Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Cardiac surgery wikipedia , lookup
Heart failure wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Electrocardiography wikipedia , lookup
Coronary artery disease wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
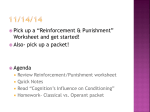
Anisotropic Reinforcement of Acute Anteroapical Infarcts Improves Pump Function Gregory M. Fomovsky, PhD; Samantha A. Clark, BS; Katherine M. Parker, MS; Gorav Ailawadi, MD; Jeffrey W. Holmes, MD, PhD Downloaded from http://circheartfailure.ahajournals.org/ by guest on May 10, 2017 Background—We hypothesize that a therapy that improves left ventricular (LV) pump function early after infarction should decrease the need for compensation through sympathetic activation and dilation, thereby reducing the risk of developing heart failure. The mechanical properties of healing myocardial infarcts are an important determinant of LV function, yet improving function by altering infarct properties has proven unexpectedly difficult. Using a computational model, we recently predicted that stiffening a large anterior infarct anisotropically (in only one direction) would improve LV function, whereas isotropic stiffening, the focus of previous studies and therapies, would not. The goal of this study was to test the novel strategy of anisotropic infarct reinforcement. Methods and Results—We tested the effects of anisotropic infarct reinforcement in 10 open-chest dogs with large anteroapical infarcts that depressed LV pump function. We measured regional mechanics, LV volumes, and cardiac output at a range of preloads at baseline, 45 minutes after coronary ligation (ischemia), and 30 minutes later, after surgical reinforcement in the longitudinal direction (anisotropic). Ischemia shifted the end-systolic pressure–volume relationship and cardiac output curves rightward, decreasing cardiac output at matched end-diastolic pressure by 44%. Anisotropic reinforcement significantly improved systolic function without impairing diastolic function, recovering half the deficit in overall LV function. Conclusions—We conclude that anisotropic reinforcement is a promising new approach to improving LV function after a large myocardial infarction. (Circ Heart Fail. 2012;5:515-522.) Key Words: cardiac output ◼ mechanics ◼ myocardial infarction ◼ surgery E ach year, over one million Americans experience a myocardial infarction (MI).1 Despite current therapies, the risk of developing heart failure after MI remains substantial, particularly for older patients and those with reduced left ventricular (LV) function.1,2 After infarction, the mechanical properties of healing myocardial infarcts are a critical determinant of both depression of pump function and LV remodeling,3 suggesting that it might be possible to improve pump function and/or reduce adverse postinfarction remodeling by manipulating infarct mechanical properties. Depressed pump function and LV dilation both contribute to the development of heart failure after infarction. Therefore, improving pump function and limiting LV dilation are both important therapeutic goals. These 2 effects are easily confused in studies that rely on ejection fraction as the primary indicator of function, because reducing LV volumes increases ejection fraction even if stroke volume does not change. By contrast, studies that report cardiac output curves over a range of filling pressures can separate effects on dilation and pump function. Polymer injection, surgical reinforcement, and computational modeling studies that report cardiac output curves consistently show that these approaches reduce or limit LV dilation and subsequent functional deterioration but do not improve LV pump function acutely.7,15,20,21 We therefore sought to develop a complementary therapeutic approach that could improve LV pump function early after a large MI. Normal myocardium deforms in a complex 3-dimensional pattern with each heartbeat,22–24 and healing myocardial infarcts can be highly anisotropic (having different mechan ical properties in different directions).25,26 By contrast, current strategies for therapeutically modifying infarct mechanical Clinical Perspective on p 522 In fact, several novel postinfarction therapies that work at least in part by modifying infarct mechanics are now in development. Injecting polymers into the infarct has been reported to improve heart function and/or reduce remodeling,4–7 as have altering metalloproteinase activity pharmacologically8–12 or through electric stimulation,13 application of surgical devices and meshes originally designed to arrest dilation in patients with advanced heart failure,14–16 and periinfarct pacing.17–19 Received September 23, 2011; accepted May 15, 2012. From the Departments of Biomedical Engineering (G.M.F., S.A.C., K.M.P., G.A., J.W.H.), Medicine (J.W.H.), and Surgery (G.A.) and the Robert M. Berne Cardiovascular Research Center (J.W.H.), University of Virginia, Charlottesville, VA. Correspondence to Jeffrey W. Holmes, MD, PhD, Associate Professor of Biomedical Engineering and Medicine, Box 800759, Health System, University of Virginia, Charlottesville, VA 22908. E-mail [email protected] © 2012 American Heart Association, Inc. Circ Heart Fail is available at http://circheartfailure.ahajournals.org 515 DOI: 10.1161/CIRCHEARTFAILURE.111.965731 516 Circ Heart Fail July 2012 properties provide isotropic reinforcement. We recently reported that selectively increasing infarct stiffness in the longitudinal direction improved predicted pump function in a computational model of a canine heart with a large anteroapical infarct, whereas isotropic or circumferential reinforcement did not.27 In the present study, we tested this prediction experimentally in 10 dogs with large, acute anteroapical infarcts and significant depression of pump function by surgically reinforcing the infarct region in the longitudinal direction. Methods Surgical Preparation and Instrumentation Downloaded from http://circheartfailure.ahajournals.org/ by guest on May 10, 2017 This study was approved by the University of Virginia Animal Care and Use Committee. Twenty-two adult mongrel dogs of both sexes (Covance Research Products, Denver, PA; body weight 23.3±3.6 kg) were anesthetized with sodium pentobarbital (30 mg/kg intravenous induction, 5 mg/kg-hr maintenance), intubated, and ventilated with room air. A heating pad was used to maintain constant body temperature. A left thoracotomy was performed at the fifth intercostal space, the pericardium was opened, and the heart suspended in a pericardial cradle. A snare made of cloth umbilical tape was placed around the inferior vena cava (IVC) to facilitate temporary IVC occlusion. The left anterior descending artery (LAD) was isolated and ligation suture was placed distal to the first diagonal. A Millar pressure catheter (Mikro-Tip SPC-454D; Millar Instruments, Houston, TX) was inserted through the left carotid artery to measure left ventricular pressure. A catheter in the femoral artery was connected to a fluid-filled Gould manometer to monitor arterial pressure. An ultrasonic flow probe (A20; Transonic Systems, Ithaca, NY) was placed around the ascending aorta to measure left ventricular stroke volume (SV). Ten sonomicrometer crystals (2T-36S-40-RS; Sonometrics, London, Ontario, Canada) were inserted into the LV midwall using a metal introducer. Six crystals were used to measure changes in the 3 axes of the LV (Figure 1A): anteroposterior, septal– lateral, and base-apex (BA). Four additional crystals were placed in the anterior LV wall, in the region supplied by the LAD, to measure regional strains. Experimental Protocol After instrumentation, 2 mg/kg propranolol and 0.2 mg/kg atropine were administered to minimize reflex changes in heart rate and intrinsic myocardial contractility.28 Blockade was confirmed by test injection of 2.5 μg/kg dobutamine. Baseline data were then recorded while preload was varied by temporary IVC occlusion (baseline). The LAD was ligated between the first and second diagonal branches; arteries providing collateral flow to the lower two thirds of the anterior wall were also ligated as needed to produce a large, dyskinetic ischemic region. Lidocaine (10 mg intravenously) was administered in 11 animals to control arrhythmias and defibrillation was required in 7. Hemodynamic and sonomicrometry data were recorded every 5 minutes after LAD occlusion. Forty-five minutes after LAD ligation, acute ischemia data were recorded during IVC occlusion (ischemia). Immediately after the ischemia recording, the ischemic region was anisotropically reinforced by sewing a modified Dacron patch (Hemashield Knitted Double Velour Fabric; Maquet Cardiovascular LLC, Wayne, NJ) onto the epicardial surface of the heart over the ischemic area (Figure 1). The patches, typically used for LV aneurysm resection and repair,29 were modified by creating longitudinally oriented slits that allowed virtually unrestricted circumferential deformation in ex vivo mechanical tests and were sewn to the epicardial surface under as much longitudinal tension as the surgeon felt could be applied without risking tearing of the sutures from the myocardium; this resulted in a remarkably consistent 11.4%±2.9% reduction in longitudinal segment lengths in the center of the infarct. After reinforcement, data were again acquired during IVC occlusion (anisotropic, acquired 30.7±7.3 minutes after ischemia). At the end Figure 1. A, Diagram of sonomicrometer and patch placement; see text for details. B, Photograph of a modified Dacron patched sewed to the epicardial surface of the left ventricle. Black line on patch is aligned with the long axis of the LV; LAD occluder is visible near left edge of photograph. LV indicates left ventricle; LAD, left anterior descending artery. of the experiment, animals were euthanized with an overdose of pentobarbital and hearts were excised for confirmation and imaging of sonomicrometer placement. Data Analysis Hemodynamic data were processed using the Sonometrics software, SonoSoft, and custom Matlab software. To assess the state of LV function at each experimental condition, measurements were averaged over 3 to 5 cardiac cycles at constant preload. To analyze the response of the LV to preload changes, cycles covering the full range of pressure variation during IVC occlusion were analyzed and the resulting parameters fitted to obtain end-diastolic (EDPVR) and endsystolic (ESPVR) pressure–volume relationships as well as cardiac output curves. For each cardiac cycle, end-diastole was defined as the point immediately before the sharp increase in LV pressure and end-systole was identified as the point of maximal elastance.30 LV volumes were computed from anteroposterior, septal–lateral, and BA axis lengths, assuming a truncated ellipsoidal geometry.30 Because sonomicrometers were located in the LV midwall, these volumes included both cavity volume and approximately half the LV wall volume, which is essentially constant over the cardiac cycle. Stroke volume was computed by integrating the ascending aorta flow signal as described and validated by Steingart, neglecting retrograde (coronary) flow.31 At baseline, SVs computed by subtracting sonomicrometer-derived EDV and ESV values (SVsono) agreed with SV computed by integrating the ascending aorta flow signal (SVflow). During ischemia, SVsono was less accurate due to systolic bulging of the ischemic region. Therefore, we report here only SVflow and compute ESV as EDV−SVflow. Fomovsky et al Anisotropic Infarcts Reinforcement 517 Downloaded from http://circheartfailure.ahajournals.org/ by guest on May 10, 2017 ESPVR, EDPVR, and cardiac output curves for each condition were fitted and used to interpolate data for comparison at matched pressures. The linear ESPVR was obtained by fitting a straight line to ESP versus ESV data (mean±SD R2 for fits to data from individual animals=0.78±0.23), the exponential EDPVR and cardiac output (CO) curves by fitting a straight line to ln(EDP) versus EDV or CO data (R2 0.90±0.09 for EDPVR, 0.88±0.12 for CO curve). Interpolated volume and cardiac output values at matched pressures were also averaged to construct mean EDPVR, ESPVR, and CO curves. To assess changes in LV shape, we fitted ln(EDP) versus end-diastole segment length curves and compared interpolated BA, anteroposterior, and septal–lateral dimensions at matched pressures. Regional strains were computed from ≥3 segment lengths measured by the 4 sonomicrometers in the center of the ischemic region. Postmortem photographs were used to construct unit vectors describing the orientation of each crystal pair relative to the short axis of the LV. Real-time segment lengths were used to compute 2-dimensional systolic regional strains reflecting circumferential shortening/stretching, longitudinal shortening/stretching, and shearing in the anterior midwall from end diastole to end systole.32 Segment lengths interpolated at matched pressures from linear fits of ln(EDP) versus end-diastole segment length data were used to compute remodeling strains reflecting changes in enddiastolic configuration across different states (baseline, ischemia, anisotropic). Statistical Analysis The goal of this study was to test the model prediction that longitudinal reinforcement can mitigate acute depression of pump function after a large anteroapical infarction. Because this hypothesis can only be tested if pump function is depressed, we used depression of pump function as reflected by a rightward shift in the ischemia CO curve as an inclusion criterion for this study. Dogs with no shift in CO curve during ischemia were excluded from further analysis. In the remaining animals, parameters with independent numeric values at each state (baseline, ischemia, anisotropic) were analyzed by one-way repeated-measures analysis of variance with Newman-Keuls post hoc comparisons when the analysis of variance showed significant variation among the groups. For parameters that were zero at baseline by definition such as remodeling strains and changes in volumes, we tested the effect of ischemia using a one-sample t test against a hypothetical mean of zero and the effect of anisotropic reinforcement by paired 2-tailed t test of anisotropic versus ischemia data. A probability value <0.05 was used as the threshold for statistical significance for all tests. Results A total of 22 dogs underwent LAD ligation for this study. Of these, 10 animals showed a shift in the ventricular function curve (CO versus end-diastolic pressure) 45 minutes after LAD ligation and were included in the study. Of the remaining 12 animals, 3 died of ventricular fibrillation after LAD ligation, 8 showed no shift in the ventricular function curve after LAD ligation, and one was excluded due to failure of the data acquisition system during the study. Hemodynamics Heart rate and maximum dP/dt did not vary during the study, demonstrating effective blockade of sympathetic and parasympathetic reflex changes (Table). Because the animals were unable to compensate for reduced pump function by increasing heart rate or intrinsic contractility, they relied on the Frank-Starling mechanism, maintaining SV and CO by significantly increasing EDP and EDV. Table. Hemodynamic Parameters Parameter Baseline Ischemia Anisotropic EDP, mm Hg 11.3±4.3 17.3±6.1† 15.9±7.5 EDV,* mL 78.2±15.5 89.0±18.0† 82.2±16.2‡ ESP, mm Hg 96.1±14.8 94.7±14.3 92.2±9.7 ESV,* mL 62.7±13.5 75.0±17.7† 66.9±15.4‡ SV, mL 15.5±3.8 14.0±3.9 15.4±3.5 HR, beats/min 108±10 109±15 111±15 CO, L/min 1.69±0.51 1.54±0.54 1.70±0.44 Maximum dP/dt, mm|Hg/s 1227±337 1220±431 1342±249 Hemodynamic data from 10 dogs that showed a shift in cardiac output curve 45 min after coronary ligation. Dogs were pretreated with propranolol and atropine to prevent reflex changes in heart rate and intrinsic myocardial contractility; by design, end-systolic pressure (ESP), heart rate (HR), and maximum dP/dt did not vary significantly during the experiment. During ischemia, animals compensated for reduced systolic function through the Frank-Starling mechanism, increasing end-diastolic pressure (EDP) and volume (EDV) to maintain stroke volume (SV) and cardiac output (CO) despite increased end-systolic volume (ESV). Anisotropic surgical reinforcement significantly reduced EDV and ESV. *Midwall volumes include cavity volume and approximately half the left ventricular wall volume. †P<0.001 versus baseline. ‡P<0.001 versus ischemia. Mechanics of Acute Ischemia and Anisotropic Reinforcement Figure 2 illustrates the impact of ischemia and anisotropic reinforcement on regional and global function in a single animal. At baseline, pressure-segment length loops indicated active contraction in the anterior wall (Figure 2A–B). Hemodynamic data acquired during IVC occlusion produced the expected exponential EDPVR, linear end-ESPVR, and relatively steep working portion of the CO curve (Figure 2C–D). Forty-five minutes after LAD ligation, pressure-segment loops indicated passive lengthening rather than active contraction, the ESPVR was shifted rightward, and the ventricular function curve was shifted down and to the right with a >50% reduction in cardiac output at matched EDP. Anisotropic surgical reinforcement selectively reduced longitudinal segment lengths (Figure 2A), shifted the ESPVR back to the left without affecting the EDPVR, and reversed approximately half the shift in the CO curve. Effect of Anisotropic Reinforcement on Regional Mechanics and LV Shape Remodeling strains in the center of the ischemic region showed increased circumferential and longitudinal dimensions at a matched EDP of 12 mm Hg during ischemia compared with baseline (Figure 3A). Anisotropic reinforcement reversed longitudinal remodeling (P<0.001 versus ischemia) and modestly reduced circumferential remodeling (P<0.01). Systolic strains were negative at baseline, indicating circumferential and longitudinal shortening during contraction (Figure 3B). Acute ischemia abolished shortening in both directions (P<0.001 versus baseline), and anisotropic reinforcement slightly increased systolic circumferential stretching without affecting longitudinal strain. Globally, ischemia increased the BA dimension significantly 518 Circ Heart Fail July 2012 Downloaded from http://circheartfailure.ahajournals.org/ by guest on May 10, 2017 Figure 2. Effect of ischemia and anisotropic reinforcement in a single animal. A, B, Infarct region pressure-segment length data. At baseline (black), loops indicated active contraction in both the longitudinal (A) and circumferential (B) directions. During ischemia, both segments demonstrated passive stretch and recoil along a single curve. Anisotropic reinforcement reduced longitudinal segment length throughout the cardiac cycle. C, Ischemia shifted the end-systolic pressure-volume relationship (ESPVR, closed symbols) rightward and anisotropic reinforcement returned ESPVR toward baseline with little effect on the end-diastolic relationship (EDPVR, open symbols). Note that volumes are midwall volumes, including both cavity volume and approximately half the LV wall volume. D, Cardiac output curves shifted down and to the right with ischemia and returned toward baseline with anisotropic reinforcement. LV indicates left ventricular. (Figure 3C) but did not induce significant changes in either short-axis dimension, whereas anisotropic reinforcement restored BA length to baseline and increased the septal– lateral dimension. Effect of Anisotropic Reinforcement on Systolic and Diastolic Function Mean EDPVR and ESPVR curves showed clearly that ischemia shifted the ESPVR rightward and anisotropic reinforcement partially reversed this shift with little effect on the EDPVR (Figure 4A). We quantified shifts in pressure– volume behavior using volumes interpolated from individual ESPVR and EDPVR curves at identical pressures for all animals. As expected from the average curves, end-systolic volume at a pressure of 85 mm Hg (ESV85) increased significantly with ischemia (Figure 4B), whereas end-diastolic volume at a pressure of 12 mm Hg (EDV12) did not change. Figure 3. Effect of ischemia and anisotropic reinforcement on regional strains and LV dimensions. A, Remodeling strains indicating changes in enddiastolic dimensions at a matched EDP of 12 mm Hg are zero at baseline by definition. Ischemia increased both circumferential and longitudinal dimensions relative to baseline, whereas anisotropic reinforcement dramatically reduced longitudinal remodeling. B, Systolic strains indicating deformation from end diastole to end-systole are negative at baseline, indicating systolic shortening, and positive during ischemia, indicating systolic stretching. C, Ischemia increased average base-apex (BA) dimensions at a matched end-diastolic pressure of 12 mm|Hg without significantly affecting anteroposterior (AP) or septal–lateral (SL) dimensions. Anisotropic reinforcement restored BA to baseline and significantly increased SL. *P<0.05 for comparison indicated. LV indicates left ventricular; EDP, end-diastolic pressure. Fomovsky et al Anisotropic Infarcts Reinforcement 519 Downloaded from http://circheartfailure.ahajournals.org/ by guest on May 10, 2017 Figure 4. Effect of ischemia and anisotropic reinforcement on average pressure–volume curves. A, Ischemia shifted the endsystolic pressure–volume relationship (ESPVR, closed symbols) rightward and anisotropic reinforcement returned ESPVR toward baseline with little effect on the end-diastolic relationship (EDPVR, open symbols). B, Comparing volumes interpolated at matched pressures (dashed lines in A) showed no change in enddiastolic volume at 12 mm|Hg (EDV12) but a significant increase in end-systolic volume at 85 mm|Hg (EDV85) with ischemia and significant reduction of EDV85 with anisotropic reinforcement. Note that volumes are midwall volumes, including both cavity volume and approximately half the LV wall volume. *P<0.05 for comparison indicated. LV indicates left ventricular. Anisotropic reinforcement recovered more than half of the change in ESV85 (P<0.01 versus ischemia) without affecting EDV12. Effect of Anisotropic Reinforcement on Pump Function A shift in CO curve during ischemia was an inclusion criterion for this study. Comparing the mean baseline and ischemia curves, average CO at a matched EDP of 12 mm Hg dropped 44%, and a 50% increase in EDP to 18 mm Hg would have been required to return to baseline CO (Figure 5A). Using the baseline EDP in each individual animal and interpolating to find CO at matched pressures in the other states confirmed a significant reduction in CO with ischemia (P<0.01; Figure 5. Effect of ischemia and anisotropic reinforcement on average cardiac output curves. A, Cardiac output curves shifted down and to the right with ischemia and returned toward baseline with anisotropic reinforcement. B, Comparing cardiac output interpolated at matched end-diastolic pressures (baseline EDP) in each animal showed a significant drop in cardiac output with ischemia and recovery of 50% of the deficit with anisotropic reinforcement. *P<0.05 for comparison indicated. Figure 5B). Anisotropic reinforcement recovered more than half the deficit in CO (P<0.05). Discussion Acute myocardial infarcts stretch and bulge during systole, wasting contractile energy expended by remaining noninfarcted myocardium and reducing overall pump function. The changes are reflected in a rightward shift in both the ESPVR and CO curve (Figures 4 and 5); for any level of preload, the heart is able to generate less pressure and eject less SV. Intuition suggests that stiffening these acute infarcts should reduce systolic stretching of the infarct and improve function, yet computational modeling and experimental studies have consistently shown that although a stiffer infarct improves systolic function, it also impairs diastolic function, shifting not only the ESPVR, but also the EDPVR to the left. The systolic and diastolic effects offset, producing no net improvement in LV function.15,20,21,33 Until recently, such studies considered only isotropic stiffening (increasing the stiffness equally in all directions). However, the complex 3-dimensional nature of deformation in the heart wall22–24 and the fact that healing myocardial infarcts can be highly anisotropic in some animal models25,26 led us to consider whether anisotropic stiffening or reinforcement 520 Circ Heart Fail July 2012 Downloaded from http://circheartfailure.ahajournals.org/ by guest on May 10, 2017 might be a better strategy. We used a computational model to ask what infarct mechanical properties would provide the best pump function after a large anterior infarction and found that the combination of high stiffness in the longitudinal direction and low stiffness in the circumferential direction provided the best predicted function.27 Infarct anisotropy appeared to circumvent the tradeoff between systolic and diastolic function, improving systolic function with little impact on diastolic function. In the present study, we tested this model prediction by surgically reinforcing acute anteroapical infarcts in dogs with postinfarction depression of LV pump function. We found that anisotropic reinforcement in these animals did in fact improve systolic function with little effect on filling, recovering half of the deficit in the CO curve associated with acute ischemia. We conclude that anisotropic reinforcement is a novel and promising approach to improving LV function after a large MI. Effects of Anisotropic Reinforcement Globally, anisotropic reinforcement improved systolic function without impairing diastolic filling. Circumferential systolic stretching in the infarct actually increased after reinforcement, suggesting that simply reducing systolic dyskinesis is not the primary mechanism for improved systolic function. Rather, our prior modeling study and current data suggest that anisotropic reinforcement reshapes the heart at ED. Comparing remodeling strains and global dimensions at matched EDP (Figures 3A and 3C), we found that ischemia not only induced acute circumferential and longitudinal expansion of the infarct, but also increased the BA dimension of the LV significantly. Anisotropic reinforcement reversed longitudinal expansion in the infarct and returned BA to baseline. Because reinforcement restricted longitudinal expansion during diastole but did not reduce diastolic volumes, we would expect increased stretching along at least one other axis, and we in fact saw a significant increase in the end-diastolic septal–lateral dimension after patch application. Therefore, anisotropic reinforcement may increase preload in circumferentially oriented remote myocardium. Additional studies are clearly required to better understand the impact of anisotropic reinforcement on border and remote myocardium as well as transmural variations in regional strains after reinforcement (this study measured midwall strains). Therapeutic Options After MI After a large MI, sympathetic activation increases myocardial contractility and heart rate, and elevated filling pressures increase diastolic volume and sarcomeric prestretch, enhancing contraction through the Frank-Starling mechanism. Although sympathetic activation and LV dilation help preserve CO acutely, they are also the initial steps in the pathogenesis of heart failure. Standard postinfarction therapy therefore includes β-blockers to counteract detrimental effects of chronic sympathetic activation and angiotension-converting enzyme inhibitors to slow LV remodeling.34 However, standard therapy tends to delay rather than prevent the development of failure, particularly in patients with large infarcts, and the prognosis for patients with heart failure is bleak.35 Several groups have therefore explored more aggressive approaches to preventing LV dilation, applying therapies originally developed for heart failure immediately after infarction to prevent LV dilation and functional deterioration rather than waiting to address them until they occur. Gorman and colleagues36 showed that early application of cardiac support devices limits dilation and functional deterioration. Several groups reported similar results with early postinfarction injection of polymers.4–7 Shuros et al19 adapted biventricular pacing, originally developed for heart failure, to a strategy termed “peri-infarct pacing” for use early after MI. By pre-exciting the border zone to reduce regional stroke work, they were able to attenuate postinfarction LV remodeling. Smalling and colleagues37,38 have even explored the potential of LV unloading with LV assist devices and aortic balloon pumps during initial reperfusion to decrease infarct size. These efforts all seek to limit LV dilation and remodeling earlier in the course of postinfarction healing but do not provide immediate improvements in LV pump function. We sought to develop a complementary strategy for improving LV function early after infarction. We hypothesize that a therapy that improves LV pump function early after infarction should decrease the need for compensation through sympathetic activation and dilation, thereby reducing the risk of developing heart failure. The present study is exciting as a proof-of-concept that it is possible to improve LV pump function immediately after infarction by appropriately manipulating infarct mechanical properties. Chronic studies are required to determine whether this acute improvement in pump function will in fact reduce long-term dilation and development of heart failure. Our approach shares the goal of improving LV pump function early after infarction with regenerative approaches such as stem cell injection that aim to restore functioning muscle to the infarct region. However, much of the remodeling that predisposes to heart failure occurs in the first few days, whereas most regenerative approaches will require weeks to fully implement. We therefore propose that mechanical reinforcement early after infarction has significant potential not only as a standalone therapy, but also as an adjunct to regenerative approaches. Limitations The goal of this study was to test the hypothesis that longitudinal reinforcement can improve depressed pump function acutely in dogs with large anteroapical infarcts. Because sympathetic activation can temporarily compensate for depressed pump function early after MI, we used pharmacological blockade to prevent changes in heart rate and intrinsic myocardial contractility.28 This approach allowed us to recognize and quantify changes in pump function through shifts in the cardiac output curve; it also facilitated comparisons with computational models, which typically hold intrinsic myocardial contractility and heart rate constant. However, additional studies are clearly required to test our hypothesis that anisotropic reinforcement will alter postinfarction sympathetic activation and remodeling when neurohumoral reflexes are intact. Fomovsky et al Anisotropic Infarcts Reinforcement 521 Downloaded from http://circheartfailure.ahajournals.org/ by guest on May 10, 2017 Computational and experimental studies have consistently found that isotropic infarct reinforcement or stiffening does not improve LV function acutely,7,15,20,21 whereas our data show that anisotropic reinforcement does improve LV function acutely in this animal model. We did not compare isotropic against anisotropic reinforcement in this study; additional studies would be needed to test definitively whether anisotropic reinforcement improves acute LV function more than isotropic reinforcement. In addition, for this proof-of-concept study, we reinforced the infarct by sewing a modified Dacron patch to the epicardial surface. Clinically, sewing a modified or specially manufactured patch to the epicardial surface could be feasible in the subset of patients who undergo surgical revascularization early after infarction, but developing a minimally invasive approach to anisotropic reinforcement would extend its potential use to a much larger patient population. Approximately one third of the animals entering this study were excluded because there was no evidence of altered pump function after infarction. Some of this variability among animals was likely due to variations in infarct size. Ligating the same artery in the same place can produce a wide range of infarct sizes in different dogs due to an extensive and variable network of coronary collaterals. Although we ligated collaterals where apparent, it is likely that infarct size varied substantially among animals and that animals with small infarcts showed less depression of pump function. In addition, although changes in other hemodynamic parameters with ischemia were similar between the included and excluded groups, dP/dt increased significantly only in the excluded group, suggesting that pharmacological blockade might have been incomplete in some of these animals. Conclusions In summary, we tested the model prediction that longitudinal reinforcement of acute canine anteroapical infarcts can acutely improve depressed LV pump function. Anisotropic reinforcement improved systolic function without impairing filling, restoring half the deficit in the CO curve associated with acute ischemia. We conclude that anisotropic reinforcement is a novel and promising approach to improving LV function after a large MI. The next step in the development of this potential therapy is to conduct chronic animal studies to evaluate the impact of anisotropic reinforcement on LV function, remodeling, and the development of heart failure. Acknowledgments We acknowledge the surgical assistance of N. Craig Goodman. Sources of Funding Supported by the University of Virginia Coulter Translational Research Program (G.A., J.W.H.) and National Institutes of Health/ National Heart, Lung and Blood Institute R01 HL-075639 (J.W.H.). Disclosures None. References 1. Lloyd-Jones D, Adams RJ, Brown TM, Carnethon M, Dai S, De Simone G, Ferguson TB, Ford E, Furie K, Gillespie C, Go A, Greenlund K, Haase N, Hailpern S, Ho PM, Howard V, Kissela B, Kittner S, Lackland D, Lisabeth L, Marelli A, McDermott MM, Meigs J, Mozaffarian D, Mussolino M, Nichol G, Roger VL, Rosamond W, Sacco R, Sorlie P, Thom T, Wasserthiel-Smoller S, Wong ND, Wylie-Rosett J. Heart disease and stroke statistics—2010 update: a report from the American Heart Association. Circulation. 2010;121:e46–e215. 2. Lewis EF, Moye LA, Rouleau JL, Sacks FM, Arnold JM, Warnica JW, Flaker GC, Braunwald E, Pfeffer MA. Predictors of late development of heart failure in stable survivors of myocardial infarction: the CARE study. J Am Coll Cardiol. 2003;42:1446–1453. 3. Holmes JW, Borg TK, Covell JW. Structure and mechanics of healing myocardial infarcts. Annu Rev Biomed Eng. 2005;7:223–253. 4. Christman KL, Fok HH, Sievers RE, Fang Q, Lee RJ. Fibrin glue alone and skeletal myoblasts in a fibrin scaffold preserve cardiac function after myocardial infarction. Tissue Eng. 2004;10:403–409. 5. Dai W, Wold LE, Dow JS, Kloner RA. Thickening of the infarcted wall by collagen injection improves left ventricular function in rats: a novel approach to preserve cardiac function after myocardial infarction. J Am Coll Cardiol. 2005;46:714–719. 6. Mukherjee R, Zavadzkas JA, Saunders SM, McLean JE, Jeffords LB, Beck C, Stroud RE, Leone AM, Koval CN, Rivers WT, Basu S, Sheehy A, Michal G, Spinale FG. Targeted myocardial microinjections of a biocomposite material reduces infarct expansion in pigs. Ann Thorac Surg. 2008;86:1268–1276. 7. Ryan LP, Matsuzaki K, Noma M, Jackson BM, Eperjesi TJ, Plappert TJ, St John-Sutton MG, Gorman JH III, Gorman RC. Dermal filler injection: a novel approach for limiting infarct expansion. Ann Thorac Surg. 2009;87:148–155. 8. Hudson MP, Armstrong PW, Ruzyllo W, Brum J, Cusmano L, Krzeski P, Lyon R, Quinones M, Theroux P, Sydlowski D, Kim HE, Garcia MJ, Jaber WA, Weaver WD. Effects of selective matrix metalloproteinase inhibitor (PG-116800) to prevent ventricular remodeling after myocardial infarction: results of the PREMIER (Prevention of Myocardial Infarction Early Remodeling) trial. J Am Coll Cardiol. 2006;48:15–20. 9.Lindsey ML, Gannon J, Aikawa M, Schoen FJ, Rabkin E, LoprestiMorrow L, Crawford J, Black S, Libby P, Mitchell PG, Lee RT. Selective matrix metalloproteinase inhibition reduces left ventricular remodeling but does not inhibit angiogenesis after myocardial infarction. Circulation. 2002;105:753–758. 10.Rohde LE, Ducharme A, Arroyo LH, Aikawa M, Sukhova GH, Lopez-Anaya A, McClure KF, Mitchell PG, Libby P, Lee RT. Matrix metalloproteinase inhibition attenuates early left ventricular enlargement after experimental myocardial infarction in mice. Circulation. 1999;99:3063–3070. 11. Villarreal FJ, Griffin M, Omens J, Dillmann W, Nguyen J, Covell J. Early short-term treatment with doxycycline modulates postinfarction left ventricular remodeling. Circulation. 2003;108:1487–1492. 12.Yarbrough WM, Mukherjee R, Brinsa TA, Dowdy KB, Scott AA, Escobar GP, Joffs C, Lucas DG, Crawford FA Jr, Spinale FG. Matrix metalloproteinase inhibition modifies left ventricular remodeling after myocardial infarction in pigs. J Thorac Cardiovasc Surg. 2003;125: 602–610. 13. Mukherjee R, Rivers WT, Ruddy JM, Matthews RG, Koval CN, Plyler RA, Chang EI, Patel RK, Kern CB, Stroud RE, Spinale FG. Long-term localized high-frequency electric stimulation within the myocardial infarct: effects on matrix metalloproteinases and regional remodeling. Circulation. 2010;122:20–32. 14.Enomoto Y, Gorman JH III, Moainie SL, Jackson BM, Parish LM, Plappert T, Zeeshan A, St John-Sutton MG, Gorman RC. Early ventricular restraint after myocardial infarction: extent of the wrap determines the outcome of remodeling. Ann Thorac Surg. 2005; 79:881–887; discussion 881–887. 15. Kelley ST, Malekan R, Gorman JH III, Jackson BM, Gorman RC, Suzuki Y, Plappert T, Bogen DK, Sutton MG, Edmunds LH Jr. Restraining infarct expansion preserves left ventricular geometry and function after acute anteroapical infarction. Circulation. 1999;99:135–142. 16. Liao SY, Siu CW, Liu Y, Zhang Y, Chan WS, Wu EX, Wu Y, Nicholls JM, Li RA, Benser ME, Rosenberg SP, Park E, Lau CP, Tse HF. Attenuation of left ventricular adverse remodeling with epicardial patching after myocardial infarction. J Card Fail. 2010;16:590–598. 17. Chung ES, Dan D, Solomon SD, Bank AJ, Pastore J, Iyer A, Berger RD, Franklin JO, Jones G, Machado C, Stolen CM. Effect of peri-infarct pacing early after myocardial infarction: results of the prevention of myocardial enlargement and dilatation post myocardial infarction study. Circ Heart Fail. 2010;3:650–658. 522 Circ Heart Fail July 2012 Downloaded from http://circheartfailure.ahajournals.org/ by guest on May 10, 2017 18.Chung ES, Menon SG, Weiss R, Schloss EJ, Chow T, Kereiakes DJ, Mazur W, Salo RW, Galle E, Pastore JM. Feasibility of biventricular pacing in patients with recent myocardial infarction: impact on ventricular remodeling. Congest Heart Fail. 2007;13:9–15. 19.Shuros AC, Salo RW, Florea VG, Pastore J, Kuskowski MA, Chandrashekhar Y, Anand IS. Ventricular preexcitation modulates strain and attenuates cardiac remodeling in a swine model of myocardial infarction. Circulation. 2007;116:1162–1169. 20.Bogen DK, Rabinowitz SA, Needleman A, McMahon TA, Abelmann WH. An analysis of the mechanical disadvantage of myocardial infarction in the canine left ventricle. Circ Res. 1980;47:728–741. 21. Wall ST, Walker JC, Healy KE, Ratcliffe MB, Guccione JM. Theoretical impact of the injection of material into the myocardium: a finite element model simulation. Circulation. 2006;114:2627–2635. 22. Arts T, Costa KD, Covell JW, McCulloch AD. Relating myocardial laminar architecture to shear strain and muscle fiber orientation. Am J Physiol Heart Circ Physiol. 2001;280:H2222–2229. 23. Costa KD, Takayama Y, McCulloch AD, Covell JW. Laminar fiber architecture and three-dimensional systolic mechanics in canine ventricular myocardium. Am J Physiol. 1999;276:H595–607. 24. Takayama Y, Costa KD, Covell JW. Contribution of laminar myofiber architecture to load-dependent changes in mechanics of LV myocardium. Am J Physiol Heart Circ Physiol. 2002;282:H1510–1520. 25.Gupta KB, Ratcliffe MB, Fallert MA, Edmunds LH Jr, Bogen DK. Changes in passive mechanical stiffness of myocardial tissue with aneurysm formation. Circulation. 1994;89:2315–2326. 26. Holmes JW, Nunez JA, Covell JW. Functional implications of myocardial scar structure. Am J Physiol Heart Circ Physiol. 1997;272:H2123–2130. 27. Fomovsky GM, Macadangdang JR, Ailawadi G, Holmes JW. Model-based design of mechanical therapies for myocardial infarction. J Cardiovasc Transl Res. 2011;4:82–91. 28. Little WC, O’Rourke RA. Effect of regional ischemia on the left ventricular end-systolic pressure–volume relation in chronically instrumented dogs. J Am Coll Cardiol. 1985;5:297–302. 29. Dor V, Sabatier M, Di Donato M, Maioli M, Toso A, Montiglio F. Late hemodynamic results after left ventricular patch repair associated with coronary grafting in patients with postinfarction akinetic or dyskinetic aneurysm of the left ventricle. J Thorac Cardiovasc Surg. 1995;110:1291– 1299; discussion 1300–1391. 30. Holmes JW. Candidate mechanical stimuli for hypertrophy during volume overload. J Appl Physiol. 2004;97:1453–1460. 31. Steingart RM, Meller J, Barovick J, Patterson R, Herman MV, Teichholz LE. Pulsed Doppler echocardiographic measurement of beat-to-beat changes in stroke volume in dogs. Circulation. 1980;62:542–548. 32.Villarreal FJ, Waldman LK, Lew WYW. Technique for measuring regional two-dimensional finite strains in canine left ventricle. Circ Res. 1988;62:711–721. 33. Janz RF, Waldron RJ. Predicted effect of chronic apical aneurysms on the passive stiffness of the human left ventricle. Circ Res. 1978;42:255–263. 34. Antman EM, Hand M, Armstrong PW, Bates ER, Green LA, Halasyamani LK, Hochman JS, Krumholz HM, Lamas GA, Mullany CJ, Pearle DL, Sloan MA, Smith SC Jr, Anbe DT, Kushner FG, Ornato JP, Jacobs AK, Adams CD, Anderson JL, Buller CE, Creager MA, Ettinger SM, Halperin JL, Hunt SA, Lytle BW, Nishimura R, Page RL, Riegel B, Tarkington LG, Yancy CW. 2007 focused update of the ACC/AHA 2004 guidelines for the management of patients with ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2008;51:210–247. 35. Lee DS, Gona P, Vasan RS, Larson MG, Benjamin EJ, Wang TJ, Tu JV, Levy D. Relation of disease pathogenesis and risk factors to heart failure with preserved or reduced ejection fraction: insights from the Framingham Heart Study of the National Heart, Lung, and Blood Institute. Circulation. 2009;119:3070–3077. 36. Gorman RC, Jackson BM, Burdick JA, Gorman JH. Infarct restraint to limit adverse ventricular remodeling. J Cardiovasc Transl Res. 2011;4:73–81. 37.Achour H, Boccalandro F, Felli P, Amirian J, Uthman M, Buja M, Smalling RW. Mechanical left ventricular unloading prior to reperfusion reduces infarct size in a canine infarction model. Catheter Cardiovasc Interv. 2005;64:182–192. 38. LeDoux JF, Tamareille S, Felli PR, Amirian J, Smalling RW. Left ventricular unloading with intra-aortic counter pulsation prior to reperfusion reduces myocardial release of endothelin-1 and decreases infarction size in a porcine ischemia–reperfusion model. Catheter Cardiovasc Interv. 2008;72:513–521. CLINICAL PERSPECTIVE After myocardial infarction, both depressed pump function and gradual dilation and remodeling of the left ventricle contribute to the development of heart failure. Although it seems logical that mechanically reinforcing the healing infarct should improve pump function, multiple studies have found that mechanical therapies such as surgical reinforcement and polymer injection can prevent dilation but do not directly improve pump function. Typically, stiffening the infarct improves systolic function but impairs filling, producing no net benefit on cardiac output. Importantly, these prior studies used methods that stiffen or reinforce the infarct similarly in all directions (isotropically). In the current study, we tested a new approach— reinforcing infarcts in only one direction (anisotropically)—in dogs with large anteroapical infarcts and found that anisotropic reinforcement can improve systolic function without impairing filling, significantly enhancing cardiac output curves. Long-term studies are now needed to determine whether anisotropic reinforcement early after infarction improves pump function enough to reduce the subsequent risk of heart failure. Anisotropic Reinforcement of Acute Anteroapical Infarcts Improves Pump Function Gregory M. Fomovsky, Samantha A. Clark, Katherine M. Parker, Gorav Ailawadi and Jeffrey W. Holmes Downloaded from http://circheartfailure.ahajournals.org/ by guest on May 10, 2017 Circ Heart Fail. 2012;5:515-522; originally published online June 4, 2012; doi: 10.1161/CIRCHEARTFAILURE.111.965731 Circulation: Heart Failure is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2012 American Heart Association, Inc. All rights reserved. Print ISSN: 1941-3289. Online ISSN: 1941-3297 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circheartfailure.ahajournals.org/content/5/4/515 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation: Heart Failure can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation: Heart Failure is online at: http://circheartfailure.ahajournals.org//subscriptions/