Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
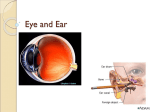
16 - Sensory Receptors and the Special Senses Taft College Human Physiology The Function of Sensory Receptors • Sensory receptors are of great survival value to the body. • They allow us to monitor changes in our internal and external environment and in so doing, maintain homeostasis. • The stimuli detected by the sensory receptors act to depolarize a membrane, then the impulses will travel to the CNS via afferent (sensory) neurons. • The nerve impulses for different senses are basically the same. • It is the connection to various parts of the brain that causes you to interpret them differently. • Theoretically, if you were able to surgically swap the attachment of cranial nerves for hearing and vision at the brain, you would hear lightning and see thunder. • We will focus on our attention on 2 main receptors: our eyes and ears. The Eye • Eye- The eye is a complex: • exteroreceptor (extero = outside) it is designed to pickup stimuli outside the body • photoreceptor (photo = light) it is designed to detect light stimuli. Innervation of the Eye • The eye is innervated by 4 cranial nerves. • II Optic nerve = nerve of vision. It has the sensory function of detecting light stimuli. • 3 cranial nerves provide motor impulses for eye movement. Eye movement is accomplished by several muscles that insert into the tough outer coat of the eye (sclera). • III Oculomotor • IV Trochlear • VI Abducens The Anatomy of the Eye Involved in the Physiology of Vision • The eyeball is made of 3 layers or coats (tunics): The outer fibrous coat, the middle vascular coat, and the inner nervous coat. • We will only discuss the inner nervous coat in detail and selected parts of the other 2 as needed to understand the basic physiology of sight. Optic Nerve 1. Fibrous coat 2. Vascular coat 3. Nervous coat = retina Nervous coat = retina • • • • • The retina receives light and converts it into nerve impulses. The retina contains 2 types of photoreceptors: rods (120 million) and cones (6 million)and is continuous with the optic nerve. Rods- high sensitivity. Respond to even low light levels. Night vision. Detect black, white, and shades of gray, no color. Detect shapes and movement. Cones- low sensitivity. Only functional in bright light. Color discrimination. 3 kinds of cones: one for each color- red, green, and blue. Colors of the spectrum other than red, blue ,and green are interpreted from interaction of all 3 kinds of cones. II Optic Nerve Retina with rods and cones Rods show summation, Cones do not. • • • • • • Rods Rods and cones are ‘wired’ differently. Cones Cones are ‘wired’ on a 1:1 ratio with bipolar cells. This allows for great resolution for detailed viewing, in color! But it does take a lot of light to allow this type of vision. Rods Rods are ‘wired’ on a ~100: 1 ratio with bipolar cells. Therefore many subthreshold stimuli may act together in an additive way to depolarize the neuron (bipolar cells) = summation. This allows for great sensitivity for night vision, but only in gray tones. Movement can be detected but resolution is poor. Nocturnal animals have many rods and a mirror like reflective layer that gathers Light Path light (tapetum lucidum), so have greater night vision sensitivity than our own. Cones Rods Bipolar cells Ganglion cells Optic (II) Nerve Fovea Centralis and Optic Disc • • • • • • • In the exact center of the posterior part of the retina is an area called the macula lutea. In this structure is a depression containing an area of highly packed cone cells, called the fovea centralis. Only cones are found here, no rods. The fovea centralis is the point of greatest visual acuity = ability to see detail. The optic disc is where the optic nerve exits the eye. There are so many axons (neurons) that converge to form the optic nerve here that there is no room for rods or cones. The optic disc is located medial to the fovea. The optic disc is commonly called is the ‘blind spot’ of the eye as no photo receptors (rods or cones) exist. It can be easily demonstrated. Other Important Structures of the Eye • • • • • Iris/Pupil - The iris is the colored portion of the eye shaped like a flattened donut. The iris is a muscular diaphragm with a central hole (pupil) that regulates the amount of light entering the eye. Cornea - Found in the outer fibrous coat and is continuous with the sclera (white of the eye) but transparent. Anterior 1/6 of eyeball that bulges forward to participate in focusing light (80%) on the retina. Corneal transplants are the most common and successful organ transplants. Due to avascular anatomy, therefore no rejection. Now, plastic corneas can be used as well. Cornea Other Important Structures of the Eye • • • • • • • Lens The lens is attached by suspensory ligaments that encircle the lens. These attach it to the ciliary body which surrounds the lens. The ciliary muscles in the ciliary body control the shape of the lens. The ciliary muscles are relaxed (tight ligaments and flattened lens) for distant viewing (far vision). The ciliary muscles are contracted (loose ligaments and rounded lens) for close inspection (near vision) of objects. Eye Fatigue - Since the ciliary muscles are contracted for close vision, it makes sense that your eyes may fatigue during reading or close inspection of objects. Changing the shape of the lens to focus the image on the retina is called accommodation. Ciliary muscles relaxed, suspensory ligaments tight flattened Ciliary muscles contracted can lead to fatigue suspensory ligaments relaxed rounded Physiology of Vision • • • • • • • • • • • • • • The rods contain a visual pigment called rhodopsin. In the presence of light rhodopsin breaks down into 2 parts: retinal and opsin . light Rhodopsin (dark color) retinal + opsin (colorless products) dark The reaction is the reverse in the dark. In light the rhodopsin splits, and it becomes colorless or ‘bleached’. The splitting of rhodopsin causes depolarization of the neuron and impulses travel to the brain and are perceived as light. The intensity of light will determine the number of rhodopsin molecules that split. Dark adaptation – In sunlight, rhodopsin molecules are continually broken down. When you go into dark theatre, you must wait for enough rhodopsin to build up so you can see (about 5 minutes for 50%). Light adaptation - An opposite effect happens when you go from the dark to a sunny place. Initially you may see nothing but bright light and no images, as so much rhodopsin is being broken down. Your eye has to decrease its sensitivity by breaking down all the rhodopsin. This why you squint and initially protect your eyes in bright light. Rhodopsin is bleached as fast as it is regenerated in the daylight. This is called ‘light adaptation’. The cones for color vision work with visual pigments as well but we will not cover. Eye Disorders • • • • • • • • • • • • Color Blindness: an inherited condition. The inability to distinguish certain color differences results from absence or deficiency of one or more of the 3 cone photopigments. Most common is red-green color blindness where the red or green sensitive pigment is missing and person cannot distinguish between red and green. It is a sex-linked trait, most commonly in males, as an inherited trait from their mother. Glaucoma: increased pressure of the aqueous humor due to blockage (canal of Schlemm). The pressure may cause irreversible damage to the retina. This is a painless condition affecting 2% over age 40. This why during an eye exam the clinician directs a puff of air or other method to detect your intraocular pressure. What drug has been used in treatment? Cataract: the lens becomes opaque. The lens proteins change shape. Usually caused by aging. Other causes: trauma, infection, diabetes, UV exposure). Corrected by surgical removal and implantation of an artificial lens. The earlier artificial lenses were fixed focus, now they may accommodate. Eye Disorders • • • • • • Refraction (light bending) abnormalities Nearsighted (myopic) (long eye) Light rays focus in front of retina. Need a concave corrective lens. Farsighted (hypermetropic) (short eye) Light rays focus behind the retina. Need a convex corrective lens. Astigmatism- blurred vision due to imperfections of the curvature of the cornea (or lens). Can be corrected by corrective lens. Eye Disorders • • • • Age-related (Senile) Macular Degeneration (AMD) Begins as hardening of the arteries in the fovea that deprives the retina of nourishment. May progress as new blood vessels grow over the macula lutea. Person loses ability to see straight ahead while peripheral vision is maintained. Early symptoms cause vision problems of blurring or distortion in central field progressing to blindness. Causes are not well understood but occurs over age 50. • Presbyopia - By age 40, the lens has lost much of its elasticity. So, the minimum distance that an object can be focused (near point of vision) moves out and away from the eyes. This is because the light rays cannot be bent enough by lens to focus on the retina. • Normal near point = 4 inches • • So, this is why bifocals are needed for reading after 40 years if age! This is a loss of accommodation and is called presbyopia (older persons vision). 40 years = 8 inches 60 years = 31 inches. Correcting Eye Disorders (FYI) • • 1. 2. 3. 4. 5. • LASIK = (Laser assisted in-situ keratomileusis.) = surgery to correct the curvature of the cornea for farsightedness, nearsightedness, and astigmatism. Anesthetic drops are placed in the eye. A circular flap of tissue is cut from the center of the cornea. The flap is folded out of the way and the cornea is precisely reshaped using a laser and computer. The circular flap is placed back in position over the treated area. A patch is placed over the eye overnight. The flap rapidly reattaches to the cornea. Corneal transplant -pic The Ear and Hearing • Introduction • The ear is a mechanoreceptor responsible for sensing hearing and equilibrium (balance). • The ear is a specialized receptor for sound waves. • VIII cranial nerve = vestibulocochlear (auditory) nerve is the nerve of hearing and balance. Anatomy and Physiology of the Ear • • • • • The ear consists of 3 major parts: the outer (external), middle, and inner(internal) ear. 1. External (outer) ear Consists of the auricle (pinna), a funnel like projection that collects sound waves and directs them to the external auditory canal (meatus) and on to the tympanic membrane (eardrum). The canal is lined by large hairs and ceruminous glands that secrete cerumen (earwax). The wax lining and hairs help to prevent dust and insects from damaging the tympanic membrane. Sound waves vibrate the tympanic membrane which vibrates the malleus = 1st of 3 ear ossicles. Anatomy and Physiology of the Ear • • • • • • • • • • 2. Middle Ear Consists of an air filled chamber in the temporal bone that houses the tiny bones of the ear = ear ossicles. The ear ossicles transmit and amplify vibrations of the tympanum to the inner ear, specifically to the oval window. The ear ossicles, in order from tympanum to inner ear: 1. Malleus = Hammer 2. Incus = Anvil 3. Stapes = Stirrup This ossicle transfers vibration to the oval window in the inner ear. Entering the middle ear chamber is the auditory tube (pharyngotympanic, or Eustachian) responsible for equalizing the pressure on both sides of the tympanic membrane. The equalization with atmospheric pressure can be accomplished by yawning or swallowing. What happens when you ears “pop”. Why does the sound become louder? Pathogens may travel through the eustachian tube from nose and throat to the middle ear. Anatomy and Physiology of the Ear • • • • 3. Inner ear (labyrinth) The inner ear is filled with liquid and houses the organs essential for hearing (cochlea) and equilibrium (semicircular canals and vestibule). The last of the ear ossicles, the stapes, is connected to a small membrane called the oval window. Located on the other side of this membrane is the fluid filled chamber, the cochlea. The cochlea contains fluid, channels, and membranes that transmit vibrations to the spiral organ (organ of Corti), the organ of hearing. The vestibulocochlear VIII nerve carries information to the brain. =Equilibrium =Hearing Physiological Steps in Sound Perception 1. 2. 3. 4. 5. 6. 7. 8. The auricle directs sound waves to the into the external auditory canal. The eardrum vibrates slowly in response to low frequency (low pitched sounds) and rapidly in response to high frequency sounds. Higher volume causes greater displacement of eardrum. Lower volume causes less displacement of the eardrum. The vibration of the eardrum is transmitted and amplified by the ear ossicles. The stapes pushes the oval window in and out. The movement of the oval window sets fluid (perilymph) pressure waves in motion in the cochlea. Pressure waves travel through the cochlea and cause the round window to bulge (9). The pressure waves push the basilar membrane back and forth. The hair cells on the basilar membrane hit the tectorial membrane. The bending of the hair cells causes impulse to travel along the vestibulocochlear nerve to the brain and is interpreted as sound. 2 Components of Sound 1. Volume = Loudness - determined by degree of movement the basilar membrane and number of hair cells stimulated. 3 1 2 4 5 9 7 8 6 8 2. Frequency = Pitch – determined by area of the basilar membrane that is stimulated, proximal = high frequency, distal = low frequency. Note- low freq sounds travel further than high freq. Physiological Steps in Sound Perception (continued) 8. • The hair cells on the basilar membrane hit the tectorial membrane. The bending of the hair cells causes impulse to travel along the vestibulocochlear nerve to the brain and is interpreted as sound. The spiral organ (Organ of Corti), the actual organ of hearing consists of 3 components, the basilar membrane, hairs cells, and tectorial membrane. Pitch Pitch • Pitch is perceived as a result of the region of basilar membrane that is ‘tuned’ to vibrate at specific pressure frequencies set up in the cochlear fluid by movement of the oval window. • The fibers in the basilar membrane that span its width (like harp strings) along the length of the cochlea, vibrate in resonance with specific wave frequencies. – The fibers are shortest near the oval window and get progressively longer toward the cochlear apex. – The shorter fibers vibrate with high frequency waves (20k Hz) and the longer fibers vibrate with lower frequencies (20 Hz). HIGH FREQUENCY MEDIUM FREQUENCY LOW FREQUENCY Volume and Pitch = 2 Components of Sound • Volume = Loudness is based on degree of displacement of the basilar membrane – bending of hairs is in direct proportion to volume. • Pitch = Frequency is based on the region of the cochlea the vibrations stimulate. Hearing Loss • • • • If your ears ever ring following a loud noise, you have done permanent damage to your hair cells. Loud noise causes the hair cells to crash into the tectorial membrane and bend the hair cells. It then takes greater volume for them to respond. The purpose of a hearing aid is to raise the volume of the sound so it may move the basilar membrane enough for the damaged hair cells to reach the tectorial membrane and send impulses to the brain. Tectorial Membrane Hair Cells Basilar Membrane Healthy Damaged Physiology of Equilibrium • Equilibrium of the body is reached through the interpretation of responses of 1) head to movement, 2) visual input, 3) stretch receptor input from muscles and tendons. • We will discuss the input from the inner ear which is effected by movement of the head. • 2 types of balance (equilibrium) are assisted by the inner ear: – Static equilibrium – dynamic equilibrium. • • • • • • • • 1. Static Equilibrium is the maintenance of body position (mainly the head) relative to the force of gravity. Mainly due to sensing of movement in the vestibule by hairs cells similar to those used in hearing. These receptors sense linear acceleration movement of the head only, not rotational movement. The hair cells project into a membrane called the otolithic membrane that is gelatinous in nature. Otoliths (calcium carbonate crystals) sit on the surface of this membrane. As tilt your head forward or side to side, or move up and down in an elevator, the heavy otoliths and otolithic membrane bend the hairs of the hair cells. The same thing happens when you stop moving, the inertia in the membrane bends the hairs. Depending on which direction the hair is bent, it either causes depolarization, so nervous impulses are triggered in the vestibular nerve. These impulses are transmitted to the brain stem (vestibular nuclei) and cerebellum for interpretation with other input and then a skeletal motor response is sent. Static Equilibrium Otoliths respond to gravity Hair cells Dynamic Equilibrium • • • • • 2. Dynamic Equilibrium is the maintenance of body position (mainly the head) in response to sudden movements such as rotation, acceleration, and deceleration (balance while moving). 3 semicircular canals that lie at right angle to each other in 3 planes (2 vertical, 1 horizontal), are the structures for sensing dynamic equilibrium. These structures are lined with hair cells that are imbedded in gelatinous membrane. As the head moves, the endolymph in the canals flows over the hairs and bends them. Since the 3 canals are in 3, 90 degree planes, rotational movement in any plane and direction will be sensed. If you keep spinning around, the endolymph will eventually spin at a similar speed. When you stop, it keeps going and bends the hairs again, only in the opposite direction. This tells the brain you have slowed or stopped. Key Point for equilibrium sensing: the rigid bony inner ear with attached hair cells moves with the body, while the fluids and gels with otoliths are free to move at various rates depending on the forces acting on them. Motion Sickness • • • • Motion sickness- a common equilibrium disorder. Probably due to sensory mismatch of visual input sensing a fixed position (your cabin on a ship) and your vestibule sensing movement (the rough seas). The brain receives conflicting info and is confused which somehow leads to motion sickness. Warning signs that precede nausea and vomiting include: increased salivation, pallor, rapid deep breathing, sweating. Prevent before the fact by using antimotion drugs (ex: Dramamine- dimenhydrinate, scopolamine- skin patch) that depress vestibular input.