Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
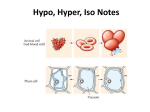
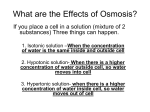
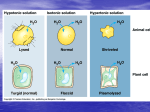
INTRAVENOUS Fluids Presented By Muhammad Suleman Raza INTRODUCTION The goal of intravenous fluid administration is to carefully achieve and maintain a euvolemic and isotonic environment within the body as well as to provide for a variety of nutritional and pharmacologic interventions. The selections of an appropriate IV solution is dependent upon the fluid volume and electrolyte status of the individual patient. Na concentration in Body fluids Body Fluid Concentration serum 135-145 mEq/L Saliva 10-55mEq/L Gastric juice 10-100mEq/L Pancreatic juice 120-140mEq/L Bile 120-160mEq/L Intestinal 105-145mEq/L Stool/diarrhea 1-100mEq/L Skin 1-80mEq/L Na distribution in Body Compartment or Tissue Na Distribution Plasma 11% Interstitial 29% Connective Tissues 12% Bone Exchangeable Non-Exchangeable 14% 29% Intracellular 2.5% Transcellular 2.5% Total 100% Water distribution in body Cont…. General Recommendations For IV Fluid Selection Hyponatremia with Hypovolemia Decreased total body water and Na ,Relatively greater decrease in Na External losses GI : vomiting ,Diarrhea, fistulas ,ostomies Third-space loses : Pancreatitis, peritonitis ,small-bowel obstructions , Rhabdomyolysis , Burns , Post operative period. Renal loses: Diuretics. Osmotic diuresis. Mineralocorticoid deficiency. Salt- losing Naphropathies. Cont… Hypernatremia with Hypovolemia Decreased TBW and Na ; relatively greater decrease in TBW. External losses. GI: vomiting ,Diarrhea. Skin : Burns , excessive sweating. Renal losses. Diuretics medications. Osmotic Diuresis. Cont… Hypernatremia with Euvolemia Relatively decreased TBW ; increased Total body Na. Inability to access free water. Patients on tube feeding. Can’t reach water glass. NPO on isotonic IV fluids only. Cont…. Hypernatremia with hypervolemia Increased TBW; greater increase in Na. Hypertonic IV fluid administration without free water. Total parental nutrition with inadequate free water. Mineralocorticoid excess. Type of IV solution Type of IV solution Isotonic Hypotonic Hypertonic Isotonic solution A solution that has the same salt concentration as the normal cells of the body and the blood. Ex: 1- 0.9% NaCl . 2- Ringer Lactate . 4- D5W. Hypotonic solution A solution with a lower salts concentration than in normal cells of the body and the blood. EX: 1-0.45% NaCl . 2- 0.33% NaCl . Hypertonic solution: • A solution with a higher salts concentration than in normal cells of the body and the blood. Ex: • D5W in normal Saline solution . • D10W. Categories of intravenous solutions according to their purpose: • Nutrient solutions. • Electrolyte solutions. • Volume expanders. Nutrient solutions. • It contain some form of carbohydrate and water. • Water is supplied for fluid requirements and carbohydrate for calories and energy. • They are useful in preventing dehydration and ketosis but do not provide sufficient calories to promote wound healing, weight gain, or normal growth of children. • Common nutrient solutions are D5W and dextrose in half-strength saline. Electrolyte solutions (Crystalloid) • • fluids that consist of water and dissolved crystals, such as salts and sugar. Used as maintenance fluids to correct body fluids and electrolyte deficit . • Commonly used solutions are: -Normal saline (0.9% sodium chloride solution). -Ringer’s solutions (which contain sodium, chloride, potassium, and calcium. -Lactated Ringer’s solutions (which contain sodium, chloride, potassium ,calcium and lactate) . Volume expanders (Colloid) Are used to increase the blood volume following severe loss of blood (haemorrhage) or loss of plasma ( severe burns). Expanders present in dextran, plasma, and albumin. Parenteral Nutrition (PN) Parenteral nutrition is a form of nutritional support that supplies protein, carbohydrate, fat, electrolytes , vitamins, minerals, and fluids via the IV route to meet the metabolic functioning of the body. IV Infusion Method I.V. Bolus (I.V. push) IV Infusion Method Intermittent infusion Continuousdrip infusion Electrolyte content of IV solutions per Liter Fluid Na K Glucose Tonicity Mosm/liter 0.9 NS* 154 0 0 Slightly Hypertonic 304 0.45 NS* 77 0 0 Hypotonic 154 0.25 NS* 38 0 0 Hypotonic 77 Lactated Ringers (LR) 130 4 0 Isotonic 280 D5W 0 0 50gm Hypotonic 0** D5W 0.45 NS* 77 0 50gm Hypotonic 154** 0.9 NS+150 mEq NaHCO3 308 0 0 Very Hypertonic 616 Hypertonic Solutions Content (mEq/L) Clinical Implication Dextrose 5% in 0.45% NS* 77 Na ,77 Cl Daily maintenance of body fluid and nutrition. Dextrose 5% in 0.9% NS* 154 Na , 154 Cl Fluid replacement of Na ,Cl and calories (170) Dextrose 10% in 0.9% NS* 154 Na , 154 Cl Fluid replacement of Na ,Cl and calories (340) Dextrose 5% in Lactated Ringer 130 Na,4 K,109 Cl, 28 lactate, 3Ca2+ Resembles the normal composition of Blood, serum and plasma K+ level below bodies daily requirement caloric value (180) General Recommendations For IV Fluid Selection Achieving Euvolemia Determine the pt. volume status estimate if any ,the degree of variation from euvolemia If euvolemic ,only maintenance fluids need to be prescribed, as in pt. who may be NPO. The dehydrated pt. will require an estimated amount of isotonic fluid to bring them to normal volume status Volume replacement because of additional clinical volume loss like NG suction, diarrhea, Blood loss Measure I/O VOLUME BODY WEIGHT AND Na content of specific fluid loss Achieving Isotonicity Tonicity of body fluids can be measured directly (serum osmolality) , or estimated approximately from the serum sodium concentration ([Na]x2 +10) or more exactly from the formula [Na]x2+glucose/18 The isotonic pt. requires only maintenance Na replacement unless they are also dehydrated The hypertonic (Hypernatremic) pt. requires additional free water replacement . Average TBW=0.66 X body weight. Water Deficit=TBW x[serum Na – 140]/140 Conclusions Achievement and maintenance of a euvolemic and isotonic internal environment requires careful adjustment of water and Na intake that reflects the excesses or deficits of these physiologically linked nutrients. Optimal care of fluid status of an individual also requires an appreciation of the limits of Na and water handling which can vary from pt. to pt depending upon such factors as Age, Renal and Cardiac function and variations in their otherwise routine intake of Na. Standard assessment method include physical examination, serum Electrolytes, and accurate body weight and fluid intake and output measurements. References Androgue HJ,Madias NE. Hyponatremia ,NEJM,2000;342(21):1581-1589 Simpson FO. Sodium intake, body sodium and sodium excretion.Lancet,1988;7(2):25. http://www.medterms.com/script/main/art.asp?articlekey=3870 -Carol.T.taylor and carol lillis.R, (2001): Fundamentals of Nursing, 4th ed ,Lippincott, company,Pheladelphia ,pp:180-249.