Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
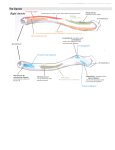
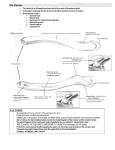
Structure and molecular composition of the coracoclavicular ligaments +1,2Ockert, B; 2Braunstein, V; 1Shinohara, Y; 1Sprecher, C; 1Kirchhoff, C; 1Richards, R G; 1,3Milz, S +1AO Research Institute Davos (ARI), AO Foundation, Davos, Switzerland 2 Department of Trauma and Orthopaedic Surgery – Campus Innenstadt, Ludwig-Maximilians Universitaet, Munich, Germany 3 Anatomische Anstalt, Ludwig-Maximilians Universitaet, Munich, Germany [email protected] BACKGROUND: The coracoclavicular ligament (CCL) complex is formed by the conoid and the trapezoid ligaments connecting the coracoid process and the clavicle. The CCL is considered as the prime restraint support of the acromioclavicular (AC) joint against superior and posterior translation of the distal clavicle with respect to the scapula. Direct or indirect trauma to the shoulder girdle can lead to dislocation of the AC-joint with concomitant rupture of the CCL in grade III to VI injuries according to Rockwood Classification. Numerous surgical procedures restoring ACjoint separation rely on the assumption of intrinsic and extrinsic CCL healing under temporary fixation. Despite its clinical relevance, little is known about the structure and molecular composition of CCL. PURPOSE: The objective was to evaluate the structure and composition of the extracellular matrix of both, the conoid and trapezoid ligament, to investigate for its molecular properties and vascular constitution. STUDY DESIGN: Descriptive laboratory study. METHODS: Tissue preparation: Twelve fresh-frozen coracoclavicular ligament complexes of 8 donors (4 female, and 4 male, age: 48.6 ± 12.1) were removed within 48h of death. Removal was performed by permission of the medical faculty’s ethical board of Munich University. The ligament complexes included the bony entheses at the clavicle and the coracoid process as well as the ligament mid substance of both, the conoid and the trapezoid ligament. Samples were fixed for at least 6 hours in 90% methanol at 4ºC, before being stored at -20ºC in 100% methanol for at least 1 week. Decalcification was done in 12.5 % EDTA after the specimens were trimmed to minimize the bone tissue. Due to the large size of some specimens, the ligament was cut into two halves in five cases before being analysed. Finally all specimens were cryosectioned longitudinally at a thickness of 12µm and mounted on glass slides. No history of AC-joint dislocation or CCL injury was available. Immunohistochemistry: For general histological examination and orientation purpose a few sections from every specimen were stained with toluidine blue. Then the immunohistochemical labelling was done with a panel of monoclonal antibodies including antibodies against type I and II collagen, proteoglycans (versican and aggrecan), link protein, basement membrane (Laminin), and endothelial cell marker (CD 31). Non-specific binding of the antibodies was blocked with horse serum, and control sections were obtained by omitting the primary antibody. Vectastain ABC 'Elite' avidin/biotin kit (Vector Labs. Burlingame, CA) was used for detecting the binding of all primary antibodies and Mayer’s haematoxylin was used as a counterstain. The immunohistochemical procedure was similar to those used in previous studies. RESULTS: The coracoclavicular ligaments could be clearly defined in all specimens. Both ligaments were characterized by a plane structure enlaced in fat tissue. The trapezoid substance originated primarily from the superior lateral tip of the coracoid, and inserted onto a bony hump at the anteroinferior aspect of the lateral clavicle. The conoid substance originated more from the medial aspect of the coracoid process posterior to the trapezoid and inserted at the posterior side of the clavicle medially to the trapezoid substance. The mid substance of the ligaments labelled for collagen types I with a narrow absence of labelling in 65% of entheses. Entheses of both ligaments showed characteristic fibrocartilaginous labelling of collagen type II and aggrecan. Labelling of link protein was also positive at entheses. Quantitative measurement of the labelling area for these molecules revealed a fibrocartilage zone of 10-15% in relationship to the ligament mid substance. In some specimens, especially type II collagen, showed a greater extent of labelling at the entheses at the coracoid process than at the entheses of the clavicle, but labelling pattern was comparable between the trapezoid and conoid ligament. In the mid substance of the CCL labelling for type II collagen, aggrecan and link protein was negative. Fat was found around all ligaments and also inbetween collagen fibres, separating each ligament in multiple parallel bands. Within fat tissue labelling of Laminin was positive in all samples to a great extend accounting for vascular supply. Vascularity was also characterized by positive labelling of endothelial cell markers (CD31). While no vascular structures were found at the entheses, vascular capillary were found in the fat tissue close to fibre bundles of the mid substance. CONCLUSION: The results of the present study show that both coracoclavicular ligaments, the trapezoid and the conoid ligament, are characterized by a plane structure. This is particularly of interest for clinicians, as plane ligaments are attributed by superior healing capacity compared to ligaments of solid round structure. The immunohistochemical findings of our study are that the CCL is highly fibrocartilaginous at both its clavicular and coracoidal entheses, but not in the ligament’s mid substance. Although fibrocartilage can be of pathological significance, from the results of our study we believe fibrocartilaginous entheses of the CCL are rather an evidence of the adaption to compression and shear force. In accordance to this, labelling of collagen type II was positive at the bony transition zone. The region positive for type II collagen included the mineralized and unmineralized fibrocartilage. In our samples these tissues also labelled for aggrecan and link protein. Aggrecan and link protein were constantly present in both ligaments of all samples. However, our study suggests that fibrocartilage at the CCL does not exceed an amount of 10-15% of its total structure. Thus, the zone of avascular fibrocartilage is fairly minimal compared to the broad section of mid substance. The mid substance of the CCL was characterized by type I collagen bundles enlaced in fat-tissue. Furthermore, fat was existent in between the two ligaments, and within the ligaments (endoligament fat). Adipose tissue within and around entheses has been reported to be a common feature of ligaments. However, the presence of fat tissue within the CCL as a normal feature is yet unclear. Apart from the common view that fat within ligaments is a sign of degeneration or age related change, we believe in the possibility that fat may promote stress dissipation or act as a mechanosensory organ at entheses. Since we found streaks of fat within all CCL near its enthesis, containing vessels, we believe, that strain on ligaments can bee seen as a normal existence and serves functional roles. Fat might help to dissipate stress away by providing a shifting pad between bone and ligament or between different fascicles of the ligament. The adipose tissue was characterized by a high amount of blood supply. Blood supply to the CCL is considered essential for ligament healing. Although various operative procedures restoring AC joint separations rely on the assumption of CCL healing, blood supply of the CCL was uncertain. Within the fat tissue around the ligaments vessels of varying calibre were present. Vascular structures strongly labelled for Laminin. Laminin is a component of the basal lamina which surrounds all vessels. We also found positive labelling of endothelial cell markers (CD 31). CD 31 was labelled in larger vessels and small capillary across CCL suggesting, that an extrinsic healing capacity is present in CCL. However, healed ligaments should be considered to have inferior morphological and biomechanical properties compared to native ligaments. CLINICAL RELEVANCE: The Results of our study help to understand the structure and properties of the coracoclavicular ligaments, which is necessary for both conservative and operative treatment of acromioclavicular joint separations. Poster No. 1079 • 56th Annual Meeting of the Orthopaedic Research Society