Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Diseases of poverty wikipedia , lookup
Compartmental models in epidemiology wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Transmission (medicine) wikipedia , lookup
Infection control wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Public health genomics wikipedia , lookup
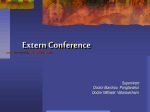
APPROACH TO LYMPHADENOPATHY Presented by: Hamad Alkhalaf, General Pediatric Fellow Children’s Hospital of Eastern Ontario Date: May 10, 2013 Objectives • Define lymphadenopathy • Develop a systematic approach to the evaluation and management of lymphadenopathy • Discuss the differential diagnosis of localized and generalized lymphadenopathy • Recognize worrisome features of lymphadenopathy Introduction • Lymph nodes, in conjunction with the spleen, tonsils adenoids, thymus, and peyer’s patches, are highly organized centers of immune cells that filter antigen from the extra cellular fluid. • Body has 600 lymph nodes. • Examining the lymph node is an important aspect of the general physical examination of any pediatric patient . Introduction • Lymph nodes are normal structures and a certain lymph nodes may palpable in healthy children. • Because of its association with malignancy, lymphadenopathy can be a major source of parental anxiety. Anatomy of Lymph node: Anatomy of Lymph node: • Lymph (ultra filtrate of blood) is collected in lymphatic capillaries present throughout the body except the brain and heart. • Lymph moves slowly under a low pressure ultimately drained into either: right lymphatic duct (lymph from the pt upper body) thoracic duct (rest of the body) • These ducts ultimately drain into the venous system (Rt and Lt subclavian veins) Anatomy of Lymph node: • A working knowledge of the nodal basins and the anatomy of the regions they drain is helpful in formulating a differential diagnosis for lymphadenopathy Pathogenesis • Lymph node enlargement can be caused by the following mechanisms: 1. proliferation of normal cells that comprise the lymph node (in response to antigen stimuli) a. benign hyperplasia b. vascular engorgement and edema secondary to local cytokine release c. suppuration secondary to tissue necrosis Pathogenesis 2. Entry of large number of cells exogenous to the node like: a. neutrophils b. metastatic neoplastic cells 3. Deposition of foreign materials like lipid storage disease Epidemiology • In one review, lymphadenopathy present in: 44% well child visits 64% sick visits (in children < 5 years of age ) Herzog LW, Prevalence of lymphadenopathy of the head and neck in infants and children. Clin Pediatr (Phila) 1983; 22:485 • Prevalence of malignancy among the patients seen in primary care setting is relatively rare. Epidemiology • In contrast, prevalence of malignancy in lymphadenopathy biopsies performed in pediatric referred centers ranges from 13 – 27% Lake AM, Oski FA. Peripheral lymphadenopathy in childhood. Ten-year experience with excisional biopsy. Am J Dis Child 1978; 132:357 Soldes OS, Younger JG, Hirschl RB. Predictors of malignancy in childhood peripheral lymphadenopathy. J Oediatr Surg 1999; 34:1447 • In the largest series studies, 239 children underwent peripheral lymph node biopsies for evaluation of lymphadenopathy Epidemiology • The following etiologies were noted 1. idiopathic reactive hyperplasia (52%) 2. Granulmatous disease (cat scratch, atypical mycobacterium, TB, fungal, histocytosis in 33%) 3. malignancy (13%) 2/3 of them has Hodgkins disease 4. Chronic dermatopathic or bacterial infections (3%) Epidemiology • The prevalence of lymphadenopathy varies with age and site • Small occipital and post auricular nodes, for example, are common in infants, but not an older children • In contrast, cervical and inguinal nodes are more common after 2 yrs of age Epidemiology • Epitrochlear and supraclavicular adenopathy are uncommon at any age • In neonates, lymph nodes are barely perceptible •M=F • Race is not a factor in most lymphadenopathy Epidemiology • Uncommon causes of lymphadenopathy should be considered in certain areas e.g. HIV in Africa TB and other tropical diseases in developing nations Important definitions • Normal lymph node diameter is up to - 1 cm (in most regions) - 0.5 cm (epitrochlear region) - 1.5 cm (inguinal region) • Lymphadenopathy Pathologic swollen lymph node (regardless of the cause) • Lymphadenitis Inflamed lymph node usually by infectious cause Important definitions • Localized lymphadenopathy Abnormal enlargement of one (or two contagious) LN • Generalized lymphadenopathy abnormal enlargement of two or more noncontiguous LN Important definitions • Acute lymphadenopathy < 2 weeks duration • Subacute lymphadenopathy 2 – 6 weeks duration • Chronic lymphadenopathy > 6 weeks duration Bacterial lymphadenitis Cat scratch tularemia atypical mycobacteria Kawasaki First visit evaluation • Stepwise management (detailed Hx, full Physical examination +/- less invasive tests) aid in selecting appropriate patients for further workup. History • HPI duration and location of lymphadenopathy local symptoms - cough, pharyngitis, dental problems, recent onset of fever, contact with sick pts, skin lesions Associated constitutional symptoms - prolonged fever, wt loss, night sweats, skin rash, bone or joint symptoms History • Exposure hx (food, animal, travel) a. ingestion of unpasteurized animal milk (brucella, TB) b. Animal contact: cats (cat scratch disease & toxoplasmosis), goats (brucellosis), rabbits (tularemia), prairie dogs (bubonic plague), tick bites, flea, and mosquito bites (lyme disease, bubonic plague, tularemia) c. travel hx (e.g. tularemia, TB, measles, rubella, leishmaniasis, typhoid fever) History • Past History Recurrent infections, skin abscess, supporative adenitis (CGD, HIV) Autoimmune disease (autoimmune lymphoproliferative syndrome) B.Asthma ( churg –strauss syndrome) History • Immunization status - diphteria, measles, rubella • Medications - Amoxicillin rash in EBV - Recent steroid therapy History Allopurinol Drugs that cause lymphadenopathy Atenolol Captopril Carbamazepine Cephalosporins Gold Hydralazine Penicillin Phenytoin Primidone Pyrimethamine Quinidine Sulfonamides Sulindac History • Family hx malignancy, autoimmune, inflammatory, storage diseases • Social hx Recent immigration Physical Examination • General appearance (including vital signs) • Growth parameters (wt loss of > 10% is a red flag) • Head - scalp infection (tinea capitis) - conjunctival injection (Kawasaki disease, oculoglandular syndrome) - nasal obstruction (rhabdomyosarcoma, nasopharyngeal carcioma, URTI) - Oropharynx and ears (dental proplems, pharyngitis, herpetic gingivostomatitis) - neck (range of motion, other LN involvement, transillumination) Examine all lymph nodes • Assess location, size, consistency, fixation, tenderness, other lymph nodes involvement. Lymph node group Causes Occipital Common: scalp infections (including tinea capitis, lice), insect bites, seborrhea, roseola (human herpesvirus 6, HHV6) Less common: Rubella, acute lymphoblastic leukemia) Posterior auricular Rubella, roseola (HHV6, HHV7) Anterior auricular (preauricular) Common: Eye or conjuctival infections (e.g. adenovirus, oculoglandular syndrome) Less common: cat scratch disease, tularemia, listeriosis Submental Tongue, gum, buccal mucosal, and dental infections (eg, gingivostomatitis), group B streptococcal infection (in infants <2 months of age) Submaxillary (submandibular) Tongue, gum, buccal mucosal, and dental infections; dental caries; chronically cracked lips) Examine all lymph nodes Lymph node group Causes Cervical Anterior: common: Viral upper respiratory infections, infections of pharynx, oral cavity, or head and neck; primary bacterial adenitis, tuberculosis, Epstein-Barr virus, cytomegalovirus, cat scratch disease, tularemia, nontuberculous mycobacterium, mycobacterium tuberculosis Less common: Kawasaki disease, tularemia, toxoplasmosis, non-infectious causes (eg, Hodgkin’s disease, lymphosarcoma, neuroblastoma, rhabdomyosarcoma, sarcoidosis) Posterior: Toxoplasmosis, Epstein-Barr virus, rubella. Supraclavicular Malignancy (lymphoma or metastatic disease) Examine all lymph nodes Lymph node group Causes Axillary Common: Cat scratch disease, pyogenic infections of upper arms, brucellosis, reactive response to disruption in skin integrity Less common: Brucellosis, Yersinia pestis, rat-bite fever, toxoplasmosis, rheumatologic disease of the hand or wrist Epitrochlear Common: Viral diseases, sarcoidosis, tularemia, infection of hands Less common: cat scratch disease, tularemia, secondary syphilis, rheumatologic disease of the hand or wrist. Inguinal Common: Genital herpes, primary; syphlis, gonococcal infection, lymphoma Less common: Yersinia pestis, chancroid, lymphogranuloma venereum Popliteal Local infection Physical Examination • Chest Additional sounds (histoplasmosis, LCH, Churg-strauss) Respiratory distress Physical Examination • Abdomen Hepatosplenomegaly a. infections (EBV, CMV, HIV, leishmaniasis, TB, syphilis, lyme disease) b. Autoimmune (JIA, SLE, serum sickness, lymphoproliferative disorders) c. Malignancy (leukemia, lymphoma, secondary metastasis) d. lipid storage diseases (Gaucher’s ,Nieman pick disease) Abdominal mass (neuroblastoma, rhabdomyosarcoma) Physical Examination • Genitalia signs of STDs. • Skin generalized rash (viral, Kawasaki) localized lesions (cat scratch disease, Tularemia, staph aureus, GAS, HSV, etc) insect or mosquito bites petechiae or bruises (Bone marrow involvement) Important considerations • Formulating your DDx requires consideration of several important clinical features: 1. age of the patient 2. size of the nodes 3. location of the nodes 4. quality of the nodes 5. localized vs generalized 6. time course of the lymphadenopathy 7. associated symptoms (including worrisome features) Important considerations 1) Patient age Lymph nodes generally are not palpable in newborns Congenital lesions can mimic lymphadenopathy - cystic hygroma - branchial cleft cysts - thyroglossal duct - Congenital cervical rib Cystic hygroma Branchial cleft cysts Thyroglossal duct Important considerations • Cont, Patient age DDXs of lymphadenopathy changes according to the age e.g. cervical or supraclavicular lymph node enlargement > 10 yrs of age consider Hodgkin’s lymphoma < 10 yrs of age Rx and observe Sexually transmitted disease (late adolescence and adulthood) Important considerations 2) Size of lymph nodes normal VS pathological tend to be larger in young children (frequent Antigenic exposure) the risk of underlying malignancy increases with increasing size of lymph node ( > 2 cm is concerning in older children) Important considerations 3) Location of lymph node Important in formulating your DDxs e.g. axillary (cat scratch disease) Supraclavicular lymph node enlargement warrants carful evaluation Inguinal and axillary lymph nodes are less worrisome Important considerations 4) Quality of lymph nodes signs of inflammation (infectious) occasionally, malignancy can cause node tenderness (hemorrhage into the node) soft, easily compressible and free mobile (usually benign) hard, firm lymph nodes (malignancy) malted lymph nodes (TB, sarcoidosis) Important considerations 5) Localized VS generalized localized lymphadenopathy is more common in a primary care practice than generalized lymphadenopathy most common sites for localized lymphadenopathy involved cervical lymph nodes, followed by inguinal nodes Causes of generalized lymphadenopathy Causes of generalized lymphadenopathy Causes of generalized lymphadenopathy Causes of generalized lymphadenopathy Causes of generalized lymphadenopathy Causes of generalized lymphadenopathy Important considerations 6) Time course of lymphadenopathy acute VS subacute VS chronic response to antibiotic trial progression of lymph node - if > 4 – 6 weeks review your DDx - if > 6 – 12 weeks consider urgent referral lymph nodes that have been present for a very long duration in a well pt are not likely to be malignant (except Hodgkin disease) Important considerations 7) Worrisome features Soldes and colleagues identified most common predictors for malignancy which include 1. larger nodes > 2 cm 2. more than 2 sites of adenopathy 3. older age > 12 yrs (malignant) > 8 yrs (benign) 4. supraclavicular lymphadenopathy Important considerations • Cont. 5. adenopathy in CXR 6. blast cells in peripheral smears • other important features wt loss (> 10 % of wt) abnormal 2 cell lines in CBC prolonged or intermittent unexplained fever. soldes OS,Younger JG,Hirschi RB. Predictors of malignancy in childhood peripheral lymphadenopathy. J pediatr surgery.1999,34:1447-1452 Work up • Initial work up: - CBC (diff) - peripheral smear - CRP, ESR, LDH, uric acid - LFT, Renal functions - CXR Work up • Specific tests - Throat c/s - viral studies (EBV, CMV) - B.henselae titres - PPD - Autoimmune work up (ANA, Ds DNA) - U/S Work up • Invasive tests: BMA lymph node biopsy (excisional type preferred) biopsy of rash (if present) Approach for Generalized LAD Approach for Cervical LAD Approach to axillary LAD Approach to inguinal LAD Home message • History and physical exam alone are very important in triage of patients with lymphadenopathy • Minimal laboratory and radiologic studies can help identify other important risk factors • Consider referral in any patient with unexplained lymphadenopathy > 6 weeks • Always remember red flags of lymphadenopathy References • 1- Up to date . • 2- Nelson Textbook of pediatrics 19th Edition (2011) . • 3- Red Book 29th Edition ( 2012). • 4- pediatrics In Review 2008; 29;53 56- 7- DOI 10.1542/pir.29-2-53 Medscape Reference ( May 2012) Current pediatrics Diagnosis and treatment 21th Ediation ( 2012). Zetelli Atlas of Pediatric Physical& Diagnosis 6th Edition ( 2012) Questions??