Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Coronary artery disease wikipedia , lookup
Heart failure wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Jatene procedure wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Myocardial infarction wikipedia , lookup
Cardiac surgery wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Congenital heart defect wikipedia , lookup
Atrial fibrillation wikipedia , lookup
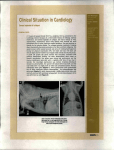
156 IRREGULAR PULSE IN A NINE-YEAR OLD GIRL MOHAMMED IRFAN QURESHI, MD, MRCPI; IBRAHIM H. AL-A YED, MRCP (UK), DCH; ABDULLAH AL-JARALLAH, CABP,MBChE ./ Figure I. ECG of a 9-year old girl with an irregular pulse. Case history A 9-year old girl was referred to the pediatric clinic for evaluation. She was accidentally discovered to have an irregular and slow pulse. Clinically she was looking well. Her blood pressure was 101/42. Her growth parameters were normal. The one-minute pulse was 40/minute, slow and irregular. All peripheral pulses were palpable. From the Departments of Pediatric Emergency and Ambulatory Care Unit (Drs. Qureshi & AI-Ayed), and Pediatric Cardiology (Dr. AI-Jarallah), King Khalid University Hospital, Riyadh, Saudi Arabia. Address reprint requests and correspondence to Dr. Qureshi: Department of Pediatric Emergency and Ambulatory Unit, King Khalid University Hospital, P.O. Box 7805, Riyadh 11472, Saudi Arabia. Hearing was normal. CVS examination revealed a grade 2/6 systolic murmur at the apex. Heart sounds were normal. An ECG was done which is shown above: Comment on the ECG. What is the prognosis? Diagnosis Congenital Complete Heart block (Third-Degree A V Block) Discussion This is a twelve-lead ECG with a rhythm strip showing P-waves and QRS complexes having no - ECG QUIZ constant relationship to each other. The QRS complexes are narrow, suggesting the pacemaker is in the A V node or high in the His bundle. P-waves are more frequent than R-waves, the RR interval is fairly regular and the atrial rate is more than the ventricular rate. In atrioventricular dissociation, the atrial rate is slower than the ventricular rate. I Surgically induced or acquired third-degree heart block usually shows a wide QRS complex. Clinical examination may reveal prominent peripheral pulse as a result of large ventricular stroke volume and peripheral vasodilatation. Systolic BP is elevated; jugular venous pulsation occur irregularly and may be large at times (cannon waves). Congenital complete heart block may be seen as an isolated anomaly or may be associated with structural defects such as L-transposition of the great arteries. It may be associated with matemallupus erythematosus.2 Autoimmune disease accounts for 60% to 70% of all congenital heart block and 80% of cases with a structurally normal heart. 2 157 Asymptomatic children with congenital heart block fall into Class II of the American Heart Association indications for pacemaker implantation and may not require pacemaker therapy. However, prospective studies have shown that those patients with a mean heart rate of less than 50 beats/m were likely to develop cardiac complications of sudden death, episodes of dizziness with or without syncope (StokesAdams attacks) or excessive fatigue. In view of this the implantation of a permanent cardiac pacemaker is recommended. 3 The family was advised accordingly and we are waiting for a decision from them. The child is stable otherwise and is followed up in the clinic. References I. Park MK, Guntheroth WG. How to read pediatric ECGs. Mosby Year Book Inc 1992;127-28. 2. Behrman RE, Kliegman RM, Arvin AM. Nelson Textbook of Pediatrics, 1996. 15th edition: 1342. 3. Kugler JD, Danford DA. Pacemakers in children: an update. Am Heart J 1989; 117:665-8.