Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Compartmental models in epidemiology wikipedia , lookup
Fetal origins hypothesis wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Public health genomics wikipedia , lookup
Epidemiology wikipedia , lookup
Seven Countries Study wikipedia , lookup
Alzheimer's disease research wikipedia , lookup
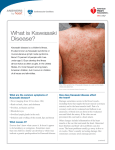
A Pain in the Neck PRESENTED BY: DR. MUNSIF BHIMANI DR. MARIA TAMBAKIS Outline of Presentation Case Presentation Case Discussion Approach to Neck Mass Differential Diagnosis Investigations Course in Hospital Case Complications Treatment Topic Review Topic Summary Case: J.H., a 13-y old boy with neck pain J.H., a 13-year-old boy, presents to the UH Emergency Department in May Chief Complaint: Left neck swelling, tenderness and pain worsening over 1 week Other Symptoms Fatigue/Myalgias Sore throat Spiking Fevers Mild dysphagia/odynophagia 2nd to swelling/neck mass Review of systems Otherwise negative Case: J.H., a 13-year old boy with neck pain Other Historical Questions? Case: Relevant Medical History PMHx: Overall, he has been a well child. Previous Reactive Airway Disease FHx: Mom and dad are both healthy. Maternal hypothyroidism. Sister has celiac disease. Maternal grandfather had RA and dad’s uncle died of cardiac arrhythmia age of 39. Meds: None Allergies: NKDA Immunizations: UTD Case: Physical examination Vitals: Weight- 72 kg, NAD, Afebrile, AVSS Mildly tender, firm left neck mass. No airway concerns. Oral cavity examination and oropharyngeal examination normal Remaining head and neck examination was normal. CVS/RESP/GI N physical exam Neck Mass in a Teenager Differential Diagnosis?? Management?? DDx of Neck Mass Inflammatory Congenital/ Developmental Adenitis Brachial cleft cyst Bacterial (Streptococcus, Thyroglossal duct cyst Staphylococcus) Viral (HIV, EBV, HSV) Fungal (coccidioidomycosis) Parasitic (toxoplasmosis) Cat-scratch disease Tularemia Local cutaneous infections Sialoadenitis (parotid and submaxillary glands) Thyroiditis Mycobacterium avium-intracellulare Mycobacterium tuberculosis Dermoid cyst Cystic hydromas Torticollis Thymic masses Teratomas Ranula Lymphangioma Laryngocele Rosen’s Emergency Medicine DDx of Neck Mass Neoplastic Benign Malignant Mesenchymal tumors (lipoma, Primary tumors Sarcoma Salivary gland tumor Thyroid or parathyroid tumors Lymphoma Metastasis From primary head and neck tumors From infraclavicular primary tumors (e.g., lung or esophageal cancer) fibroma, neural tumor) Salivary gland masses Vascular abnormalities (hemangiomas, AVM, lymphangiomas, aneurysm) Rosen’s Emergency Medicine J.H. Case Management Plan??? J.H. Case Management Plan??? How would you manage this differently if you were in a Community Hospital ED??? Case: Investigations LABS Day 1 WBC 13.3 H HGB 136 MCV 86.7 Plt 290 PMN 10.9 H Lymph 0.7 L Mono 1.6 H Eosino 0.2 What additional investigations would you order? Case: Investigations Blood C + S Sent Throat C+S Sent Monospot Negative Next Step??? Case: Course in Hospital Referred to Peds ER Peds ENT consulted Admitted to hospital for further management of neck mass IV antibiotics started Metronidazole and Cefotaxime Case: Investigations CT Neck Left palatine tonsillitis with reactive lymphadenopathy in the left neck. No definite drainable collections. Throat C+S Group A Streptococcus (Strep pyogenes) NOT isolated. Blood C+S No growth at Day 1 and Day 5 Heterophile Ab (Monospot) Negative Case: Course in Hospital Despite antibiotic therapy: Ongoing neck swelling and pain Ongoing associated spiking fevers J.H. also developed new symptoms: Conjunctivitis Nausea, diarrhea Maculopapular rash on his torso Additional Differential Dx? Investigations? Case: Additional Investigations Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7 WBC 13.3 H 11.6 H 12.8 H 15.9 H 18.6 H 22.1 H 18.4 H HGB 136 135 147 134 137 135 136 MCV 86.7 85.3 85.4 84.9 85.9 86.1 85.7 Plt 290 297 392 382 387 412 H 403 H PMN 10.9 H 16.4 ESR 67 CRP 149.8 H SMA-7 U/A N N H 16.3 H H 75 H 151.4 H N Neg ALT/AST 25/30 Albumin 31 L Case: Course in Hospital • Neck swelling /fatigue improved over 1 week • Remained afebrile over a 48 hour period • J.H. was discharged home on oral Keflex x 2 weeks with • follow-up with ENT in 2 wks. Discharge Diagnosis: Left neck lymphadenitis Associated viral URI Rash secondary to reaction to antibiotic use Return to ER Day 4 Post Discharge Parents concerned about: Weight loss of 20 lbs since start of illness Bilateral conjunctivitis/rash not resolved fully Continued Cervical LAD Additional Questions??? Management Return to ED • Before patient is discharged home, he shows you a new rash on his hands • Diagnostic considerations? Next step? Return to ED • Before patient is discharged home, he shows you a new rash on his hands • Diagnostic considerations? Next step? • Patient is wondering why fingers are now peeling Two Week Follow-Up Visit- ENT ENT noted new desquamation to palms and fingertips Referred back to ID for ??Incomplete Kawasaki disease ID diagnosed J.H with Incomplete KD Started on ASA daily What are the important sequelae of iKD? Sequelae of KD Cardiac Myocarditis and pericarditis Aneurysm Formation with associated SCD, MI, rupture Erythema and edema on the hands and feet Strawberry tongue and lip fissures Hepatic, renal, and GI dysfunction Lymphadenopathy Arthritis Pediatric Cardiology Assessment Physical Exam- N ECG- N Echo Grossly dilated R/L coronary arteries ( >2 cm diameter) with multiple distal coronary aneurysms LVEF= >65% with no regional wall abN to suggest myocardial involvement No valvular AbN Small Pericardial effusion CXR- N Pediatric Cardiology Assessment Diagnosis Incomplete Kawasaki Disease with multiple giant coronary artery aneurysms Treatment suggestions EC ASA 81 mg po OD Case: Additional Complications Referral to Peds Cardiology at SickKids Repeat Echo= LAD clot Admitted for anticoagulation and antiplatelet therapy Discharged on Enoxaparin and ECASA 81 mg po OD CABG (SickKids- Toronto) Ongoing follow-up demonstrating ischemia CABG performed GOALS OF TOPIC REVIEW 1. Clinical suspicion to diagnose KD must be high 2. Features of disease not all present at the same time 3. Incomplete KD exists 4. Treat them early Kawasaki Disease (KD) Mucocutaneous lymph node syndrome is a generalized systemic vasculitis Unknown etiology Complete (or classic) and incomplete disease Peaks at 18 to 24 months Rare below the age of 4 months or after 5 years of age. Younger infants have increased risk for long-term sequelae and sudden death Kawasaki Disease (KD) Incomplete KD (iKD) clinical manifestations are more common in children <1 yr or >5 yr Leading cause of acquired heart disease in children in N.A. High index of clinical suspicion is key for diagnosis Epidemiology of KD Age of Onset Peak incidence at 1 year, mean 2.6 years, uncommon after 8 years. Incidence U.S.A.: 9/100,000 (Caucasian) 32/100, 000 (Asian) Sex Male predominance, 1.5:1. Race In United States: Japanese > blacks > whites. Affects all races worldwide. Epidemiology of KD Etiology Community outbreaks every 2-3 yrs suggest potential transmissible cause. Season Winter and spring in N.A. Geography First reported in Japan, 1961; United States, 1971. Morbidity/Mortality Reported mortality rate of KD is low (0.1 to 0.3 percent) Often secondary to cardiac sequelae. Peak Mortality=15-45 days after onset of fever Classic Kawasaki Disease Fever for 5 days or more plus FOUR of the following symptoms: 1. Bilateral Conjunctival injection (Nonexudative) 2. Changes to the Lips and Oral cavity Erythema, peeling, cracking of lips, "strawberry tongue," or diffuse oropharyngeal mucosa injection 3. Changes of the Extremities Acute: Erythema of palms/soles, edema of hands/feet Subacute: Peeling of finger tips/toes (Weeks 2-3) 4. Rash Polymorphous, diffuse, maculopapular exanthem 5. Cervical adenopathy Greater than or equal to 1.5 cm in diameter, usually unilateral, minimal erythema to skin, non tender LAD Clinical Features of KD NOTE!! Typically all of the clinical features are not present at a single point in time History is key Kawasaki disease is divided into three phases: Acute febrile phase during first 2 weeks of illness Subacute phase from 2 to 4 weeks Convalescent phase from 4 to 6 weeks In most cases, all external clinical manifestations have resolved by 6 weeks. Coronary artery aneurysm development is most prevalent as the fever begins to lessen Manifestations of KD Classic KD Clinical Criteria: Pearls Fever High- Spiking, Remittent with peak temp >39 C Not responsive to antibiotics or antipyretics Lips and Oral Cavity (90% cases) Typically no oral ulcerations or pharyngeal exudates Rash (70 to 90 %) Within 5 days of fever onset Diffuse non-specific maculopapular rash Classic KD Clinical Criteria: Pearls Extremities (50-85%) Acute Erythema/Edema of Palms/Soles Desquamation Conjunctival Injection (>75%) Bilateral Non-Exudative Painless No associated corneal edema/ulcers Cervical LAD (25 to 70 %) Least common feature Occasionally mistaken for Bacterial adenitis Incomplete Kawasaki Disease Fever for 5 days and two to three clinical criteria of classic Kawasaki disease plus C-reactive protein 3.0 milligrams/L and/or erythrocyte sedimentation rate 40 mm/h plus Three or more of the following supplemental labs or positive echo 1. Albumin <3 grams/dL 2. Anemia for age 3. Elevated alanine aminotransferase 3 4. Platelets >450,000/mm after 7 d of fever onset 3 5. White blood cell count >12,000/mm 6. Presence of pyuria (> 10 WBC/HPF) Nondiagnostic Supplemental Lab Criteria 1. Albumin <3 grams/dL 2. Anemia for age 3. Elevated ALT 3 4. Platelets >450,000/mm after 7 d of fever onset 5. White blood cell count 3 >12,000/mm 6. Presence of pyuria (> 10 WBC/ HPF) Incomplete KD: Pearls More common in the extremes of the age spectrum ≤1 y/o or ≥5 to 9 y/o Labs help to increase or reduce the suspicion of KD ESR/ CRP are consistently elevated after day 7 of illness in KD and should prompt echocardiogram iKD diagnosis often based on positive Echo findings suggestive of early coronary arteritis Cardiac Complications • Coronary artery aneurysms or ectasia occur in 15% to 25% of untreated children • May lead to further myocardial infarction, sudden death, or ischemic heart disease • Treatment within 10 days reduces severe aneurysms to <1% Phase of Illness Cardiac Complications Acute (0–2 wk) Myocarditis, pericarditis, coronary arteritis, arrhythmias, valvular regurgitation, LV dysfunction, pericardial effusion Subacute (2–4 wk) Coronary artery aneurysms Convalescent (4–6 wk) Coronary artery aneurysms Risk Factors for Coronary Artery Aneurysm Development Clinical Course Patient Characteristics Laboratory Values Age <1 year old Prolonged fever (>16 d) Hematocrit <35% Male Recurrent fever after 48 h White blood cell count afebrile >12,000/mm3 Cardiomegaly on presentation Platelets >350,000/mm3 C-reactive protein >3 milligrams/dL Albumin <3.5 grams/dL Investigations for KD: Echocardiogram Echo assessment is ideal as it is a non-invasive test Echo is used to assess coronary artery morphology, LV and left valvular function, and the evolution of pericardial effusions Coronary artery aneurysms rarely form before 10 days of illness but may see signs of coronary arteritis in acute KD Aneurysms most commonly involve the proximal LAD/RCA Echocardiogram Echocardiogram is Positive if any conditions are met: Aneursyms are classified by size based on Internal vessel diameter • Small= <5 mm • Medium= 5-8 mm • Large= >8 mm Echocardiogram- Follow-Up Uncomplicated Cases Echo at time of diagnosis 2 weeks 6-8 weeks after onset Follow-up Echocardiograms Progression/Regression of Coronary AbN, evaluate ventricular and valve function, and assess for pericardial effusions Complicated Cases Persistently Febrile, Coronary abN, ventricular dysfunction, pericardial effusion, or valvular regurgitation May need more frequent Echo or additional invasive testing such as angiogram, CT, MRI, and cardiac stress testing Angiogram- Giant Coronary Aneurysms Newburger J W et al. Pediatrics 2004;114:1708-1733 Noncardiac Manifestations of KD System Associated Signs and Symptoms Gastrointestinal Vomiting, diarrhea, abdominal pain, gallbladder hydrops, elevated transaminases, paralytic ileus, mild jaundice Blood Elevated ESR or CRP, leukocytosis with left shift, hypoalbuminemia, mild anemia in acute phase and thrombocytosis in subacute phase (usually second to third week of illness) Renal Sterile pyuria (urethral origin) , proteinuria Respiratory Cough, rhinorrhea, hoarseness, infiltrate on chest radiograph Joint Arthralgia and arthritis Neurologic Mononuclear pleocytosis of cerebrospinal fluid, irritability, facial palsy Skin Perineal rash and desquamation in subacute phase, transverse furrows of fingernails (Beau’s lines) during convalescence Differential Diagnosis of KD Viral infections ( Measles, Adenovirus, Enterovirus, EBV) Scarlet Fever Toxic shock syndrome Staphylococcal scalded-skin syndrome Bacterial Cervical Lymphadenitis Adverse cutaneous drug eruption/hypersensitivity Stevens- Johnson Syndrome Juvenile rheumatoid arthritis Leptospirosis Rocky Mountain spotted fever Erythema multiforme Serum sickness SLE Reactive arthritis syndrome Mercury Hypersensitivity Reaction Treatment of KD Directed at reducing inflammation and preventing cardiac complications. Acute phase Combination of IVIG and high dose ASA Aspirin works synergistically with IVIG to combat acute inflammation, provides symptomatic relief of fever, and may prevent thrombosis of inflamed or dilated coronary arteries Steroids are not routinely indicated but may be useful in refractory cases that do not improve with IVIG. Treatment of KD Patients who develop aneurysms or coronary sequelae are referred to a pediatric cardiologist and/or cardiothoracic surgeon for further management Long-term therapy in individuals who develop coronary aneurysms is aimed at preventing myocardial ischemia or infarction Dependent on severity of disease and aneurysm location/size Treatment of Kawasaki disease ASA Anti-inflammatory (high dose) and antiplatelet (low dose) effects Must use in combination with IVIG to reduce coronary abnormalities Treat with high-dose aspirin (20 to 25 milligrams/kg/dose every 6 hours) Dose is later reduced to 3 to 5 milligrams/kg once daily for 6 to 8 weeks Varied Protocols for when to reduce dose: Afebrile x 48-72 hrs OR Continue until day 14 of illness and > 3-5 days afebrile Treatment of Kawasaki disease IVIG Unknown MOA but likely anti-inflammatory effects Single dose IV immunoglobulin (IVIG) (2 grams/kg over 12 hours) Rapid, symptomatic improvement in 90% of patients and prevents aneurysm formation in 95%. Despite timely therapy, 5% will develop transient CA dilation and 1% develop giant aneurysms IVIG may be readministered for persistent symptoms Treatment of Acute Complications Coronary Thrombosis/AMI Promoted by sluggish flow within dilated aneurysm and occurrence of stenotic lesions at proximal and distal ends Differs from typical adult acute thrombosis related to plaque rupture Treatment often aimed at targeting multiple steps in coagulation cascade May benefit from interventional and surgical techniques in acute and progressive CAD Cardiology: Long Term Follow-Up Children without cardiovascular abnormalities treated fully in the acute and subacute phase appear to be clinically asymptomatic 10 to 21 years later CA dilatation <8 mm generally regresses over time Most smaller aneurysms fully resolve by echo Patients with giant aneurysms are at the greatest risk for myocardial infarction resulting from CA occlusion Long-Term Management in Kawasaki Disease Risk Level Definition Management Guidelines I No coronary artery changes at No ASA is needed beyond the subacute phase (6– 8 wk). No P.A. restrictions > 6–8 wks. No followany stage of the illness up beyond the first year. II Transient ectasia of coronary Same as above, or clinical follow-up ± ECG every arteries during acute phase 3–5 y. No P.A. restrictions >6–8 wks. III Single small to medium coronary aneurysm IV Giant aneurysm or multiple small to medium aneurysms without obstruction V Coronary artery obstruction ASA until abnormality resolves. Annual follow-up with ECG and echo if < 10 y and every other-year stress testing if > 10 y. P.A. restrictions guided by stress testing. Long-term ASA ± warfarin. Annual follow-up with ECG, echo, and stress testing. P.A. restrictions guided by stress testing. No contact sports. Angio. Long-term ASA ± warfarin ± calcium channel/beta blocker to reduce myocardial oxygen consumption. Echo and ECG every 6 mo. Stress testing and Holter examination annually. P.A. restrictions as above. Angiogram. Incomplete KD Algorithm- Does it work?? KD with isolated cervical lymphadenopathy Case series Initial presentation of only fever and cervical LAD at the time of admission. These patients tended to be older and to have a more severe course, with increased risk of coronary artery disease and lack of response to IVIG Thus, certain presentations may be associated with a worse prognosis Incomplete KD- Delayed Diagnosis Incomplete KD should not be equated with mild KD (Sonobe et al., 2007) Literature suggests that patients with Incomplete KD are more likely to develop coronary artery abnormalities, probably because they are less likely to be diagnosed expeditiously 14.2 % in Complete KD vs. 18.4 % in Incomplete KD Repeated histories and physical examinations are important for: Diagnosis of KD Consideration of alternative diagnoses Kawasaki Disease: Summary KD is a systemic illness characterized by fever, conjunctivitis, mucositis, rash, extremity changes, and cervical lymphadenopathy. Patients who lack a sufficient number of findings to fulfill the classic criteria may have incomplete KD No laboratory or cardiac studies are included among the classic diagnostic criteria for KD, but certain findings characteristic of KD may support the diagnosis in ambiguous cases Kawasaki Disease: Pearls Must consider KD in the DDx of a child with unexplained fever for 4-5 days that is associated with any clinical features of KD History is Key Features often do not occur at the same time so must ask if clinical criteria have been present When entertaining the diagnosis of possible iKD, using the algorithmic approach and consulting a specialist is advised Early treatment of KD with IVIG and high dose ASA can drastically reduce the likelihood of development of cardiac complications References 1. . Anderson MS, Todd JK, Glode MP. Delayed diagnosis of Kawasaki syndrome: An analysis of the problem. Pediatrics. 2005; 115 (4): e428 2. Barone SR, Pontrelli LR, Krilov LR. The differentiation of classic Kawasaki disease, atypical Kawasaki disease, and acute adenoviral infection: use of clinical features and a rapid direct fluorescent antigen test. Arch Pediatr Adolesc Med. 2000;154:453–456. 3. Council on Cardiovascular Disease in the Young; Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease; American Heart Association. Diagnostic guidelines for Kawasaki disease. Circulation. 2001;103:335–336 4. Minich LL, Sleeper LA, Atz AM, et al. Delayed diagnosis of Kawasaki disease: what are the risk factors? Pediatrics. 2007;120(6):e1434. References 5. Newburger JW, Takahashi M, Gerber MA, et al: Diagnosis, treatment, and long- term management of Kawasaki disease: A statement for health professionals from the Committee on Rheumatic Fever, Endocarditis and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Circulation 2004 Oct 26;110(17):2747–2771. 6. Sundel, R. Kawasaki disease: Clinical features and diagnosis. In: UpToDate, Tepas, E (Ed), UpToDate, Waltham, MA, 2013. 7. Sundel, R. Kawasaki disease: Epidemiology and etiology. In: UpToDate, Tepas, E (Ed), UpToDate, Waltham, MA, 2013. 8. Sundel, R. Incomplete (atypical) Kawasaki disease. In: UpToDate, Tepas, E (Ed), UpToDate, Waltham, MA, 2013 References 9. Sundel, R. Kawasaki disease: Initial treatment and prognosis. In: UpToDate, Tepas, E (Ed), UpToDate, Waltham, MA, 2013 10. Tintinalli, JE (Eds). Pediatric Heart Disease: Acquired Heart Disease. In: Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 7e. McGrawHill Education, 2011. 11. Yellen ES, Gauvreau K, Takahashi M et al. Performance of 2004 American Heart Association recommendations for treatment of Kawasaki disease. Pediatrics. 2010;125:e234–e241 12. Yu, JJ. Diagnosis of incomplete Kawasaki disease. Korean J Pediatr. 2012 March; 55(3): 83–87. 2D Echocardiogram Newburger J W et al. Pediatrics 2004;114:1708-1733