Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
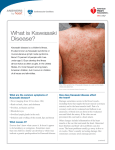
Emily Caudle Jill Collins Maria Cangiani AKA.. ◦ mucocutaneous lymph node syndrome -OR◦ infantile polyarteritis Characterized by an acute generalized systemic vasculitis occurring throughout the body Self-limiting and is the most common cause of acquired heart disease in children in Japan and the U.S. Over 80% of patients with Kawasaki disease are 4 years of age or younger ◦ Male to female ratio of 4:1 Etiology remains unknown Most exclusively affects young children Exhibits geographic and seasonal outbreaks Between 9.1 and 32.5 per 100,000 children contract the disease each year in the U.S. ◦ Clinical evidence supports an infectious cause ◦ with peak incidence between 13 and 24 months ◦ Increased rate of spread among children are low ◦ Late winter and early spring ◦ Incidence is HIGHER in Asian-American children, followed by African Americans, Hispanics and LOWEST in White children Disease is characterized by VASCULITIS ◦ begins in the small vessels and progresses to involve some of the larger arteries Immunologic abnormalities ◦ increased activation of helper T cells ◦ increased levels of immune mediators and antibodies destroy endothelial cells have been detected during the acute phase of the disease Pathophysiology ◦ Stage 1: acute phase (0-14 days) begins with abrupt onset of high fever that is unresponsive to antipyretics or antibiotics Significant irritability bilateral nonpurulent conjunctival injection, erythema or the oropharynx dryness and fissuring of the lips “strawberry tongue” cervical lymphadenopathy polymorphous rash erythema of urethral meatus tachycardia edema of extremities Lab findings: an elevated ESR platelet count positive CRP leukocytosis with left shift slight decreases in RBCs and hemoglobin. Initially platelets may be normal with gradual increase after 7th day of fever Stage 2: subacute phase (2-4 weeks after onset) ◦ Begins with resolution of fever and lasts until all other clinical signs have disappeared ◦ Desquamation of the fingers occurs first, followed by toes ◦ Coronary artery aneurysms appear during this period in 15% -25% of untreated children and less than 5% of treated children ◦ Death from the disease occur from cardiac sequelae 1545 days after onset of fever Stage 3: convalescent phase ◦ All clinical signs have resolved ◦ Lab values may not have returned to normal ◦ Phase complete when all blood values normal 6-8 weeks from onset Stage 4: chronic phase ◦ 40 days to years after illness ◦ Coronary complications, if present, can persist into adulthood ◦ Children with coronary dilation or aneurysms may have long-term coronary endothelial changes, which place the child at risk for early ischemic disease Child must exhibit FEVER for 5 days plus four of the other five criteria, or, if fewer than four criteria, coronary vessel involvement: ◦ ◦ ◦ ◦ Bilateral conjunctival injection without exudate Polymorphous rash that may be uticarial or pruritic Inflammatory changes in the lips and oral cavity Changes in the extremities, such as peripheral edema, erythema of the palms and soles, or desquamation of the hands and feet ◦ Cervical lymphadenopathy that is often unilateral, anterior cervical Conjuctival erythema Oral mucous membrane changes, injected or fissured lips, injected pharynx The word “injected” means RED Strawberry Tongue including erythema of palms or soles, edema of hands or feet (acute phase), and periungual desquamation (convalescent phase) PERIUNGUAL DESQUAMATION (Convalescent phase) The diagnostic of Kawasaki disease is based on clinical manifestations. The CDC requires that fever and four of the six other criteria listed above in stage I be demonstrated. Electrocardiogram, echocardiogram, cardiac catheterization, and angiocarddiography may be required to diagnose cardiac abnormalities. Although there are no specific laboratory tests, the following may help support diagnosis or rule out other disease. ◦ 1.CBC Leukocytosis during acute stage. ◦ 2.Erythrocytes and hemoglobin slight decrease. ◦ 3.Platelet count increased during second to fourth week of illness. ◦ 4.IgM, IgA, IgG, and IgF transiently elevated. ◦ 5.Urine protein and leukocytes present. ◦ 6.Acute phase reactants (ESR, C-reactive protein, alpha I antitrypsin) are elevated during the acute phase. ◦ 7.Myocardial enzyme levels (serum CK-MB) suggest MI if elevated. ◦ 8.Liver enzymes (AST, ALT) moderately elevated. ◦ 9.Lipid profile low high density lipoprotein and high triglyceride level. Measles Erythema Multiforme Leptospirosis Adenovirus Kawasaki Disease StevensJohnson Syndrome Kawaskaki Disease Scarlet Fever Drug reaction Inflammatory Bowel Disease Toxic shock Rickettsial Infection SLE Sarcoidosis Kawasaki disease has replaced acute rheumatic fever as the most common cause of acquired heart disease in children. Rheumatic fever (RF) is an inflammatory disease that may develop after an infection with Streptococcus bacteria (such as strep throat or scarlet fever). The disease can affect the heart, joints, skin, and brain. ◦ It arises as a complication of untreated or inadequately treated strep throat infection. Rheumatic fever can seriously damage the valves of the heart. Abdominal pain Fever Heart (cardiac) problems Joint pain, arthritis Joint swelling; redness or warmth Nosebleeds (epistaxis) Skin nodules Skin rash (erythema marginatum) Sydenham chorea ◦ which may not have symptoms, or may result in shortness of breath and chest pain ◦ mainly in the knees, elbows, ankles, and wrists ◦ Skin eruption on the trunk and upper part of the arms or legs ◦ Eruptions that look ring-shaped or snake-like ◦ emotional instability, muscle weakness and quick, uncoordinated jerky movements that mainly affect the face, feet, and hands Acute Rheumatic Fever Kawasaki Disease Once diagnosed… ◦ immediate treatment should be started The recommended initial therapy includes: ◦ IVIG (2 gm/kg) administered as a single infusion over 8 to 12 hours ◦ Aspirin (initial dose of 80 to 100 mg/kg daily divided into four doses). ◦ The AHA and the AAP recommend these two medications for the treatment of acute KD. (Additional agents are used only for children who fail to respond to standard therapy) CARDIOVASCULAR The most common and potentially life-threatening complication of KD is coronary artery aneurysm. The aneurysm is a result of the chronic inflammation of the blood vessels (vasculitis) which causes a weakening in the vessel wall. ◦ The aneurysm can eventually burst leading to internal bleeding or more often, blood clots form in the area leading to occlusion of the coronary artery and myocardial infarction. If untreated, up to 25% of patients with KD develop coronary artery aneurysms. Most aneurysms develop within 6-8 weeks from the onset of illness. If treatment is started within 10 days of the diagnosis, the incidence of coronary artery disease/complications drops to approximately 2%. CARDIOVASCULAR Other possible cardiac complications include: Myocarditis Pericarditis CHF Pericardial effusion Mitral insufficiency Aortic insufficiency Arrythmias LONG TERM CARDIAC SEQUELAE A multi-centre follow-up study was done in Japan obtaining cardiac status on 1594 patients who presented with KD in 1996. Of the 1338 in whom follow up data was available, 10.3% had cardiac sequelae at 1 month and 4.2% at 1 year. The prevalance was greater in males. About 50% of aneurysms regressed within 5 years. The main cause of death in KD is myocardial infarction secondary to thrombosis of an aneurysm or stenosis. GASTROINTESTINAL Diarrhea Vomiting Abdominal pain Hydrops of the gallbladder Elevated liver enzymes Hepatomegaly Acute surgical abdomen NEUROLOGICAL Irritability Aseptic meningitis Transient hemiplegia Cerebral infarction Ataxia Seizures Focal encephalopathy Lethargy Facial palsy RENAL Proteinuria Hematuria Sterile pyuria Echogenic kidneys Renal failure (rare) HEMATOLOGICAL Haemophagocytic syndrome (AKA…Hemophagocytic lymphohistiocytosis (HLH))-a rare condition caused by excess activation and proliferation of macrophages. At this point in time, the exact cause of Kawasaki Disease remains unknown and so it is unknown how to prevent the onset of the disease. Some believe it is caused by a virus or bacteria but this theory has never been proven. It is important, however, to note that when the disease is diagnosed and treatment is initiated in the very early stages, all most all of the complications that were discussed previously can be prevented. Full recovery can be expected for most patients diagnosed with the disease. Patient education about this disease revolves around early recognition of the symptoms as well as seeking treatment as soon as possible. There is a great educational handout on Kawasaki Disease that can be obtained by visiting the American Family Physician website at http://www.aafp.org/afp/990600ap/990600c.html. The handout is copyrighted but permission is given to print and photocopy for nonprofit educational uses. Just a couple tidbits of information found on Kawasaki Disease that may be of interest to some: John Travolta’s son, Jett was diagnosed with Kawasaki Disease at the age of two. There has been some speculation that the vaccine used to help prevent rotavirus infection (RotaTeq) has been linked to development of Kawasaki Disease. ◦ To this date there has not been enough data to support this claim and the CDC continues to support the safety and effectiveness of the RotaTeq vaccine in preventing rotavirus infection. For more information on this visit http://www.cdc.gov/vaccinesafety/vaccines/rotavirus.html. http://www.youtube.com/watch?v=thdcueIequ0&feat ure=player_detailpage ENJOY and THANK YOU! Bulbar conjunctiva (2011). Retrieved from http://www.britannica.com/EBchecked/topic/84026/bulbarconjunctiva Burns, C., Dunn, A., Brady, M., Starr, N., & Blosser, C. (2009). Cardiovascular disorders. In S. Clark (Ed.), Pediatric Primary Care (pp. 758-764). St. Louis, MO: Saunders Elsevier. Celebrity sentry. (n.d.). Retrieved June 30, 2011, from http://www.celebritysentry.com/post/kawasakidisease/ Chin, T. K., & Jung, L. K. (2010, February 25). Pediatric Rheumatic Fever. Medscape. Retrieved from http://emedicine.medscape.com/article/1007946-overview#a0101 Fisman, D. N. (2000, Nov-Dec). Hemophagocytic syndromes and infection. Emerging Infectious Diseases, 6(6). Retrieved from http://www.cdc.gov/ncidod/eid/vol6no6/fisman.htm Jatla, K. K. (2011). Medscape reference. In H. Roy, Sr (Ed.), Ophthalmologic Manifestions of Kawasaki Disease. Retrieved from http://emedicine.medscape.com/article/1197545-overview#aw2aab6b3 KD Foundation. (2010, September 8). Kawasaki Disease [Video file]. Retrieved from http://www.youtube.com/watch?v=thdcueIequ0&feature=player_detailpage Kawasaki disease. (1999, June). American Academy of Family Physicians. Retrieved from http://www.aafp.org/afp/990600ap/990600c.html Kawasaki syndrome and RotaTeq vaccine. (2011, February 8). Centers for Disease Control and Prevention: Vaccine Safety. Retrieved from http://www.cdc.gov/vaccinesafety/vaccines/rotavirus.html Ogershok, P. R. (2009, August 6). Kawasaki Disease. Medscape Reference. Retrieved from http://emedicine.medscape.com/article/330081-overview Porth, C. M., & Matfin, G. (2008). Pathophysiology: Concepts of altered health states (8th ed.). Philadelphia, PA: Lippincott Williams & Wilkins. Sundel, R. (2011, January). Epidemiology and etiology of Kawasaki disease. UpToDate. Retrieved from http://0-www.uptodate.com.topekalibraries.info/contents/epidemiology-and-etiology-of-kawasakidisease?source=search_result&selectedTitle=3%7E150 Tizard, E. J. (2005). Complications of Kawasaki disease. Current Pediatrics, 62-68.