM, Goodman NC, Jayaweera AR, and Kaul S. Changes in myocardial blood volume with graded coronary stenosis. Am J Physiol Heart Circ Physiol 272: H567–H575, 1997. MacConaill MA. The movement of bones and joints-4. The mechanical structure of articulating cartilage. J Bone Joint Surg Br 33: 251–257, 1951. Matyas JR, Anton MG, Shrive NG, and Frank CB. Stress governs tissue phenotype at the femoral insertion of the rabbit MCL. J Biomech 28: 147–157, 1995. Nelson GS, Sayed-Ahmed EY, ter Keurs HEDJ, Tyberg JV, and Shrive NG. A 2D finite element model of the interventricular septum under normal and abnormal loading. Comp Meth Biomech Biomed Eng. In press. Olsen CO, Tyson GS, Maier GW, Spratt JA, Davis JW, and Rankin JS. Dynamic ventricular interaction in the conscious dog. Circ Res 52: 85–104, 1983. Omens JH and Fung YC. Residual strain in rat left ventricle. Circ Res 66: 37–45, 1990. Pao YC, Robb RA, and Ritman EL. Plane-strain finite-element analysis of reconstructed diastolic left ventricular cross section. Ann Biomed Eng 4: 232–249, 1976. Popp RL, Wolfe SB, Hirata T, and Feigenbaum H. Estimation of right and left ventricular size by ultrasound: a study of the echoes from the interventricular septum. Am J Cardiol 24: 523–530, 1969. Resar JR, Judd RM, Halperin HR, Chacko VP, Weiss RG, and Yin FCP. Direct evidence that coronary perfusion affects diastolic myocardial mechanical properties in canine heart. Cardiovasc Res 27: 403–410, 1993. Rodriguez EK, Hunter WC, Royce MJ, Leppo MK, Douglas AS, and Weisman HF. A method to reconstruct myocardial sarcomere lengths and orientations at transmural sites in beating canine hearts. Am J Physiol Heart Circ Physiol 263: H293– H306, 1992. Rushmer RF. Shrinkage of the heart in anesthetized, thoracotomized dogs. Circ Res 2: 22–27, 1954. Santamore WP, Lynch PR, Meyer G, Heckman J, and Bove AA. Myocardial interaction between the ventricles. J Appl Physiol 41: 362–368, 1976. Schouten VJ, Bucx JJ, de Tombe PP, and ter Keurs HE. Sarcolemma, sarcoplasmic reticulum, and sarcomeres as limiting factors in force production in rat heart. Circ Res 67: 913–922, 1990. Scott-Douglas NW, Traboulsi M, Smith ER, and Tyberg JV. Experimental instrumentation and left ventricular pressure-strain relationship. Am J Physiol Heart Circ Physiol 261: H1693–H1697, 1991. Stool EW, Mullins CB, Leshin SJ, and Mitchell JH. Dimensional changes of the left ventricle during acute pulmonary arterial hypertension in dogs. Am J Cardiol 33: 868–875, 1974. Streeter DD, Spotnitz HM, Patel DJ, Ross J Jr, and Sonnenblick EH. Fiber orientation in the canine left ventricle during diastole systole. Circ Res 24: 339–347, 1969. Suga H and Sagawa K. Instantaneous pressure-volume relationships and their ratio in the excised, supported canine left ventricle. Circ Res 35: 117–126, 1974. Tanaka H, Tei C, Nakao S, Tahara M, Sakurai S, Kashima T, and Kanehisa T. Diastolic bulging of the interventricular septum toward the left ventricle. An echocardiographic manifestation of negative interventricular pressure gradient between left and right ventricles during diastole. Circulation 62: 558– 563, 1980. ter Keurs HEDJ, Rijnsburger WH, van Heuningen R, and NMJ. Tension development and sarcomere length in rat cardiac trabeculae. Evidence of length-dependent activation. Circ Res 46: 703–714, 1980. Thompson CR, Kingma I, MacDonald RPR, Belenkie I, Tyberg JV, and Smith ER. Transseptal pressure gradient and distolic ventricular septal motion in patients with mitral stenosis. Circulation 76: 974–980, 1987. Downloaded from http://ajpheart.physiology.org/ by 10.220.33.6 on May 13, 2017 4. Bemis CE, Serur JR, Borkenhagen D, Sonnenblick EH, and Urschel CW. Influence of right ventricular filling pressure on left ventricular pressure and dimension. Circ Res 34: 498– 504, 1974. 5. Beppu S, Matsuda H, Shishido T, and Miyatake K. Functional myocardial perfusion abnormality induced by left ventricular asynchronous contraction: experimental study using myocardial contrast echocardiography. J Am Coll Cardiol 29: 1632– 1638, 1997. 6. Beyar R, Dong SJ, Smith ER, Belenkie I, and Tyberg JV. Ventricular interaction and septal deformation: A model compared with experimental data. Am J Physiol Heart Circ Physiol 265: H2044–H2056, 1993. 7. Chajes A. Structural Analysis. Englewood Cliffs, NJ: Prentice Hall, 1990, p. 1–468. 8. Cook RD. Concepts and Applications of Finite Element Analysis. New York: Wiley, 1974, p. 271–271. 9. De Tombe PP and ter Keurs HEDJ. Sarcomere dynamics in cat cardiac trabeculae. Circ Res 68: 588–596, 1991. 10. De Tombe PP and ter Keurs HEDJ. An internal viscous element limits unloaded velocity of sarcomere shortening in rat myocardium. J Physiol (Lond) 454: 619–642, 1992. 11. Diamond MA, Dillon JC, Haine CL, Chang S, and Feigenbaum H. Echocardiographic features of atrial septal defect. Circulation 43: 129–129, 1971. 12. Dong SJ, Beyar R, Zhou ZN, Fick GH, Smith ER, and Tyberg JV. Determinants of midwall circumferential segmental length of the canine ventricular septum at end diastole. Am J Physiol Heart Circ Physiol 265: H2057–H2065, 1993. 13. Dong SJ, Smith ER, and Tyberg JV. Changes in the radius of curvature of the ventricular septum at end diastole during pulmonary arterial and aortic constrictions in the dog. Circulation 86: 1280–1290, 1992. 14. Elzinga G, Van Grondelle R, Westerhof N, and VandenBos GC. Ventricular interference. Am J Physiol 226: 941–947, 1974. 15. Feneley MP, Olsen CO, Glower DD, and Rankin JS. Effect of acutely increased right ventricular afterload on work output from the left ventricle in conscious dogs: systolic ventricular interaction. Circ Res 65: 135–145, 1989. 16. Gould P, Ghista D, and Brombolich L. In vivo stresses in the human left ventricular wall: analysis accounting for the irregular 3-dimensional geometry and comparison with idealised geometry analyses. J Biomech 5: 521–539, 1972. 17. Grossman W and McLaurin LP. Diastolic properties of the left ventricle. Ann Intern Med 84: 316–326, 1976. 18. Guccione JM, McCulloch AD, and Waldman LK. Passive material properties of intact ventricular myocardium determined from a cylindrical model. J Biomech Eng 113: 42–55, 1991. 19. Guccione JM, O’Dell WG, McCulloch AD, and Hunter WC. Anterior and posterior left ventricular sarcomere lengths behave similarly during ejection. Am J Physiol Heart Circ Physiol 272: H469–H477, 1997. 20. Heethaar RM, Robb RA, Pao YC, and Ritman EL. Threedimensional stress and strain in the intact heart. In: Proceedings of the San Diego Biomedical Symposium, edited by Martin JI. New York: Academic, 1976, p. 337–342. 21. Horowitz A, Sheinman I, and Lanir Y. Non-linear incompressible finite element for simulating loading of cardiac tissue. II. Three-dimensional formulation for thick ventricular wall segments. J Biomech Eng 110: 62–68, 1988. 22. Ingels NB Jr, Daughters GT, Nikolic SD, DeAnda A, Moon MR, Bolger AF, Komeda M, Derby GC, Yellin EL, and Miller DC. Left ventricular diastolic suction with zero left atrial pressure in open-chest dogs. Am J Physiol Heart Circ Physiol 270: H1217–H1224, 1996. 23. Kerber RE, Dippel WF, and Abboud FM. Abnormal motion of the interventricular septum in right ventricular volume overload. Circulation 48: 86–96, 1973. 24. Kingma I, Tyberg JV, and Smith ER. Effects of diastolic transseptal pressure gradient on ventricular septal position and motion. Circulation 68: 1304–1314, 1983. 25. Lima JAC, Guzman PA, Yin FCP, Brawley RK, Humphrey L, Traill TA, Lima SD, Marino P, Weisfeldt ML, and Weiss H2647 H2648 SEPTAL COMPRESSION DURING RV LOADING 46. Toridis TG. Stress analysis of the femur. J Biomech 2: 163–174, 1969. 47. Visner MS, Arentzen CE, O’Conner MJ, Larson EV, and Anderson RW. Alterations in left ventricular three-dimensional dynamic geometry and systolic function during acute right ventricular hypertension in the conscious dog. Circulation 67: 353–365, 1983. 48. Watanabe J, Levine MJ, Bellotto F, Johnson RG, and Grossman W. Effects of coronary venous pressure on left ventricular diastolic distensibility. Circ Res 67: 923–932, 1990. Downloaded from http://ajpheart.physiology.org/ by 10.220.33.6 on May 13, 2017