Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Heart failure wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Aortic stenosis wikipedia , lookup
Pericardial heart valves wikipedia , lookup
Artificial heart valve wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Atrial septal defect wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
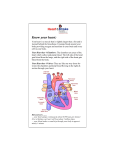
Ebstein’s Malformation Seoul National University Hospital Department of Thoracic & Cardiovascular Surgery Ebstein’s Malformation 1. Definition Congenital defect of tricuspid valve in which the origins of the septal or posterior leaflet or both, are displaced downward into the right ventricle, & the leaflets are variably deformed. Characteristically, the anterior leaflet is enlarged and sail-like. 2. History Ebstein : Description in 1866 MacCallum : 1st description in English literature in 1900 Van Lingen, Soloff : Diagnosis during life in 1951 Lev : WPW syndrome in 1955 Gasul, Scott : Glenn operation in 1959 Barnard, Schrire : Prosthetic valve replace in 1962 Hardy : 1st successful valvuloplasty in 1964 Ebstein’s Malformation Pathophysiology • Downward displacement of the posterior and septal leaflets of the tricuspid valve and atrialization of the right ventricle leads to diminished right ventricular output and congestive heart failure, stemming from tricuspid insufficiency and/or right ventricular dysfunction. • High right atrial pressures from tricuspid insufficiency and high pulmonary vascular resistance during early postnatal period result in right-to-left shunting across an interatrial communication leading to varying degrees of cyanosis. • An increased incidence of accessory conduction pathways leads to paroxysmal supraventricular arrhythmias. Ebstein’s Malformation Ebstein’s Malformation TV Septal leaflet Anatomic Types of Ebstein’s Anomaly 1. Small, contractile, atrialized chamber with a mobile anterior leaflet 2. Large, noncontractile, atrialized chamber with a mobile anterior leaflet 3. Restricted motion of the anterior leaflet 4. “Tricuspid sac” Leaflet tissue forms a continuous sac adherent to the dilated right ventricle. Types of Ebstein’s Anomaly Ebstein’s Malformation Surgical Morphology 1. Tricuspid valve 2. Right ventricle 3. Right atrium 4. Left ventricle 5. The lung 6. Associated defects ; ASD, Pulmoanry atresia or stenosis, VSD, TOF, PDA, TGA, CoA, Congenital MS Clinical Features & Diagnosis 1. Mechanism . . . . Right ventricular dysplasia & dysfunction Tricuspid valve incompetence Pulmonary hypoplasia Wolff-Parkinson-White syndrome 2. Symptoms & signs . . . . 3. 4. 5. 6. Breathlessness, cyanosis, cardiomegaly during the 1st week of life Cyanosis (1/2) : onset in infancy and early childhood Palpitation, malar flush (mitral facies) in 1/3 Wide splitting of the 1st heart sound Chest radiography : rounded or boxlike EKG : RAH, low amplitude R-wave, WPW (5%) Echocardiography Cardiac catheterization & cineangiography Radiographic Findings • Cardiomegaly, Atrialized RV, TR Pathologic Features Three primary pathologic features predominate in patients with Ebstein anomaly • RV abnormalities • Tricuspid valve abnormalities • Accessory conduction pathways • Pulmonary hypoplasia • Their severity & extent determine secondary pathophysiologic features, clinical presentation, and natural history. Also extent and severity of these relate to age at presentation Natural History 1. Incidence . Less than 1% of CHD( 0.2~0.5%), equal in both sex, rarely familial reported 2. Presentation during the 1st week of life . Stillborn, cyanosis, CHF . 20~40% die in newborn 3. Presentation in infancy . Less risk of death or severe symptoms 4. Presentation in childhood & adult life . Mild symptoms & prognosis is good 5. Modes of death . CHF(1/2) . Sudden death(arrhythmia related WPW in 60%) . Others (cerebral abscess, emboli) Operative Techniques 1. Repair of the TV and ASD closure 2. Placement of tricuspid valve About 20~30% 3. Simple ASD closure Rarely indicated 4. Technique for neonate in extremis Starnes Operation (TV closure, ASD creation, systemic-pulmonary shunt) 5. One and a half ventricle repair Operative Technique (Danielson Method) Operative Technique Single-stitch Technique Repair by Carpentier Method Operative Technique Carpentier Method Tricuspid Valve Replacement Surgical Results 1. Survival Early ; acute cardiac failure Late ; sudden death, rhythm disturbances, chronic cardiac failure 2. 3. 4. 5. Functional status Tricuspid valve function after repair Postoperative rhythm disturbances Results of other procedures 1) 2) 3) 4) Starnes operation Repair of ASD alone Tricuspid valvotomy Pulmonary valvotomy Ebstein’s Malformation Advantages of ventricular unloading 1. Alteration in the tricuspid valve function by a combination of geometric changes in the right ventricle and valve apparatus 2. Improve Lt. ventricular function by minimizing the deleterious effects of right to left ventricular interaction Thrombosis in Tricuspid Valves Possible reasons of high incidence • Peak velocity of rapid filling flow is low. • Pressure half time or deceleration time is prolonged. • Velocity is liable to variation under the influence of respiration. • Difference of prostacyclin (PGI2) level in arterial & venous blood (Lungs produce high amount.) Operative Indications 1. Neonates presenting in extremis * Starnes procedure after stabilization 2. Valve repair & closure of ASD * Patients with important TR, moderate cyanosis, or symptoms of CHF and cardiomegaly 3. Simple repair of ASD * Lt. to Rt. shunt with or without symptoms of CHF, and no or little tricuspid valve incompetence 4. Ablation of accessory conduction pathway * Division or ablation of accessory conduction with concomitant repair Special Situations & Controversies 1. Morphology 2. Tricuspid valve replacement . Bioprosthesis . Homograft . Mechanical prosthesis 3. Indications for plication of atrialized ventricle in TVR . Controversial in all cases . When the atrialized portion of RV is very thin & aneurysmal (10~20%) & when TV is repaired 4. Excision or plication of right atrial wall