Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Electrocardiography wikipedia , lookup
Heart failure wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Cardiac surgery wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Coronary artery disease wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
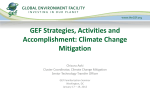
Journal of Cardiac Failure Vol. 13 No. 2 2007 Basic Science and Experimental Studies Enhanced Inotropic State of the Failing Left Ventricle by Cardiac Contractility Modulation Electrical Signals Is Not Associated With Increased Myocardial Oxygen Consumption CHRISTIAN BUTTER, MD,1 ERNST WELLNHOFER, MD,1 MICHAEL SCHLEGL, MD,1 GEORGIA WINBECK, MD,1 ECKART FLECK, MD,1 AND HANI N. SABBAH, PhD2 Berlin, Germany; Detroit, Michigan ABSTRACT Background: Previous studies in patients and in dogs with experimentally induced heart failure (HF) showed that electrical signals applied to the failing myocardium during the absolute refractory period improved left ventricular (LV) function. We examined the effects these same cardiac contractility modulating (CCM) electrical signals on myocardial oxygen consumption (MVO2) in both patients and dogs with chronic HF. Methods and Results: Six dogs with microembolizations-induced HF and 9 HF patients underwent CCM leads and generator (OPTIMIZER II) implantation. After baseline measurements, CCM signals were delivered continuously for 2 hours in dogs and for 30 minutes in patients. MVO2 was measured before and after CCM therapy. In dogs, CCM therapy increased LV ejection fraction at 2 hours (26 6 1 versus 31 6 2 %, P 5 .001) without increasing MVO2 (257 6 41 versus 180 6 34 mmol/min). In patients, CCM therapy increased LV peak þdP/dt by 10.1 6 1.5 %. As with dogs, the increase in LV function after 30 minutes of CCM therapy was not associated with increased MVO2 (13.6 6 9.7 versus 12.5 6 7.2 mL O2/min). Conclusions: The study results suggest that unlike cAMP-dependent positive inotropic drugs, the increase in LV function during CCM therapy is elicited without increasing MVO2. (J Cardiac Fail 2007;13:137e142) Key Words: Ventricular function, Positive inotropic agents, Congestive heart failure, Device therapy for heart failure. Despite marked improvements in pharmacologic treatments that reduce mortality and morbidity in patients with chronic heart failure (HF),1e3 a large number of patients with advanced HF are refractory to optimal standard medical therapy. This patient population mostly New York Heart Association (NYHA) class III and IV require additional therapy to limit progression of their disease and improve their quality of life. The need for further therapeutic interventions in this patient population has given rise to a host of device-based therapies such cardiac resynchronization therapy among others. Biventricular pacing or resynchronization therapy has been shown to improve LV systolic function and quality of life in a subset of these patients who a manifest wide QRS complex.4e7 Cardiac contractility modulation (CCM) electrical signals delivered to the failing myocardium during the absolute refractory period is another device-based therapy targeting this HF population. CCM electrical signals applied to the myocardium during the absolute refractory period can increase have been shown to increase systolic function of the failing LV.8e17 Preliminary clinical studies of CCM signals delivered to the myocardium of patients with chronic HF suggest that CCM therapy is safe and can also improve exercise tolerance and quality of life.18,19 Classic positive inotropic From the 1German Heart Institute Berlin, Berlin, Germany and Division of Cardiovascular Medicine, Henry Ford Health System, Detroit, Michigan. Manuscript received January 13, 2006; revised manuscript received November 2, 2006; revised manuscript accepted November 3, 2006. Reprint requests: Christian Butter, MD, Heart Center Brandenburg Bernau/Berlin, Ladeburger Str. 17, 16321 Bernau, Germany. Supported, in part, by research grants from Impulse Dynamics USA and by National Heart, Lung, and Blood Institute PO1 HL074237-03. 1071-9164/$ - see front matter Ó 2007 Elsevier Inc. All rights reserved. doi:10.1016/j.cardfail.2006.11.004 2 137 138 Journal of Cardiac Failure Vol. 13 No. 2 March 2007 agents such as dobutamine and milrinone improve LV systolic function in patients with HF. The cost for this improvement, however, is increased myocardial oxygen consumption (MVO2), a payment that the failing LV myocardium can ill afford.20 The purpose of this study was to determine whether the increase of LV systolic function observed during CCM therapy is also associated with increased MVO2. Methods Animal Protocol The canine model of chronic HF used in the present study was previously described in detail.13e15 In this experimental preparation, chronic LV dysfunction and failure is produced by multiple sequential intracoronary embolizations with polystyrene Latex microspheres (70e102 mm in diameter) that result in loss of viable myocardium, LV enlargement, and a decrease in LV ejection fraction. In the present study, 11 healthy mongrel dogs weighing between 20 and 26 kg underwent serial coronary microembolizations to produce HF. Embolizations were performed 1 week apart and were discontinued when LV ejection fraction, determined angiographically, was !30%. Microembolizations were performed during cardiac catheterization under general anesthesia and sterile conditions. Animals were sedated with intravenous oxymorphone hydrochloride (0.22 mg/kg) and diazepam (0.17 mg/kg) and a plane of anesthesia was maintained with 1% to 2% isoflurane. The study was approved by Henry Ford Health System Institutional Animal Care and Use Committee and conformed to the National Institute of Health ‘‘Guide and Care for Use of Laboratory Animals’’ and the ‘‘Position of the American Heart Association on Research Animal Use.’’ Two weeks after the target LV ejection fraction was reached, dogs were anesthetized as described previously, intubated, and ventilated with room air. In 6 dogs, the right external jugular vein was surgically exposed and used to position the CCM leads. Two standard active fixation leads were positioned on the anterior and posterior septal grooves and were used sense ventricular activity and to deliver CCM electrical signals. A third active fixation lead was positioned in the right atrium for sensing. The leads were connected to a CCM signal generator (OPTIMIZER II, Impulse Dynamics USA, Inc, Orangeburg, NY). The generator was implanted in a subcutaneous pocket created on the right side of the neck. The animals were allowed to recover. Studies were performed 2 weeks after CCM system implantation. This period of time also allowed the tip of the leads to mature into place. The remaining 5 of 11 dogs were not treated and served as controls. Two weeks after CCM system implantation, dogs were anesthetized and underwent a baseline left and right heart catheterization that included measurement of MVO2. The Optimizer II system was then activated to deliver 7.73 volts CCM electrical signals continuously for 2 hours. At the end of 2 hours of CCM delivery, all hemodynamic measures were repeated including MVO2. Left ventricular pressure was measured using a catheter-tip micromanometer (Millar Instruments, Houston, TX) and LV end-diastolic pressure was measured from the phasic LV pressure waveform. Stroke volume was calculated as the ratio of cardiac output to heart rate. MVO2 and LV external power (watts) were measured as previously described in detail.21 The same hemodynamic measurements were made at the same study time points in control dogs. Table 1. Hemodynamic and Ventriculographic Findings in Untreated Heart Failure Control Dogs Obtained at Baseline and After 2 hours of Follow-up (n 5 5) Baseline HR (beats/min) Peak LVP (mm Hg) LV EDP (mm Hg) Stroke Volume (mL) LV EDV (mL) LV ESV (mL) LV EF (%) LV CBF (mL/min) LV Power (watts) MVO2 (mmol/min) 90 98 12 18 67 49 27 20 0.35 191 6 6 6 6 6 6 6 6 6 6 5 9 1 1 2 1 1 2 0.03 19 2 Hours P value 6 6 6 6 6 6 6 6 6 6 .39 .39 .10 .18 .53 .78 .37 .13 .82 .54 95 108 12 18 67 49 27 22 0.38 201 5 6 1 1 1 1 1 2 0.03 31 HR, heart rate; LVP, left ventricular systolic pressure; EDP, end-diastolic pressure; EDV, end-diastolic volume; ESV, end-systolic volume; EF, ejection fraction; CBF, coronary blood flow; MVO2, myocardial oxygen consumption; P value 5 probability value of baseline versus 2 hours. Patient and Protocol The clinical characteristics of all 9 patients included in this single center sub-study are shown in Table 1. The cohort of 9 patients was participating in a randomized, double blind multicenter study to test the safety and efficacy of CCM therapy in patients with HF (the FIX-HF-4 Study, IMPULSE Dynamics USA, Inc). All 9 patients had NYHA class III symptoms despite of treatment with b-blockers, angiotensin-converting enzyme inhibitors, or angiotensin receptor blockers and, with 1 exception, the aldosterone receptor antagonist spironolactone. Patients were excluded from the study if they had been hospitalized within 1 month for acute exacerbation of HF or had undergone revascularization within 1 month with either percutaneous coronary intervention of coronary artery bypass surgery or they experience an acute myocardial infarction within 3 months of entry into the study. The study was approved by the local institutional review committee. Written informed consent was obtained from all patients before entry into the study. Right heart and left heart catheterizations were performed according to standard clinical practice using the transfemoral approach. The OPTIMIZER II system employs 2 leads placed on the right ventricular septum and one lead in the right atrium (Fig. 1). Septal lead placement is optimized to achieve the greatest possible increase in peak LV þdP/dt. The latter was measured in Fig. 1. Example of instrumentation in anteroposterior view (A) and final lead placement in left anterior oblique projection (B) in patients. The Millar catheter (pigtail) is placed in the left ventricle. The 2 right ventricular septal leads apply cardiac contractility modulating signals. The venous catheter is in the coronary sinus and the defibrillator lead points to the right ventricular apex. Oxygen Consumption With CCM Therapy all patients. The OPTIMIZER II system was implanted in all patients in whom peak LV þdP/dt increased more than 5% during CCM signal delivery. A 0.014-inch Doppler guide wire (Jometrics, FloWire XT, Jomed, Rancho Cordova)22 was positioned in the left main coronary artery to measure average peak flow velocity (APV). The diameter (D) in mm of the coronary arterial segment used for flow sampling was estimated by quantitative angiography. Assuming a parabolic flow profile and a circular lumen coronary blood flow (CBF) was calculated as: CBF 5 60*APV/ 2*0.01*(p/4)*D2 mL/min.23 A coronary sinus catheter was placed for coronary venous blood sampling. Coronary sinus and coronary arterial blood samples were analyzed for hemoglobin concentration and oxygen saturation, which were converted to blood oxygen content (volume %, mL O2/100 mL blood). The product of CBF and arteriovenous oxygen content difference (AVDO2) was used as a measure of MVO2.21 CBF and AVDO2 were measured in triplicate and the average of all 3 measurements reported. After baseline hemodynamic measurements and acquisition of blood samples, CCM signals were delivered for 30 minutes. Measurements were then repeated. Stability of the Doppler flow wire tip position was confirmed with fluoroscopy. Data Analysis Comparison between baseline measurements and measurements obtained at 2 hours (dogs) and 30 minutes (patients) after initiating CCM signal delivery were made using a Students paired t-test with significance set at P value ! .05. All data are reported as the mean 6 SEM. Results Butter et al 139 rate and peak LV pressure did not change with CCM therapy. Compared with baseline, CCM therapy significantly decreased LV end-diastolic pressure and significantly increased stroke volume. Left ventricular end-diastolic volume and end-systolic volume both decrease significantly with CCM therapy and LV ejection fraction and LV external power increased significantly. Compared with baseline, CBF decreased with CCM therapy and MVO2 tended to decrease but the reduction did not reach statistical significance (Table 2). Findings in Patients With HF Compared with baseline, 30 minutes of CCM therapy significantly increased peak LV þdP/dt from 701 6 48 to 775 6 60 mm Hg/s (Table 3). APV between baseline (30 6 7 cm/s) and 30 minutes after initiating CCM delivery did not change (29 6 8 cm/s). Differences in individual patients were negligible (Fig. 2, top). Consistent with these measurements, estimated average CBF was nearly identical between baseline (100 6 20 mL/min) and 30 minutes after initiating CCM signal delivery CCM (97 6 18 mL/min). AVDO2 was not changed after CCM therapy compared with baseline (13.2 6 1.0 versus 12.8 6 1.4 mL O2/100 mL). Thus, estimated MVO2 remained essentially unchanged (13.6 6 3.2 versus 12.5 6 2.4 mL O2/min) (Fig. 2, bottom). Discussion Findings in Dogs with HF The hemodynamic and ventriculographic results obtained in control dogs are shown in Table 1. Heart rate and peak LV pressure did not change during the 2 hours of follow-up. In this control group, 2 hours of follow-up had no significant effects on LV end-diastolic pressure, stroke volume, LV end-diastolic volume, LV end-systolic volume, LV ejection fraction, CBF, LV external power, or MVO2 when compared to baseline (Table 1). The hemodynamic and ventriculographic results obtained in CCM-treated dogs are shown in Table 2. Heart Table 2. Hemodynamic and Ventriculographic Findings in Dogs with Heart Failure Obtained at Baseline and 2 hours After Initiating CCM Therapy (n 5 6) Baseline HR (beats/min) Peak LVP (mm Hg) LV EDP (mm Hg) Stroke volume (mL) LV EDV (mL) LV ESV (mL) LV EF (%) LV CBF (mL/min) LV Power (watts) MVO2 (mmol/min) 79 101 14 18 71 53 26 35 0.32 257 6 6 6 6 6 6 6 6 6 6 3 5 1 1 8 7 1 4 0.02 41 2 Hours of CCM P value 6 6 6 6 6 6 6 6 6 6 .26 .23 .005 .004 .001 .001 .001 .017 .040 .12 75 107 9 21 68 47 31 27 0.37 180 3 8 1 1 7 6 2 3 0.03 34 Abbreviations are same as in Table 1. CCM, cardiac contractility modulation; P value 5 probability value of baseline versus CCM. CCM-mediated enhancement of LV contractile performance is a new frontier of electrical therapy for HF in patients not eligible for resynchronization therapy. This is the first study in both dogs with experimentally induced HF and in patients with chronic HF that examined the effects of CCM-mediated enhancement of contractile performance on MVO2. The results suggest that acute CCM therapy significantly increased LV systolic function without increasing MVO2. The extent acute increase in peak LV þ dP/dt in patients after acute CCM therapy seen in the present study is consistent with changes of peak LV þ dP/dt reported in previous studies in patients with HF.16,18,19 The hemodynamic and angiographic changes observed in this study in dogs with HF that were treated with CCM could not be attributed to changes in loading conditions that may have occurred during the 2 hours of follow-up. A control group of HF dogs also followed under anesthesia for 2 hours showed no changes in indexes of LV function. With the growing number of patients with advanced HF in whom pharmacologic therapy has been optimized, but who remain symptomatic with depressed LV systolic function, efforts continue to identify safe therapies to improve LV function and relieve symptoms. In the past, b-adrenoceptor agonists and selective phosphodiesterase III inhibitors were explored for this purpose but were associated with increased mortality. The causes of adverse effects of these agents, which act primarily via cAMP mechanisms are not fully 140 Journal of Cardiac Failure Vol. 13 No. 2 March 2007 Table 3. Patient Characteristics at Baseline and Peak Left Ventricular þdP/dt During CCM Application Patient Gender Age (years) HF Etiology EF (%) VO2-max (mL$min$kg) Baseline Peak LV þdP/dt (mm Hg/s) CCM Peak LV þdP/dt (mm Hg/s) Peak LVþ dP/dt (% change) Male Male Male Male Male Male Male Male Male 65 63 50 50 66 48 66 40 62 DCM DCM DCM DCM CAD DCM CAD CAD CAD 25 25 22 19 28 23 25 30 29 13.4 12.3 12.9 17.2 13.6 11.7 17.3 12.4 17.3 733 580 770 900 550 460 860 750 710 847 613 834 988 601 485 1020 830 761 15.6 5.7 8.3 9.8 9.3 5.4 18.6 10.7 7.2 25 1 14.2 0.8 701 48 775 60 10.1 1.5 PR GS HP GS LS SU HO NB DL Mean SEM 57 3 EF, ejection fraction; HF, heart failure; VO2-max, peak oxygen consumption; LV, left ventricular; þdP/dt, peak positive rate of change of LV pressure during isovolumic period, CCM, cardiac contractility modulation. Average Peak Velocity (cm/s) understood. It has been shown that MVO2 increases with dobutamine by as much as 42% when the dose of dobutamine was sufficient to increase peak LV þ dP/dt by 37%.6 The effects of new HF treatments on MVO2 remain of primary interest. Furthermore, in contrast to systemic pharmacologic inotropes with multiple actions on the heart and the vascular system, an electrical treatment such as CCM acts locally and appears to be devoid of positive chronotropic effects, proarrhythmic effects and systemic blood pressure lowering effects. In addition, CCM therapy is designed to be intermittent and, therefore, the phenomenon of tachyphylaxis may not be a factor in contrast to pharmacologic treatment. Trend Average Peak Velocity 100.00 PR 04-12-01 GS 04-12-02 HP 04-12-04 GS 04-12-05 LS 04-12-06 SU 04-12-07 HO 04-12-08 NB 04-12-09 RM 04-12-10 RW 04-12-11 DL 04-12-12 Average 80.00 60.00 40.00 20.00 0.00 1 2 Oxygen consumption (ml/min) 1: Prä CCM - 2: Post CCM Trend myocardial oxygen consumption 70.00 PR 04-12-01 GS 04-12-02 HP 04-12-04 GS 04-12-05 LS 04-12-06 SU 04-12-07 HO 04-12-08 NB 04-12-09 RM 04-12-10 RW 04-12-11 DL 04-12-12 Average 60.00 50.00 40.00 30.00 20.00 10.00 0.00 1 2 1: Prä CCM - 2: Post CCM Fig. 2. Coronary blood flow velocity (top) and myocardial oxygen consumption (bottom) at baseline (PRE) and after cardiac contractility modulating signal application (POST). Acute increases in peak LV þ dP/dt in the range of 20% have been reported with cardiac resynchronization therapy. This increase in peak LV þ dP/dt were also associated with no change in MVO2. Although the changes are somewhat larger than observed in the present study with CCM therapy, preliminary findings indicate that LV ejection fraction increases by about 5% with chronic CCM,18,19 which compares favorably with the reported effects of chronic treatment with resynchronization therapy.5 The results seen in this study in dogs with HF also suggest that the effects of CCM on LV systolic function is more robust as time of therapy is increased and, despite a marked increase in LV ejection fraction in the dogs, MVO2 remained unchanged. The mechanism by which CCM signals are believed to acutely enhance contractility have been attributed to normalization of calcium handling,14,24,25 whereas mechanisms that underlie the benefits of resynchronization therapy are likely related to coordination of myocardial contraction. Thus synergistic effects of CRT and CCM may be expected.10,16 Early studies in isolated Langendorff-perfused ferret hearts of the mechanisms of action of CCM therapy suggested that the positive inotropism of CCM therapy may be due to increased peak [Ca2þ]i.12 Early studies also focused on the potential impact of CCM signals on action potential configuration which acts to enhance calcium loading of the SR.8,11 In these early studies, the increase in calcium was assumed to be the sole cause of the increase in contractility. More recent studies, however, have suggested that in vivo delivery of CCM signals to the failing canine myocardium can, within a short period of 2 to 4 hours, lead to increased phosphorylation of phospholamban.14 It has been suggested that electromagnetic fields can modify enzyme reactions.26 Enhanced phosphorylation of phospholamban seen within as little as 2 hours of CCM signal application suggests that this type of electrical therapy can modulate the phosphorylation of proteins. In this case, the already existing phospholamban protein is being phosphorylated rather than synthesis of new protein. Phosphorylation of phospholamban enhances sarcoplasmic reticulum calcium sequestration by enhancing the activity or affinity of SERCA-2a for calcium. In turn, this Oxygen Consumption With CCM Therapy enhances intracellular calcium cycling capacity and, hence, contractility. In the short-term (hours and days), CCM therapy is thought to improve function in the LV region adjacent to the site of CCM signal delivery.11 In the present studies, the site of CCM signal delivery in both patients and dogs was the interventricular septum. Acute delivery of CCM therapy appears to impact enough myocardium at the regional level so as to enhance global LV function13,27 as also evident from the present study. Thus measures of global LV contractile function such as ejection fraction and peak þ dP/dt, are expected to correlate with global measures of MVO2 that are partly based on measurements of oxygen content in blood drawn from the coronary sinus. Limited studies have suggested that in dogs, not all venous affluent from the interventricular septum empties into the coronary sinus28 an anatomic condition that may affect the correlation between LV function and MVO2 in the present study. In addition to these limitations, there are other limitations to the study that merit consideration. The study in patients and the one in dogs were conducted in different laboratories with different protocols and were only combined after the fact to illustrate the same effects of CCM therapy in both patients and dogs with HF. This led to the use of different indexes of LV performance. Nonetheless, the results from both patients and dogs were directionally similar. Calculation of MVO2 from coronary blood flow velocity measurements and arteriovenous oxygen content difference is an established method,6 estimates of total CBF were made in both studies in dogs with HF and in HF patients.21 In patients and in dogs, measurements of velocity and oxygen content of blood samples and additional quantitative coronary angiography were made in triplicate or in duplicate to enhance the accuracy. In the present study, the increase in peak LV þ dP/dt measured in patients undergoing implantation of the CCM system was modest (approximately 10%) and one may argue that this modest increase may not be sufficient to elicit an increase MVO2. Studies in dogs in which CCM therapy was delivered for a longer time (2 hours) in the absence of the type of constraints that one faces in studies in human subjects, however, also showed that MVO2 was unchanged despite an increase in LV ejection fraction of approximately 20%. Conclusions In a manner consistent with previous studies, the present study suggests that acutely applied CCM signals increase systolic LV function in patients with advanced HF despite background therapy with angiotensin-converting enzyme inhibitors, b-adrenergic receptor blockers, and, in some cases, aldosterone receptor blockers. Importantly, the study results suggest that the increase in LV function during CCM therapy is elicited without increasing MVO2. At present, CCM therapy remains investigational. Ongoing randomized clinical trials are underway in Europe and the United States and, when completed, will establish the efficacy or lack Butter et al 141 thereof of this form of novel electrical therapy for chronic advanced HF. References 1. Packer M, Coats AJ, Fowler MB, et al. Effect of carvedilol on survival in severe chronic heart failure. N Engl J Med 2001;344:1651e8. 2. Pitt B, Zannad F, Remme WJ, et al. The effect of spironolactone on morbidity and mortality in patients with severe heart failure. Randomized Aldactone Evaluation Study Investigators. N Engl J Med 1999; 341:709e17. 3. Moss AJ, Zareba W, Hall WJ, et al. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med 2002;346:877e83. 4. Cazeau S, Leclercq C, Lavergne T, et al. Effects of multisite biventricular pacing in patients with heart failure and intraventricular conduction delay. N Engl J Med 2001;344:873e80. 5. Abraham WT, Fisher WG, Smith AL, et al. Cardiac resynchronization in chronic heart failure. N Engl J Med 2002;346:1845e53. 6. Nelson GS, Berger RD, Fetics BJ, et al. Left ventricular or biventricular pacing improves cardiac function at diminished energy cost in patients with dilated cardiomyopathy and left bundle-branch block. Circulation 2000;102:3053e9. 7. Auricchio A, Abraham WT. Cardiac resynchronization therapy: current state of the art: cost versus benefit. Circulation 2004;109:300e7. 8. Burkhoff D, Shemer I, Felzen B, et al. Electric currents applied during the refractory period can modulate cardiac contractility in vitro and in vivo. Heart Fail Rev 2001;6:27e34. 9. Ellison K. Nonexcitatory stimulation: 2002: a pace odyssey. J Cardiovasc Electrophysiology 2002;13:696e7. 10. Marrouche NF, Pavia SV, Zhuang S, et al. Nonexcitatory stimulus delivery improves left ventricular function in hearts with left bundle branch block. J Cardiovasc Electrophysiol 2002;13:691e5. 11. Mohri S, He KL, Dickstein M, et al. Cardiac contractility modulation by electric currents applied during the refractory period. Am J Physiol Heart Circ Physiol 2002;282:H1642e7. 12. Mohri S, Shimizu J, Mika Y, et al. Electric currents applied during the refractory period enhance contractility and systolic calcium in ferret. Am J Physiol Heart Circ Physiol 2003;284:1119e23. 13. Morita H, Suzuki G, Haddad W, et al. Cardiac contractility modulation with nonexcitatory electric signals improves left ventricular function in dogs with chronic heart failure. J Card Fail 2003;9:69e75. 14. Mishra S, Gupta RC, Rastogi S, Haddad W, Mika Y, Sabbah HN. Short-term therapy with nonexcitatory cardiac contractility modulation electric signals increases phosphorylation of phospholamban in left ventricular myocardium of dogs with chronic heart failure: [abstract]. Circulation 2004;110:III-604. 15. Morita H, Suzuki G, Haddad W, et al. Long-term effects of non-excitatory cardiac contractility modulation electric signals on the progression of heart failure in dogs. Eur J Heart Fail 2004;6:145e50. 16. Pappone C, Rosanio S, Burkhoff D, et al. Cardiac contractility modulation by electric currents applied during the refractory period in patients with heart failure secondary to ischemic or idiopathic dilated cardiomyopathy. Am J Cardiol 2002;90:1307e13. 17. Pappone C, Vicedomini G, Salvati A, et al. Electrical modulation of cardiac contractility: clinical aspects in congestive heart failure. Heart Failure Rev 2001;6:55e60. 18. Pappone C, Augello G, Rosanio S, et al. First human chronic experience with cardiac contractility modulation by nonexcitatory electrical currents for treating systolic heart failure: mid-term safety and efficacy results from a multicenter study. J Cardiovasc Electrophysiol 2004;15: 418e27. 19. Stix G, Borggrefe M, Wolpert C, et al. Chronic electrical stimulation during the absolute refractory period of the myocardium improves severe heart failure. Eur Heart J 2004;25:650e5. 20. Suga H. Ventricular energetics. Phys Rev 1990;70:247e77. 142 Journal of Cardiac Failure Vol. 13 No. 2 March 2007 21. Chandler MP, Stanley WC, Morita H, Suzuki G, Roth BA, Blackburn B, et al. Acute treatment with ranolazine improves mechanical efficiency in dogs with chronic heart failure. Circ Res 2002;91:278e80. 22. Doucette JW, Corl PD, Payne HM, et al. Validation of a Doppler guide wire for intravascular measurement of coronary artery flow velocity. Circulation 1992;85:1899e911. 23. Sagawa K. Editorial: the end-systolic pressure-volume relation of the ventricle: definition, modifications and clinical use. Circulation 1981; 63:1223e7. 24. Gupta RC, Mishra M, Rastogi S, Imai M, Haddad W, Mika Y, et al. Non-excitatory cardiac contractility modulation electric signals normalize phosphorylation and expression of the sodium-calcium exchanger in left ventricular myocardium of dogs with heart failure: [abstract]. J Am Coll Cardiol 2005;45:151A. 25. Gupta RC, Mishra S, Imai M, Mika Y, Sabbah HN. Cardiac contractility modulation with non-excitatory electric signals normalizes expression of the transcriptional factor GATA-4 in dogs with chronic heart failure. Heart Rhythm 2005;2:S138. 26. Blank M, Goodman R. Initial interactions in electromagnetic fieldinduced biosynthesis. J Cell Physiol 2004;199:359e63. 27. Lawo T, Borggrefe M, Butter C, Hindricks G, Schmindinger H, Mika Y, et al. Electrical signals applied during the absolute refractory period: an investigational treatment for advanced heart failure in patients with normal QRS Duration. J Am Coll Cardiol 2005;46: 2229e36. 28. Shiki K, Masuda M, Yonenaga K, Asou T, Tokunaga K. Myocardial distribution of retrograde flow through the coronary sinus of the excised normal canine heart. Ann Thorac Surg 1986;41:265e71.