Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Donald O. Hebb wikipedia , lookup
Cortical stimulation mapping wikipedia , lookup
History of anthropometry wikipedia , lookup
Craniometry wikipedia , lookup
Transcranial Doppler wikipedia , lookup
Brain damage wikipedia , lookup
Dual consciousness wikipedia , lookup
Lumbar puncture wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
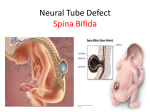
Lecture 10 Ultrasound Evaluation of the Fetal Neural Axis Holdorf OBSTETRICAL ULTRASOUND PART I Take-a-ways… The Banana Sign “Bent” Cerebellum The part of the brain at the back of the skull in vertebrates. Its function is to coordinate and regulate muscular activity. Absent Cisterna Magna One of three principal openings in the subarachnoid space between the arachnoid and pia mater layers of the meninges surrounding the brain. The openings are collectively referred to as cisterns. The Lemon Sign Frontal bossing of the cranium Temporal bones The Banana Sign explained: Seen on axial imaging through the posterior fossa and is associated with Chiari II Malformation. The Banana sign describes the way the cerebellum is wrapped tightly around the brain stem as a result of spinal cord tethering and downward migration of posterior fossa content. The cisterna magna gets obliterated and the shape of the cerebellum takes on the appearance of a banana. This sign persists into the second and third trimesters. The Lemon sign explained: The lemon sign is the medial inward displacement and scalloping of the frontal bones of the fetal calvarium. This is often associated with an open spina bifida (seen under ultrasound as the widening and flattening of the posterior elements of the spine. The formation of the Neural Axis The stuff that is always on the boards… The lateral, 3rd, and 4th ventricles Ventriculomegaly Ventriculomegaly is a brain condition that occurs when the lateral ventricles become dilated. The most common definition uses a width of the atrium of the lateral ventricle of greater than 10 mm. This occurs in around 1% of pregnancies. When this measurement is between 10 and 15 mm, the ventriculomegaly may be described as mild to moderate. Ventriculomegaly When the measurement is greater than 15mm, ventriculomegaly may be classified as more severe. Enlargement of the ventricles may occur for a number of reasons, for example due to loss of brain volume (perhaps due to infection or infarction), or due to impaired outflow or absorption of cerebrospinal fluid from the ventricles. Often, however, there is no identifiable cause. This diagnosis is generally found in routine fetal anomaly scans at 18–22 weeks gestation. It is one of the commonest abnormal brain findings on prenatal ultrasound, occurring in around 1-2 per 1000 pregnancies. In many cases of mild ventriculomegaly, however, there is resolution of ventriculomegaly during the pregnancy. Ventriculomegaly is also known to be associated with other malformations such as agenesis of the corpus callosum (a broad band of nerve fibers joining the two hemispheres of the brain), spina bifida, and heart defects. Fetuses with both isolated ventriculomegaly and with other anomalies have an increased risk of having a chromosomal abnormality, including that of Down Syndrome . Anencephaly Cephalic disorder that results from a neural tube defect that occurs when the cephalic (head) end of the neural tube fails to close, usually between the 23rd and 26th day of pregnancy, resulting in the absence of a major portion of the brain, skull, and scalp. Children with this disorder are born without a forebrain, the largest part of the brain consisting mainly of the cerebral hemispheres (which include the isocortex, which is responsible for higher level cognition, i.e., thinking). The remaining brain tissue is often exposed - not covered by bone or skin. Anencephaly Spina bifida (Latin: "split spine") is a developmental birth defect involving the neural tube: incomplete closure of the embryonic neural tube results in an incompletely formed spinal cord. In addition, the vertebrae overlying the open portion of the spinal cord do not fully form and remain unfused and open. Spina Bifida The spinal opening allows the abnormal portion of the spinal cord to protrude through the opening in the bones. There may or may not be a fluid filled sac surrounding the open spinal cord. Other neural tube defects include anencephaly, a condition in which the portion of the neural tube which will become the cerebrum does not close, and encephalocele, which results when other parts of the brain remain unfused Spina bifida malformations fall into three categories: spina bifida occulta, spina bifida cystica (myelomeningocele), and meningocele. The most common location of the malformations is the lumbar and sacral areas of the spinal cord. Myelomeningocele is the most significant form and is that which leads to disability in most affected individuals. The terms spina bifida and myelomeningocele are usually used interchangeably. Spina bifida can be surgically closed after birth, but this does not restore normal function to the affected part of the spinal cord and an individual with this condition will have dysfunction of the spinal cord and associated nerves from the point of the open defect and below. Intrauterine surgery for spina bifida has also been performed and the safety and efficacy of this procedure is currently being investigated. Holoprosencephaly A type of cephalic disorder. This is a disorder characterized by the failure of the prosencephalon (the forebrain of the embryo) to develop. During normal development the forebrain is formed and the face begins to develop in the fifth and sixth weeks of human pregnancy. (The condition also occurs in other species, as with Cy, the Cyclops kitten.) Holoprosencephaly is caused by a failure of the embryo's forebrain to divide to form bilateral cerebral hemispheres (the left and right halves of the brain), causing defects in the development of the face and in brain structure and function. Holoprosencephaly Dandy-Walker syndrome DWS, or Dandy-Walker complex, is a congenital brain malformation involving the cerebellum and the fluid filled spaces around it. The Dandy-Walker complex is a genetically sporadic disorder that occurs one in every 25,000 live births, mostly in females. Dandy-Walker Syndrome/absent pons and cerebellum in 7y/o The key features of DWS are an enlargement of the fourth ventricle, the space containing cerebrospinal fluid between the medulla and the cerebellum, a partial or complete absence of the cerebellar vermis, the posterior midline area of cerebellar cortex responsible for coordination of the axial musculature, and cyst formation near the internal base of the skull. An increase in the size of the fluid spaces surrounding the brain as well as an increase in pressure may also be present. The syndrome can appear dramatically or develop unnoticed. And now…the other stuff Chapter 10 outline Neural Tube Defects (NTD) Spina Bifida Anencephaly Encephalocele Iniencephaly Intracranial Abnormalities Hydrocephaly (Ventriculomegaly) Hydranencephaly Holoprosencephaly Porencephaly Dandy-Walker Syndrome Agenesis of the Corpus Callosum Schizencephaly Lissencephaly Choroid Plexus Cysts Choroid Plexus Papillomas Microcephaly Intracranial Tumors Terminology Rachischisis: Completely open spine with Herniation and or destruction of the spinal cord Spina Bifida occulta: Failure of closure of the vertebral column without any associated external abnormalities. Rarely associated with neurologic complications. Spina Bifida Apperta: Failure of closure of the vertebral column with apparent external abnormalities and neurologic complications Meningocele: Herniation of the meninges through a schisis defect Myelomeningocele: Herniation of the mengenges and neural tissue through a schisis defect. Neural Tube Defects On the boards since 1991. There are MANY questions regarding NTDs…study this!!!! A gamut of CNS anomalies may result from a failure of the normal process of Neurulation (Embryology). The lesions are frequently open. This allows CSF to pour into the amniotic cavity, causing elevation of the maternal serum and amniotic fluid levels of AFP. Routine prenatal testing that reveals elevated MSAFP levels is and indication for a level II sonogram. When the sonogram does not find the cause of elevated AFP, an amniocentesis is recommended. Spina Bifida Is a general term for lack of closure of the vertebral column. Prognosis depends on the severity of the lesion. Pathology Presence of a Myelomeningocele, a protruding sac which may contain meninges and spinal cord. May occur anywhere along the spinal column but lumbar region is most common. Variable in size and content. Sonographic findings in Transverse view: Splaying of posterior ossification centers into a U or V shape. When sac is intact, a cystic structure may be seen extending from the back. Appearances include a small cystic structure, a cyst with septations and or solid matter. Sonographic Findings on Sagittal View: Splaying of parallel lateral ossification centers Soft tissue defect or discontinuity of skin and muscle of posterior back An image of a Myelomeningocele in Transverse view Splayed ossification centers in transverse view. Soft tissue defect or discontinuity of skin and muscle of posterior back on Sagittal view. Spina Bifida Continued… Intracranial Lemon sign-frontal bossing of cranium Banana sign-dislocated cerebellum and obliteration of the cistern magna Chiari type II malformation-variable displacement of cerebellum, 4th ventricle and medulla oblongata through the foramen magnum The lemon and Banana signs The lemon sign ANENCEPHALY Anencephaly occurs at 2-3 weeks when the anterior neuropore fails to fuse. Pathology Absence of cranial vault and cerebral hemispheres (functioning brain) Portions of midbrain and brain stem may be present Other features include bulging eyes, macroglossia and a very short neck. Sonographic findings Fetal head should be identifiable by 12 weeks, definitively by 15 weeks. Major portions of cranium and intracranial structures are absent: orbits and face are usually present Associated Polyhydramnios in half the cases Anencephaly Encephalocele Protrusion of the intracranial contents through a bony defect of the skull can also be called a cephalocele. Occipital encephaloceles are most frequent. There is a defect in the cranium. Pathology Boney defect in calvarium with herniation of brain and or meninges outside of cranium Classified as occipital, frontal, or parietal Hydrocephalus is present 80 % of the time in occipital lesions. Sonographic findings Mass extending from calvarium, may be totally cystic, have some meninges (cranial Meningocele, or may contain brain (encephalocele) Cranial disruption is occasionally seen Associated with hydrocephalus, Polyhydramnios Encephalocele Iniencephaly Iniencephaly is a dramatic NTD characterized by an exaggerated spinal Lordosis, cervical Rachischisis and an occipital encephalocele Sonographic findings Exaggerated, hyperextension of the fetal head Demonstration of cervical spina bifida Iniencephaly Iniencephaly A type of cephalic disorder. It is a rare neural tube defect that combines extreme retroflexion (backward bending) of the head with severe defects of the spine. The affected infant tends to be short, with a disproportionately large head. Diagnosis can be made immediately after birth because the head is so severely retroflexed that the face looks upward. The skin of the face is connected directly to the skin of the chest and the scalp is directly connected to the skin of the back. Generally, the neck is absent. Most individuals with iniencephaly have other associated anomalies such as anencephaly, encephalocele (a disorder in which part of the cranial contents protrudes from the skull), hydrocephalus, cyclopia, absence of the mandible (lower jaw bone), cleft lip and palate, cardiovascular disorders, diaphragmatic hernia, and gastrointestinal malformation. The disorder is more common among females. Iniencephaly Intracranial Abnormalities Hydrocephaly AKA Ventriculomegaly Dilatation of the ventricular system secondary to the increase in the amount of CSF. Classifications Aqueductal Stenosis is the cause 43% of the time Hydrocephalus caused by narrowing of the aqueduct of Sylvius (3rd ventricle outflow) Communicating hydrocephalus is the cause 38% of the time Dilatation of all ventricles and subarachnoid space caused by an obstruction to CSF follow outside the ventricular system. Dandy-Walker Syndrome is the cause 12% of the time Idiopathic in 7% of the time Cause unknown Bilateral ventriculomegaly diagram of the ventricular system, showing the lateral ventricle, the third ventricle, and the fourth ventricle. Ventriculomegaly cont… Sonographic findings In the first trimester CSF seen in the lateral ventricle and possibly compressing choroid plexus In the 2nd and 3rd trimester Normal ventricular configuration…just dilated Presence of excess fluid in lateral ventricles, with an atrial measurement exceeding 10mm Dangling choroid plexus Observe brain echogenicity-echogenic foci in parenchyma may suggest intrauterine infection Can have Polyhydramnios, abnormal fetal lie, fetal ascites, encephalocele, and Dandy-Walker. An image measuring the atrial measurement exceeding 10mm a “Dangling” choroid plexus. DEFINE FILLY’s RULE Ventriculomegaly is a brain condition that occurs when the lateral ventricles become dilated. The most common definition uses a width of the atrium of the lateral ventricle of greater than 10 mm. This occurs in around 1% of pregnancies. When this measurement is between 10 and 15 mm, the ventriculomegaly may be described as mild to moderate. When the measurement is greater than 15mm, the ventriculomegaly may be classified as more severe. Enlargement of the ventricles may occur for a number of reasons, such as loss of brain volume (perhaps due to infection or infarction), or impaired outflow or absorption of cerebrospinal fluid from the ventricles. Often, however, there is no identifiable cause. The interventricular foramen may be congenitally malformed, or may have become obstructed by infection, hemorrhage, or rarely tumor, which may impair the drainage of cerebrospinal fluid, and thus accumulation in the ventricles. This diagnosis is generally found in routine fetal anomaly scans at 18–22 weeks gestation. It is one of the more common abnormal brain findings on prenatal ultrasound, occurring in around 1–2 per 1000 pregnancies. In many cases of mild ventriculomegaly, however, there is resolution of ventriculomegaly during the pregnancy DEFINE FILLY’s RULE Hydranencephaly Means “water, no brain”. Total or near total absence of the cerebral hemispheres. Cause could be intrauterine infarction secondary to bilateral ICA occlusion or malformation. Sonographic findings Microcephaly Large anechoic areas in cranial vault Variable presence of 3rd ventricle Polyhydramnios Hydranenephaly HOLOPROSENCEPHALY (this is always on the boards) Three classifications 1. Alobar (Most severe) Large single cavity with minimal amount of cerebral tissue surrounding it, fused thalami, and facial syndrome with hypotelorism and other craniofacial anomalies 2. Semilobar More cerebral tissue is present. Occipital lobe is present. Associated cleft palate and cleft lip 3. Lobar Interhemispheric fusion is developed, but there is variable degree of fusion and CSP is absent Sonographic findings Fetal cranium appears as a large cystic space with some peripheral cerebral tissue Presence of a single midline ventricle Craniofacial abnormalities including a proboscis, severe hypotelorism, Cycolpia Appearance varies with severity of malformation. . Alobar (Most severe) In Holoprosencephaly, remember this hint…”THE FACE PREDICTS THE BRAIN”. Porencephaly The presence of cystic areas within the cerebral parenchyma. The etiology is believed to be the result of lysis of in-utero intracranial hemorrhage or cystic encephalomalacia. Sonographic findings Simple cystic structures within the cerebral parenchyma. Porencephaly A type of cephalic disorder involving an extremely rare disorder of the central nervous system involving a cyst or cavity in a cerebral hemisphere. The cysts or cavities are usually the remnants of destructive lesions, but are sometimes the result of abnormal development. Porencephaly most likely has a number of different, often unknown causes, including absence of brain development and destruction of brain tissue. More severely affected infants show symptoms of the disorder shortly after birth, and the diagnosis is usually made before age 1. Signs may include delayed growth and development, slight or incomplete paralysis, decreased muscle tone, seizures and macrocephaly or microcephaly. Individuals with porencephaly may have poor or absent speech development, epilepsy, hydrocephalus, spastic contractures (shrinkage or shortening of muscles), and mental retardation. Porencephaly Dandy-Walker Syndrome Indicates the association of the following: Large Cistern Magna Ventriculomegaly of varying degree Cerebellar Vermain Agenesis (complete or partial), through which the 4th ventricle communicates with the cystic structure in the posterior fossa. There is obstruction of the 4th ventricle outflow and subsequent cystic enlargement of the posterior fossa. Sonographic findings Large midline cystic structure in posterior fossa Enlargement of posterior fossa Assoc. with ventriculomegaly and Polyhydramnios Dandy-Walker Syndrome/fluid filled spaces in the posterior fossa Agenesis of the Corpus Callosum Absence of the corpus callosum results from a chromosomal abnormality. May be complete or partial. Is frequently associated with other syndromes and or anomalies. Sonographic findings Absent Cavum septum Pellucidum Lateral ventricles displaced upward and outward with a teardrop shape. Enlarged occipital horn 3rd ventricle enlarged and displaced superiorly. The corpus Callosum The corpus callosum (from Latin: "tough body"), is a wide, flat bundle of neural fibers beneath the cortex at the longitudinal fissure. It connects the left and right cerebral hemispheres and facilitates inter-hemispheric communication. It is the largest white matter structure in the brain. Teardrop ventricle with Agenesis of the Corpus Callosum Schizencephaly Abnormal clefts in the cerebral hemispheres. The brain appears split into anterior and posterior parts Schizencephaly A rare developmental disorder characterized by abnormal slits, or clefts, in the cerebral hemispheres. Schizencephaly can be distinguished from porencephaly by the fact that in schizencephaly the cyst is lined by heterotopic grey matter while a porencephalic cyst is lined by white matter. Individuals with clefts in both hemispheres, or bilateral clefts, are often developmentally delayed and have delayed speech and language. Individuals with smaller, unilateral clefts (clefts in one hemisphere) may be weak on one side of the body and may have average or near-average intelligence. Patients with schizencephaly may also have varying degrees of microcephaly, mental retardation, hemiparesis (weakness or paralysis affecting one side of the body), or quadriparesis (weakness or paralysis affecting all four extremities), and may have reduced muscle tone (hypotonia). Most patients have seizures and some may have hydrocephalus. Schizencephaly/destructive brain lesion Lissencephaly The surface of the brain lacks the normal sulci and gyri and appears smooth. Diagnosis is not made until the 3rd trimester. Choroid Plexus cyst The significance is an infrequent association with aneuploidy (Trisomy 18). Can be lateral, bilateral, small, large… Choroid plexus Papillomas Are benign tumors of the choroid plexus. Most frequently are unilateral and occur at the level of the atrium of the lateral ventricle. They are frequently associated with hydrocephalus Lissencephaly Choroid Plexus cyst Microcephaly Considered a symptom of many etiologic disturbances. Defined as a small head circumference below 3 standard deviations of normal. Sonographic findings Small HC (other parameters are normal) Sloping forehead, and disproportion between size of face and skull Microcephaly Intracranial tumors Rare. Teratomas are the most common. Prognosis is dismal Sonographic findings Loss of normal intracranial architecture Presence of space-occupying lesion Intracranial Tumor Homework 1. Rhombencephalon: what is it, and how is it visualized by ultrasound? 2. The ventricular system: Draw and label the ventricle system 3. Choroid plexus: what are they, what do they do, and where are they located in the brain? 4. Ventriculomegaly: how is it defined? Show this with an image. What is measured? What are the upper limits of normal? What measurement is considered abnormal? 5. Define hydrocephalus 6. Is hydrocephalus usually isolated? Explain 7. Are there any surgical options available for the parents of the fetus diagnosed with intrauterine hydrocephalus? 8. Spina Bifida: Define occulta and aperta. 9. What is myeolmeningocele? 10.What is Arnold-Chiari or Chiari Type II malformation? 11. What is the banana sign? 12. What is the lemon sign? 13. Define a Cephalocele. 14. What is a cranial Meningocele? 15. What is an encephalocele? 16. Define Holoprosencephaly. 17. What is agenesis of the Corpus Callosum? 18. What is Dandy-Walker Complex? 19. What is porencephaly? 20. What is Hydranencepahly? 21. What is Microcephaly? 22. Is there such a thing as intracranial calcification? Explain. 23. Please discuss the occurrence of choroid plexus cysts.