Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Orthohantavirus wikipedia , lookup
Meningococcal disease wikipedia , lookup
Typhoid fever wikipedia , lookup
Chagas disease wikipedia , lookup
Onchocerciasis wikipedia , lookup
Rocky Mountain spotted fever wikipedia , lookup
Marburg virus disease wikipedia , lookup
Schistosomiasis wikipedia , lookup
Oesophagostomum wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Visceral leishmaniasis wikipedia , lookup
Leishmaniasis wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
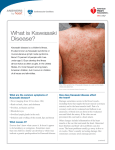
Kawasaki Disease Dr Paul A Brogan Senior Lecturer in vasculitis Department of Rheumatology ICH/GOSH [email protected] Overview • • • • • • History and Epidemiology Clinical features Pathogenesis Treatment Outcome Research at GOSH: Long term KD follow up study What time is dinner? The first case of Kawasaki disease: London 1870 A C B Epidemiology KD epidemiology • • • • • World wide distribution Male preponderance Commoner in oriental children Some seasonality and occasional epidemics The incidence of KD is rising world-wide, including the UK. – Incidence in the UK is 8.1 /100 000 children aged less than 5 years old Epidemiology Japan: – Incidence 220 per hundred thousand children under the age of five – peak age onset 9-11 months – 70% of all cases younger than 3 years – 240 00 cases in Japan – Increased cases in winter – Epidemics moving from adjoining region – Risk higher in siblings of index cases Hawaii Mean 40 per 100 000 – – – – – 360 for Japanese 95 for Chinese 77 for Hawaiians 56 for Filipino 7 for Caucasians Race-specific incidence of Kawasaki disease Davis RL , Waller PL , Mueller BA , et al. Kawasaki syndrome in Washington State. Race-specific incidence rates and residential proximity to water. Arch Pediatr Adolesc Med 1995; 149:66-69 Rising incidence of Kawasaki disease in the UK Incidenc e 8/100 000 Harnden A et al. BMJ 2002; 324: 1424-1425 Clinical features Kawasaki disease - AHA diagnostic criteria Fever of 5 days duration + four of five criteria 1. Oropharyngeal changes 3. (90%+ of cases) 2. Changes in peripheral extremities Bilateral non-purulent conjunctival injection (90%+ of cases) 4. Polymorphous rash (95%+ of cases) (90%+ of cases) 5. Cervical lymphadenopathy (~75% of cases) KD differential diagnosis 1. 2. 3. 4. Toxic shock syndrome (streptococcal and staphylococcal) Staphylococcal scalded skin syndrome Scarlet fever Infection with viruses enterovirus, adenovirus, measles, parvovirus, Epstein–Barr virus, cytomegalovirus 5. 6. 7. 8. Mycoplasma pneumoniae Rickettsiae Leptospirosis The differential diagnosis of IVIG (intravenous immunoglobulin) resistant KD includes polyarteritis nodosa, systemic onset juvenile idiopathic arthritis, and malignancy (particularly lymphoma). The cause of KD is… … nature & nurture Genetics Genetics of KD KD is polygenic • • • • • • • • • • Mannose binding lectin: ambiguous role ACE MMP TNF alpha (IVIG resistance) IL-10 promoter Chemokines (CCR5) IL-18 promoter (Taiwanese) IL 1 beta- no association eNOS/iNOS not associated with CAA in Japanese Fc gamma so far not associated No infectious cause yet found For and against Superantigens in KD Studies against Studies for Seroconvert (IgG and IgM) for SAgs (Matsubara et al 2006, CEI) T cell activation consistent with SAg mediated disease (Brogan et al 2008, CEI) A new RNA virus? Rowley et al PIDJ 2011 Treatment Treatment • IVIG 2g/kg over 12 hours • Aspirin 30-50 mg/kg/day (4 divided doses) – Then 2-5 mg/kg/od 48 hours after fever settles • Fever recrudescence/IVIG resistance: – Repeat IVIG – OR corticosteroids – OR Infliximab Recent developments in KD Rx Corticosteroids as adjunctive first line Rx? • Inoue Y et al. A multicenter prospective randomized trial of corticosteroids in primary therapy for Kawasaki disease: clinical course and coronary artery outcome. 2006; J Pediatr; 149: 336-341 – Prospective RCT of 178 patients – Fewer CAA at 1 month in those receiving IVIG AND prednisolone (11.2% versus 2.4%) Corticosteroids as adjunctive first line Rx? • Newburger JW et al. Randomized trial of pulsed corticosteroid therapy for primary treatment of Kawasaki disease. NEJM 2007; 356: 663-675 – No effect on CAA Rationale for blocking TNF-α in KD • Murine model of KD: – Production of TNF- α in the peripheral immune system – Response site directed, migration to the coronary arteries – Mice treated with etanercept and TNFRI knockout mice resistant to development of both coronary arteritis and coronary aneurysm formation. Hui-Yuen JS et al J Immunol. 2006;176:6294-301 Evidence for infliximab • Burns JC et al 2005 J Pediatr 2005; 146:662–667. – 13 patients with IVIG resistant KD, good response • Burns JC et al 2008 J Pediatr 2008; 153:833–838 – 24 patients 2nd IVIG vs infliximab (non inferior) • Case reports: – O‘Connor MJ, Saulsbury FT. Incomplete and atypical Kawasaki disease in a young infant: severe, recalcitrant disease responsive to infliximab. Clin Pediatr 2007; 46:345-8 – Zulian F et al. Efficacy of infliximab in long-lasting refractory Kawasaki disease. Clin Exp Rheumatol. 2006; 24: 453 – Brogan RJ et al Pediatr Rheumatol Online J. 2009 Jan 21;7:3. Infliximab • Chimeric monoclonal antibody against TNFα • Dose 6mg/kg IV • ?repeat after 2 weeks if ongoing inflammation (consider differential diagnosis) KD outcome • 25 % CAA untreated • 4-9% CAA with IVIG and aspirin • IVIG resistance 15-20% – V high risk of CAA: 20-30% • The acute mortality rate due to myocardial infarction <1% Follow up • Stop aspirin if echo at 6/52 normal • Continue if CAA present • Giant aneurysms (>8mm) never resolve: – Aspirin and warfarin (heparin until INR 2-3) • Long term follow up Prognosis for those with giant CAA (>8mm) • 76 patients from 1972 • Median observational period 19 years • 61% required surgical coronary intervention – At one month to 21 years – Mode time of intervention: one month • Survival rate: – 10 yrs: 95% – 20 yrs: 88% – 30 years: 88% Suda et al 2011 Circulation Does KD cause premature atherosclerosis? GOSH KD follow up study Hypothesis: KD predisposes to premature atherosclerosis (or vasculopathy) in UK patients We are studying: 1. Subclinical endothelial injury 2. Sub-clinical inflammation 3. Arterial stiffness (vicorder PWV) 4. Carotid intimal medial thickness Years after KD Take home messages • HSP and KD are the commonest paediatric vasculitides • KD still kills children- limited window of opportunity to influence outcome: switch off the inflammation ASAP – Earlier use of steroids and infliximab ie after 1 dose of IVIG • Polygenic and no infectious cause yet found • Does KD predispose to premature atherosclerosis?













































![2014 Jun 13. pii: ciu449. [Epub ahead of print] Clinical efficacy](http://s1.studyres.com/store/data/004659563_1-cbbffe8299af8775d28fa21caafaf24f-150x150.png)

