Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
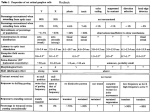
Patterns of neural degeneration in the human cochlea and auditory nerve: Implications for cochlear implantation JOSEPH B. NADOL, Jr, MD, Boston, Massachusetts Although the identity of all the variables that may influence speech recognition after cochlear implantation is unknown, the degree of preservation of spiral ganglion cells is generally considered to be of primary importance. A series of experiments in our laboratories, directed at quantification of surviving spiral ganglion cells in the profoundly deaf, evaluation of the predictive value of a variety of clinical parameters, and the evaluation of the consequences of implantation in the inner ear, is summarized. Histologic study of the inner ears of patients who were deafened during life demonstrated that the cause of deafness accounted for 57% of the variability of spiral ganglion cell counts. Spiral ganglion cell counts were highest in individuals deafened by aminoglycoside toxicity or sudden idiopathic deafness and lowest in those deafened by postnatal viral labyrinthitis, congenital or genetic deafness, or bacterial meningitis. Study of the determinants of degeneration of the spiral ganglion revealed that degeneration is most severe in the basal compared with the apical turn and more severe when both inner and outer hair cells are absent. Unlike the findings in some experimental animal studies, no survival advantage of type II ganglion cells could be identified. There was a strong negative correlation between the degree of bony occlusion of the cochlea and the normality of the spiral ganglion cell count. However, even in specimens in which there was severe bony occlusion, significant numbers of spiral ganglion cells survived. A strong positive correlation between the diameter of the cochlear, vestibular, and eighth cranial nerves with the total spiral ganglion cell count (p < 0.001) was found. This would suggest that modern imaging techniques may be used to predict residual spiral ganglion cell population in cochlear implant candidates. Trauma from implantation of the electrode array was studied in both cadaveric human temporal bone models and temporal bones from individuals who received implants during life. A characteristic pattern of damage to the lateral cochlear wall and basilar membrane was identified in the upper basal turn. New bone formation and perielectrode fibrosis was common after cochlear implantation. Despite this significant trauma and reaction, there is no firm evidence that further degeneration of the spiral ganglion can be predicted as a consequence. (Otolaryngol Head Neck Surg 1997;117:220-8.) A l thet identity h ofo all uthe variables g hthat may influence the success of speech recognition after cochlear implantation is unknown, the degree of preset- Supported by grant no. 5P01 DC00361 from the National Institute on Deafness and Other CommunicationDisorders, National Institutes of Health. Presented at the Sixth Symposiumon CochlearImplants in Children, Miami Beach, Fla., Feb. 2-3, 1996. Reprint requests: Joseph B. Nadol, Jr, MD, Department of Otolaryngology,Massachusetts Eye and Ear Infirmary,243 Charles St., Boston, MA 02114. Copyright © 1997 by the American Academy of OtolaryngologyHead and Neck SurgeryFoundation, Inc. 0194-5998/97/$5.00 + 0 23/1/75094 220 vation of spiral ganglion cells is generally considered to be of primary importance. 1 Therefore an understanding of the degenerative patterns of the spiral ganglion in the multiple causes that result in profound deafness would be useful. Based on correlation between spiral ganglion cell counts from temporal bone studies and premortem clinical parameters such as age, sex, comorbidity, cause of deafness, radiologic findings, and duration of deafness, a formula for predicting spiral ganglion cell counts in implant candidates could theoretically be developed, The strength of correlation between performance of cochlear implant recipients, as judged by speech-recognition scores, and predicted spiral ganglion cell counts could then be calculated. Finally, if such correlations are OtolaryngologyHead and Neck Surgery NADOL 221 Volume 117 Number 3 Part 1 strong, prognostication of success of cochlear implantation in a given candidate might be possible, based on predicted spiral ganglion cell counts. Insertion of an implant electrode will result in trauma to the inner ear. Based on limited human and animal temporal bone data, the long-term consequences of implantation on survival of spiral ganglion cells remain controversial. The purpose of this article is to summarize a series of experiments in our laboratories, directed at quantification of surviving spiral ganglion cells in the profoundly deaf, evaluation of the value of a variety of clinical parameters in predicting residual spiral ganglion cell counts, and evaluation of the consequences of implantation on the inner ear. METHODS AND MATERIAL Archival Temporal Bone D a t a b a s e From the temporal bone collection at the Massachusetts Eye and Ear Infirmary, 93 temporal bones from 66 patients who, during life, had documented profound sensorineural loss were used for this study. Of these, nine temporal bones were from six patients who in life suffered profound sensorineural loss as a result of bacterial meningitis. To evaluate the correlation between the diameter of the cochlear nerve and the survival of spiral ganglion cells, 47 temporal bones were analyzed. Of these, 42 were from patients with a clinically documented history of profound deafness, and five were from patients with normal hearing. In each instance only one temporal bone per individual was evaluated. For each patient the cause of deafness, age at onset of hearing loss, duration of hearing loss, age at onset of total deafness, and duration of total deafness were documented. In an effort to understand the implications of the presence of labyrinthitis ossificans for spiral ganglion cell survival, a quantitative study of six temporal bones from individuals who were profoundly deafened by bacterial meningitis was evaluated. The severity of labyrinthitis ossificans was quantified by estimating the percentage of the volume of the membranous labyrinth replaced by new bone. The segmental and total spiral ganglion cell counts were compared with age-matched control subjects to determine the percent normality of residual spiral ganglion counts per segment and in total. 2 All temporal bones were fixed in Heidenhain-Susa solution or 10% buffered formalin, decalcified in trichloroacetic acid or ethylenediamine tetraacetic acid (EDTA), and embedded in celloidin. The temporal bones were sectioned at a thickness of 20 gm in the Table 1. Pearson c o r r e l a t i o n coefficients with spiral g a n g l i o n c o u n t ( o n e e a r from e a c h person) Variable Correlation Sex Age at death Age at onset of hearing loss Duration of hearing loss Age at onset of deafness Duration of deafness -0.10 -0.24 0,22 -0.41" 0.18 -0.401- From NadolJB Jr, YoungYS, Glynn RJ. Ann Otol RhinolLaryngol 1989;98:414-6. *p < 0.001. tp < 0.01. horizontal plane. Every tenth section was stained with hematoxylin and eosin and mounted on glass slides. To understand the cellular patterns of degeneration of the spiral ganglion better, an additional 12 human pathologic specimens and two normal neonatal specimens, in which fixation was achieved within 4 1/2 hours after death, were evaluated. All specimens were fixed in 2% paraformaldehyde and 2% glutaraldehyde in 0.1 mol/L phosphate buffer at pH 7.2 by perilymphatic perfusion through the oval and round windows before necropsy. After removal of excess bone, the otic capsule was thinned with a power drill and the specimens were decalcified i t 0.1 mol/L disodium EDTA with 1.25% glutaraldehyde in 0.1 mol/L phosphate buffer. The tissue was then stained en bloc with aqueous uranyl acetate, dehydraded in graded alcohols, and embedded in epon resin. For these studies, sections were cut at 2 gm and stained with 1% toluidine blue. Finally, temporal bones from humans who had received a cochlear implant during life and cadaveric human temporal bones in which cochlear implantation was done postmortem were evaluated by light microscopy to assess patterns of cochlear injury induced by the implantation process. These specimens were fixed in 10% buffered formalin, decalcified in buffered EDTA, stained en bloc with aqueous uranyl acetate, and embedded in araldite to allow serial sectioning of the temporal bone at a thickness of 35 gm with the electrode array maintained in situ. 3,4 Data Analysis Graphic reconstruction of serial sections by a method described previously5,6 were done. Statistical methods included analysis of variance, t tests, Pearson correlation coefficients, and multiple linear regression analysis with the BMDP statistical software. 7 Quantification of spiral ganglion cell counts was done by segmental analysis 6 or segmental density measurements, s OtolaryngologyHead and NeckSurgery September 1997 222 NADOL Total # Spiral Ganglion Cells 35,000 Sudden idiopathic SNHL ( n - 6) 30,000 Aminoglycoside ototoxicity (n - 8) 25,000 Normal hearing (n : 5) 20,000 t 15,000 10,000 5,000 - m m Neoplasm of temporal bone (n = 8) Bacterial labyrinthitis (n 11) Congenitalor genetic (n 9) Postnatalviral labyrinthitis (n 8) Fig. 1. Means and standard deviations of spiral ganglion cell counts in six most common diagnostic categories and five individuals with normal hearing. (SNHLSensorineural hearing loss.) (From Nadol JB Jr, Young Y-S,Glynn RJ. Ann Otol Rhinol Laryngol 1989:98;411-6.) Table 2, Summary of multiple linear regression analysis predicting total spiral ganglion cell c o u n t for ears from diagnostic groups 1, 3, 5, 6, 8, a n d 10" Variable Diagnostic group 3t Diagnostic group 51Diagnostic group 6t Diagnostic group 81Diagnostic group 10t Age at death (yr) Age at deafness (yr) Sex++ Constant Coefficient Standarderror 14,795' 5,293 11,029§ 2,871 12,524~ -36.2 -14.8 400 9,283 4,452 3,458 4,934 3,510 4,271 56.5 55.9 2,259 -- Reprinted with permission from Nadol JB Jr, Young Y-S, Glynn RJ. Ann Otol Rhinol Laryngol 1989;98:414-6. R2 = 0.446; R2 for a model containing only the five indicators of diagnostic groups = 0.425. *One ear was chosen from each patient for a total of 49 ears (one ear was deleted because age of deafness was unknown). 1Coefficients for a diagnostic group estimate the mean difference in counts between ears from that diagnostic group and ears from diagnostic group 1. ::p < 0.01. §p < 0.05. ++The coefficient of sex estimates the mean difference in counts between ears of men and ears of women. RESULTS Correlation of Survival of Spiral Ganglion Cells with Age, Duration, and Cause of Deafness The results of bivariate analysis of the correlation of total spiral ganglion cell counts with a number of clinical variables is displayed in Table 1. Spiral ganglion cell counts were generally lower in older compared with younger deaf individuals. The total spiral ganglion cell count tended to be negatively correlated with duration of hearing loss and deafness. The only correlations that reached statistical significance were between total spiral ganglion cell counts and duration of hearing loss and duration of total deafness. 9 Analysis of variance indicated that the mean total spiral ganglion cell counts were not equal across the six most common diagnostic groups (postnatal viral labyrinthitis, sudden idiopathic deafness, bacterial labyrinthitis, tumor of temporal bone or cerebellopontine angle, congenital or genetic causes, and aminoglycoside ototoxicity). Multiple regression analyses were performed with data from the 49 ears in the six most common diagnostic categories. The diagnostic grouping accounted for 57% of the variability in spiral ganglion cell count. Thus the major determinant of spiral ganglion cell count at death was the diagnostic category rather than the age at death, duration of deafness, or duration of hearing loss (Table 2). The means and standard deviations of spiral ganglion cell counts in the six most common diagnostic categories and five individuals with normal hearing are shown in Fig. 1. Thus spiral ganglion cells from individuals who were deafened by sudden idiopathic sensorineural loss or aminoglycoside ototoxicity were among the highest, whereas those from individuals deafened from congenital or genetic causes or postnatal viral labyrinthitis were among the lowest counts. In summary, the contribution of age and duration of deafness were much less significant than the OtolaryngologyHead and Neck Surgery Volume 117 Number 3 Part 1 NADOL 223 '31¢ 1O0 80 o~" ,.J O-o l o z W • • o _> > o.5 50 • ®e O c-j: • o ,,g 40 • ee o • e u} ee 20 S , e • o o o v e o e • • 2O 0.5 0.6 0.7 0.8 0.9 1 1.1 1.2 C.N. Diameter (mm) e 40 GO 80 IO0 % SURVIVAL TOTAL Fig. 2. Scatter plot of percent survival of type II spiral ganglion cells and all spiral ganglion cells in 12 pathologic and two normal human spiral ganglia, suggesting that survival of type II cells is highly correlated with survival of entire spiral ganglion. This suggests that there is no survival advantage for type II ganglion cells. (From Zimmermann CE, Burgess BJ, Nadol JB Jr. Hear Res 1995:90;192-201.) Fig. 3. Histogram of mean and standard deviation of spiral ganglion (SGC) cell count by maximum diameter of cechelar nerve (C.N,). (From Nadol JB Jr, Xu W-Z.Ann Otol Rhinol Laryngol ]992;]01:988-93.) %NORMAL SPG BY %BONY OCCLUSION 8O 70 cause of deafness. Insofar as the cause of deafness is known in many candidates for cochlear implantation, this clinical variable would seem to be a valuable prognosticator of spiral ganglion cell count and by extension, perhaps, valuable for prognostication of success with cochlear implantation. However, there was considerable variability of total spiral ganglion cell count within each diagnostic category. In addition, the minimum requisite number of functioning spiral ganglion cells and their optimal distribution along the cochlear partition is not known. Finally, the presence of the spiral ganglion cell as determined histopathologically does not guarantee that it was functioning normally during life. In an effort to validate the prognostic utility of estimating spiral ganglion cell count, the NU-6 scores of i6 recipients of cochlear implants with greater than 6 months' experience with the speech processor were correlated with the spiral ganglion cell counts. The correlation was low (R = 0.32), suggesting that spiral ganglion cell count alone may be a poor predictor of success. P a t t e r n s of D e g e n e r a t i o n Ganglion in t h e H u m a n Spiral !n a study of 12 human pathologic specimens and two normal neonatal specimens, the patterns of degeneration of the human spiral ganglion and their correlation with degeneration of the organ of Corti, age, sex, I2: 60 O o 5O ~ [ ] REGRESSION LINE o. ¢n 4o < nO z 30" 20 ° R = -.861 P = .025 (PEARSON) 10' =~ i i i I 10 20 30 40 50 60 % BONY OCCLUSION Fig. 4. There was negative correlation between spiral ganglion ($PG) count expressed as percentage of normal and degree of bony occlusion expressed as percentage of volume of cochlea. (From Nadol JB Jr, Hsu W. Ann Otol Rhinol Laryngol 1991;100:712- 6.) duration of deafness, and cochlear location were evaluated. 1° Degeneration of the spiral ganglion was significantly greater for the basal one half compared with the apical one half of the cochlea (p < 0.001). Linear regression analysis demonstrated a strong correlation between the presence of the organ of Corti and the density of type I spiral ganglion cells. In the pathologic specimens, the prevalence of type II ganglion cells as a OtoiaryngologyHead and Neck Surgery 224 NADOL September 1997 Table 3. C o r r e l a t i o n o f spiral g a n g l i o n c o u n t a n d n e r v e d i a m e t e r s w i t h h e a r i n g status ( t test) Parameters Spiral ganglion count Maximum diameter of cochlear nerve (mm) Maximum diameter of vestibular nerve (mm) Maximum diameter of eighth cranial nerve (mm) Normal (n = 5)* 27,304 1.04 0.98 2.02 + 4,203 (23,103-31,932) _+0.11 (0.90-1.20) _+0.08 (0.90-1.10) + 0.08 (1.90-2.10) 15,463 0.81 0.76 1.57 Deaf (n = 42)* p Value + 7,838 (0-29,997) _+0.15 (0.50-1.20) _+0.12 (0.50-1.00) _+0.26 (1.00-2.10) 0.0008 0.0067 0.0019 0.0001 Reprintedwith permissionfrom Nadol JB Jr, Xu W-Z. Ann Otol Rhinol Laryngo11992;101:988-93. *Data are expressedas mean + SD (range). percentage of the total remaining spiral ganglion cell population in each segment ranged from 0% to 17%, with an average of 8.6%. There was no significant correlation between the prevalence of type II ganglion cells and age, sex, or duration of deafness or the degree of degeneration of the spiral ganglion as a whole. Similar to the findings for type I ganglion cells, there was a strong correlation between the survival of type II ganglion cells and the preservation of the organ of Corti. As shown in Fig. 2, there was a strong correlation between survival of type II cells with survival of the spiral ganglion as a whole and, hence, no obvious survival advantage for the type II cell, compared with the type I cell. Correlation of the Diameter of the Nerve Trunks of the Internal Auditory Canal with Remaining Spiral Ganglion Cell Count Given the sizeable variability of spiral ganglion cell counts with other clinical parameters such as cause of deafness, age, and duration of deafness, a histologic correlation between the diameter of the eighth, auditory, and vestibular nerves in the internal auditory canal with the total spiral ganglion cell count was done in 42 individuals with clinically documented profound deafness, who in life would have been candidates for implantation, and in five temporal bones from patients with normal hearing, u The diameters of the nerve trunks were measured at their points of maximum diameter in the internal auditory canal. As shown in Table 3, the total spiral ganglion cell count and maximum diameters of the cochlear, vestibular, and eighth cranial nerves were significantly smaller in the deaf population than in the normal-hearing group. According to the Pearson correlation, the maximum diameter of the cochlear, vestibular, and eighth cranial nerves was strongly correlated with the spiral ganglion cell count (p = 0.0006, p = 0.0001, and p = 0.0003, respectively, and Fig. 3). However, there is considerable overlap in the range of diameters of cochlear nerves in deaf and hearing ears. Nevertheless, it would seem reasonable that modern imaging techniques, which are capable of demonstrating the soft tissue contents of the internal auditory canal, may be considered a way of evaluating residual spiral ganglion cell preservation. Implications of the Presence of Labyrinthitis Ossificans Labyrinthitis ossificans, or new bone formation within the cochlea, is a common finding in temporal bones from individuals who were deafened by bacterial meningitis. 12,13Despite the mechanical impediments to implantation, the presence of labyrinthitis ossificans is now considered only a relative, rather than absolute, contraindication to cochlear implantation. 13,14 As shown in Fig. 4, there was a statistically significant negative correlation between the percent bony occlusion and the percent normal spiral ganglion cell count. In all cases in which the segmental and total bony occlusion was less than 10%, there was at least 30% of the normal segmental and total spiral ganglion cell densities. Expressed in another way according to Pearson correlations, a statistically significant negative correlation (p < 0.05) was found between spiral ganglion cell counts and the presence of bony occlusion in segments 2 (7 to 15 mm) and 4 (23 mm to apex). For all four segments of the cochlea there was a negative correlation, weakest in segment 1 (0 to 6 mm; r = -0.30), between the degree of bony occlusion and spiral ganglion cell counts. Therefore because significant degrees of bony occlusion can be determined before surgery by computed tomography, it is possible to predict before surgery that severe degrees of bony occlusion will be correlated with lower total spiral ganglion cell counts. Hence if the hearing levels are comparable in both ears, this study would predict that the ear with less bony occlusion would have a higher spiral ganglion cell count and perhaps a highler likelihood of success with the cochlear implant. However, it is important to recognize that even in those specimens in which there was severe bony occlusion, significant numbers of spiral ganglion cells survived. Total absence of spiral ganglion cells was not found in any specimen with labyrinthitis ossificans after bacterial meningitis. Evaluation of Implantation Trauma to the Inner Ear A major potential factor determining long-term survival of cochlear neurons, particularly in the pediatric population, is the degree of trauma to the inner ear dur- OtolaryngologyHead and Neck Surgery NADOL 225 Vorume 117 Number 3 Part 1 Fig. 5. In cadaveric human temporal bone in which cochlear implanation was done postmortem, bone chips (BC) were carried into upper basal turn by advancing electrode array. (Original magnification ×138.) Fig. 6. Sixty-seven-year-old patient received cochlear implant in right ear 2 years before death. Electrode array (EA) in midbasal turn is surrounded by fibrous tissue (F). (Original magnification ×55.) ing the process of implantation. This may not only impact survival of spiral ganglion cells after implantation but also influence the ease of changing an electrode array if necessary. In a study of temporal bones in which cochlear implantation was done, a characteristic pattern of damage to the lateral cochlear wall in the 8 to 15 mm region was found. This consisted of damage to the spiral ligament and in some cases displacement or even disruption of the basilar membrane. Even without obvious intracochlear mechanical impediment such as presence of new bone, the electrode array may pass from the scala tympani into the scala media or scala vestibuli. In these cadaveric specimens, particles of bone from the OtolaryngologyHead and Neck Surgery 226 NADOL September 1997 Fig. 7. Seventy-two-year-old man received cochlear implant in his right ear 7 years before death, Here in the basal turn of the cochlea, a bail electrode (BE) is encased in new bone (NB) in the scala tympani, indicating that new bone formation occurred after implantation. (Original magnification x55.) round window cochleostomy were often carried deep within the inner ear with the advancing electrode array (Fig. 5). In an evaluation of in vivo implantations a similar pattern of damage to the cochlear wall was identified. Evidence for perielectrode fibrosis (Fig. 6) and some degree of new bone formation after implantation was also found (Fig. 7). However, despite this significant trauma, as judged from histopathologic study of humans with implants, there is evidence that postimplantation degeneration of the spiral ganglion as a consequence of implantation is not severe. For example, in one case in which implantation was done during life and in which there was significant trauma to the basilar membrane (Fig. 8) there was little apparent impact on spiral ganglion counts (Fig. 9). DISCUSSION A l t h o u g h all the parameters that influence the success of cochlear implantation as judged by speech recognition scores are unknown, the preservation of spiral ganglion cells is considered to be of primary importance. 1 Our ability to predict spiral ganglion cell preservation accurately from individual to individual or between ears in the same individual would therefore be valuable clinical information for the purpose of prognosticating success or selecting the ear to be implanted. Study of the temporal bone from humans who in life were deaf has indicated that spiral ganglion cell count decreases with age and the duration of deafness. However, the most significant predictor of spiral ganglion cell count appears to be the cause of deafness. Specimens from individuals who were deafened by aminoglycoside ototoxicity or sudden idiopathic sensorineural hearing loss had significantly higher residual spiral ganglion cell counts than those deafened by postnatal viral labyrinthitis or congenital or genetic causes. In evaluating the differential survival of types I and II spiral ganglion cells, no survival advantage for type II ganglion cells was identified in the human. This differs from the findings in some animal studies in which a positive survival advantage of type II ganglion cells was identified after trauma to the organ of Corti 15 or ototoxic insult. 16 The finding in the human of no survival advantage of type II ganglion cells suggests that in ears with reduced total spiral ganglion cell count approximately 85% to 90% of the residual spiral ganglion cells will be of the type I variety, which are thought to be of primary importance for the detection of the acoustic signal. The demonstration of a positive correlation between the residual spiral ganglion cell population and the diameter of the cochlear, vestibular, and eighth nerve trunks in temporal bone specimens provides optimism that preoperative imaging of potential candidates for cochlear implantation may prove to be a useful prognostic tool. The identification of labyrinthitis ossificans, or new OtolaryngologyHead and Neck Surgery NADOL 227 Volume 117 Number 3 Part 1 Fig. 8. Unstained 35 ~m axial section of implanted right ear in 62-year-olcl woman who became deaf after intravenous gentamycin 5 years before implantation. Electrode array (EA) was sectioned in situ. Disruption of basilar membrane (BM) is shown on left approximately 11 mm from round window membrane and displacement of basilar membrane is shown on right approximately 18 mm from round window membrane. (Original magnification x28.) (From Nadol JB Jr, Ketten DR, Burgess BJ. Laryngoscope 1994;104:299-303.) bone formation within the cochlea, as can be evaluated before surgery by computed tomography, predicts a reduced population of residual spiral ganglion cells. Therefore if other indications are equal, the ear with the smaller amount of new bone formation would be predicted to have the higher spiral ganglion cell count. On the other hand, the presence of even severe labyrinthitis ossiflcans does not predict total loss of the spiral ganglion population. Cochlear implantation in the human results in a predictable pattern of trauma to the inner ear. Previous studies have demonstrated significant trauma to the spiral ligament and basilar membrane near the site of insertion and at the 8 to 15 mm region or ascending segment of the basal turn. 17-21 In addition, in human temporal bone specimens from individuals who received a cochlear implant during life, there is evidence to suggest that new bone formation may occur after implantation. This may be due to the original cause of deafness, new bone introduced into the cochlea at the time of implantation, or damage to the cochlear blood supply from trauma to the lateral cochlear wall or basilar membrane at the time of implantation. The effects of implantation on the spiral ganglion cell count are less clear. In some studies 2°22 a decrease in the number of spiral ganglion cells on the implanted side compared with the nonimplanted side was identi- 7OOO 6000 tO00 ~O00 10~0 0 I I I I i I I~ASE C O C~'LP, A.R S E G M E N T A ~ E oToto~c Fig. 9. Calculated segmental spiral ganglion cell counts for imlanted and unimplanted side of patient described in Fig. 8, compared with average data for normal adult cochleae, patients with ototoxic deafness, and predicted counts for patient calculated by regression analysis. 8,9 (From Nadol JB Jr, Keften DR, Burgess BJ. Laryngoscope 1994; 104:299-303.) fled. In other studies no signficant effect of implantation was identified in either in humans 4J9,23 or animals. 24,25 However, some reports have demonstrated improved survival of residual spiral ganglion cell 228 NADOL counts on the implanted versus nonimplanted side in the experimental animal. 26,27 REFERENCES 1. Clopton BM, Spelman FA, Miller JM. Estimates of essential neural elements for stimulation through a cochlear prosthesis. Ann Otol Rhinol Laryngol Suppl 1980;89:5-7. 2. Nadol JB Jr, Hsu W. Histopathologic correlation of spiral ganglion cell count and new bone formation in the cochlea following meningogenic labyrinthitis and deafness. Ann Otol Rhinol Laryngol 1991;100:712-6. 3. Ketten DR, Nadol JB Jr, Burgess BL Short-term effects of multiple electrode implants. Abstracts of the Fourteenth Midwinter Research Meeting, Association for Research in Otolaryngology, 1991:114. 4. Nadol JB Jr, Ketten DR, Burgess BJ. Otopathology in a case of multichannel cochlear implantation. Laryngoscope 1994;104: 299-303. 5. Schuknecht HF.,Techniques for study of cochlear function and pathology in experimental animals: development of the anatomical frequency scale for the cat. Arch Otolaryngol 1953;58:37797. 6. Otte J, Schuknecht I-IF, Kerr AG. Ganglion cell populations in normal and pathological human cochleae: implications for cochlear implantation. Laryngoscope 1978 ;88:1231-46. 7. Dixon WJ, editor. BMDP statistical software. Berkeley, California: University of California; 1985. 8. Nadol JB Jr. Quantification of human spiral ganglion cells by serial section reconstruction and segmental density estimates. Am J Otolaryngol 1988;9:47-51. 9. Nadol JB Jr, Young YS, Gtyrm RJ. Survival of spiral ganglion cells in profound sensorineural hearing loss: implications for cochlear implantation. Ann Otol Rhinol Laryngol 1989;98:4116. 10. Zimmerman CE, Burgess BJ, Nadol JB Jr. Patterns of degeneration in the human cochlear nerve. Hear Res 1995;90:192-201. 11. Nadol JB Jr, Xu WZ. Diameter of the cochlear nerve in deaf humans: implications for cochlear implantation. Ann Otol Rhinol Laryngol 1992;101:988-93. 12. Eisenberg LS, Luxford WM, Becker TS, House WE Electrical sltimulation of the auditory system in children deafened by meningitis. Otolaryngol Head Neck Surg 1984;92:700-5. O|olaryngologyHead and NeckSurgery September 1997 13. Balkany T, Gantz B, Nadol JB Jr. Multichannel cochlear implants in partially ossified cochleas. Ann Otol Rhinol Laryngol Suppl 1988;97:3-7. 14. Gantz BJ, McCabe BF, Tyler RS. Use of multichannel cochlear implants in obstructed and obliterated cochleas. Otolaryngol Head Neck Surg 1988;98:72-81. 15. Spoendlin H. Retrograde degeneration of the cochlear nerve. Acta Otolaryngol (Stockh) 1975;79:266-75. 16. Leake PA, Hradek GT. Cochlear pathology of long term neomycin induced deafness in cats. Hear Res 1988;33:11-33. 17. Shepherd BK, Clark GM, Pyman BC, et al. Banded intracochlear electrode array: evaluation of insertion trauma in human temporal bones. Ann Otol Rhinol Laryngol 1985;94:559. 18. Kennedy DW. Multichannel intracochlear electrodes: mechanism of insertion trauma. Laryngoscope 1987;97:42-9. 19. Clark GM, Shepherd RK, Franz BK-H, et at. The histopathology of the human temporal bone and auditory central nervous system following cochlear implantation in a patient. Acta Otolaryngol Suppl (Stockh) 1988;448:1-65. 20. Zappia JK, Niparko JK, Oviatt DL, et al. Evaluation of the temporal bones of a multichannel cochlear implant patient. Ann Otot Rhinol Laryngol 1991;100:914-21. 21. O'Leary MJ, Fayad J, House WE et al. Electrode insertion trauma in cochlear implantation. Ann Otol Rhino1 Laryngol 1991;100:695-9. 22. Marsh MA, Coker NJ, Jenkins HA. Temporal bone histopathology of a patient with a Nucleus 22-channel cochlear implant. Am J Otol 1992;I3:241-8. 23. Linthicum FH, Fayad J, Otto SR, et al. Cochlear implant histopathology. Am J Otol 1991; 12:245-311. 24. Sutton D, Miller JM. Cochlear implant effects on the spiral ganglion. Ann Otol Rhinol Laryngol 1983;92:53-8. 25. Shephard RK, Clark GM, Black RC. Chronic electrical stimniation of the auditory nerve in cats. Acta Otolaryngol Suppl (Stockh) 1983;399:19-3t. 26. Loustean RJ. Increased spiral ganglion cell survival in electrically stimulated deafened guinea pig cochleae. Laryngoscope 1987;97:836-42. 27. Hartshorn DO, Miller JM, Altschuler RA. Protective effect of electrical stimulation in the deafened guinea pig cochlea. Otolaryngol Head Neck Surg 1991;104:311-26.