Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Heart failure wikipedia , lookup
Saturated fat and cardiovascular disease wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Cardiovascular disease wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Cardiac surgery wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Infective endocarditis wikipedia , lookup
Electrocardiography wikipedia , lookup
Myocardial infarction wikipedia , lookup
Coronary artery disease wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
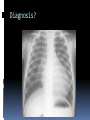
Gavin Burgess R5, PEM PAEDIATRIC EMERGENCY CARDIOLOGY General Review common presentations Uncommon Paediatric ECG Congenital heart disease Rhythm disturbances Long QT HOCM Rheumatic fever Carditis – myo, endo, peri General Innocent murmurs Kawasaki disease Fetal circulation “Normal” Age Respiratory rate Pulse rate Systolic BP O-1mo 30-60 120-160 50-70 1-12mo 20-40 80-140 70-100 1-5y 20-30 80-130 80-110 6-12y 20-30 70-110 80-120 adolescents 12-20 60-100 110-120 “Normal” Ball-park BP? Neonate? Older? “Normal” Gestational age should equal MAP Systolic BP = 70 + (2 x age) “Normal” ECG Typically have shorter PR, QRS, QT RV dominance, RAD RVH Causes Tetralogy of Fallot PS Coarct ASD TAPVD Large VSD with Pulm HT LVH Causes AS VSD PDA Complete AV block Cardiomyopathy Diagnosis? Superior or “north west” axis Endocardial cushion defect 2% of congenital heart disease Down syndrome account for 70% Fatal due to pulm HT Banding in infancy Myocardial infarction AT III Cardiomyopathy Congenital heart disease CAD (ALCAPA) Drugs (cocaine) Homocystinuria Hyperlipidaemia and cholesterolaemia Kawasaki Leukaemia Marfans Haemoglobinopathies Tumours (myxoma) Rheumatic fever SLE Diagnosis? Diagnosis? Diagnosis? Which lesions give cyanosis? Tetralogy of Fallot Tricuspid atresia Transposition of the great arteries (IDM) Truncus arteriosus Total anomalous pulmonary venous drainage Hypoplastic left heart Ebstein’s anomaly (lithium) Pulmonary atresia/severe stenosis Pulmonary markings Decreased: Pulmonary atresia/stenosis Tetralogy Tricuspid atresia Ebstein’s anomaly Increased: TGA TAPVD Truncus What’s the hyperoxia test? ABG Give 100% O2 Repeat ABG after 10 min If rises by >10%, likely pulmonary lesion When does the ductus close? 10-14 days after birth, it is physiologically closed Neonatal and infant presentations to ED What are the 4 presentations in and infants neonates? 1) shock 2) cyanosis 3) cardiac failure 4) murmur What are the ductaldependent lesions? Systemic Coarct/interrupted arch Aortic stenosis HLH Pulmonary PS/atresia Tricuspid atresia Shock L ventricular outflow obstruction Coarct AS HLH Shock Management: ABC’s Start prostin CXR ECG What’s prostin? Prostaglandin E1 Rate 0.05-0.2 mcg/kg/min Side effects? Apnoea Fever Flushing Hypotension Prostin has an “all or nothing” action Should work in 15min Time to presentation of cyanotic lesions Age ECG X-ray 0-1 week TGA RVH Increased 1st week TAPVD RVH Increased 1-4weeks Tricuspid Atresia LVH Decreased Severe PS RVH Decreased 1-12weeks TOF RVH Decreased Anytime in infancy Truncus arteriosus BVH Increased Cyanosis What is a tetralogy of Fallot? RVH Overriding aorta VSD RV outflow obstruction What’s a “tet spell”? Change in the balance of pulmonary and systemic flow Hypoxic and cyanotic event Decreased system vascular resistance or increased RV outflow obstruction Increasing hypoxia How do I treat it? O2 Chest-knee (why?) Analgesia B-blocker (why?) Cardiac failure History: Fussy Sweating FTT Short frequent meals Physical: HSM Murmur FTT You will NOT see a JVP AVM – auscultate the head Murmurs Features of an innocent murmur 80% of children will have a murmur at some time in their lives All have normal ECG and X-rays Never diastolic Common innocent murmurs Type Description Age Still’s LLSB, 2/6, “twang” 3-6y Pulmonary flow ULSB, blowing, transmits Gone in 3-6mo Venous hum Supra clavicular, rotate head, supine goes 3-6y Carotid bruit Over carotid Any age Arrhythmia SVT Very common Tolerated well, occasional LOC change Child is fussy Newborn >220 bpm <12y often accessory pathway Arrhythmia SVT treatment In shock vs stable Vagal stim Adenosine Amiodarone ,verapamil use extreme caution. Frequently develop profound hypotension and die Arrhythmia Long QT History Deafness Single person MVC Swimming syncope Exercise syncope Family history of sudden death Seizure of unknown etiology Recurrent syncope/lightheadedness Sibling with SIDS Physical Infant with bradycardia Arrhythmia All first degree family members should be screened with ECG HOCM 2% under 2 y, 7% under 10y Variable history CP Palpitations SOB Syncope Sudden death High risk if syncope Sudden death with strenuous exercise HOCM Physical S4 gallop, mid systolic murmur Increased PVR decreases murmurs Rheumatic fever Who was Jones? What where his criteria? What do you need to make a diagnosis? Which valve? Then? Rheumatic fever What about Sydenham’s chorea? And the rash? Rheumatic fever Treatment ASA 75-100mg/kg Prednisone 1-2mg/kg Benzathine (Pen G) 600 000U (27kg), 1.2 million U (27kg) Prophylaxis Age questioned Myocarditis Various causes, most notably viral Coxsackie A,B, ECHO, flu’ Non-specific viral prodrome Non-specifc fussiness, lethargy etc Heart failure IVIG may be indicated Infective endocarditis Rheumatic fever, congenital heart defects, catheters, IVD S. aureus, viridans are the usual suspects Fungi in neonates, usually in the NICU Infective endocarditis Major 2 + BC, (viridans, s. bovis, HACEK, S. aureus, enterococci Persistently + BC (1 hr between multiple, or 12h or 3h +) + echo mass at typical sites Intracardiac abscess Prosthesis failure New regurgitant murmur Infective endocarditis Minor Fever (38C) Predisposing condition/IVD Vascular phenomena Non-specific echo findings Prophylaxis -1997 High risk – amp and gent Prosthesis Previous IE Complex CHD Surgical systemic-pulmonary shunts Medium risk - amp Other congenital heart malformation Acquired valve dysfunction HOCM MVP Negligible risk – no Rx Isolated secundum; repaired ASD, VSD, PDA; bypass graft; MVP (no regurge); “innocent” murmurs; KD with normal valves; RF with no valve dysfunction; pacemakers Prophylaxis High risk Prosthesis Previous IE Transplants Complex CHD Dropped from the list……. Moderate risk (PDA,VSD,primumASD,coarct,bicuspidAV) Calcified AS,RF,HOCM,MVP Pericarditis Classic chest pain worse when lying flat Radiation to L shoulder Friction rub Most often viral causes Diffuse ST changes, “saddle”shaped CXR important Cefotaxime, ASA, prednisone, colchicine Kawasaki disease Etiology unkown, presumed infectious More common in Asian and Pacific islanders Peaks around 1-2years, 80% under 4y, 50% under 2y Slight male preponderance 3mo-8y is typical range Kawasaki disease 3 phases Acute phase (10 days) High fever for 5 days 4 of rash (ANY rash, no bullae/vesicles), oedema of extremities/ peeling of extremities Non-exudative bulbar conjuctivitis Mucosal changes (cracked lips, strawberry tongue – even on HISTORY) Cervical LN (1.5cm) Carditis, other organs (arthritis, pyuria, gallbladder/liver, menigitis, irritable Kawasaki disease Acute ESR, CRP WCC, plt Lipids, LFTs Echo coronary artery aneurysms unusual before 10d Subacute phase Desquamation Coronary disease Rash, fever, LN disappear plt Kawasaki disease Convalescent phase ESR, plt normalise Beau’s lines Kawasaki disease Rx IVIG ASA Vaccinations Steroid of no benefit Reduces CAD from 25% to 5% Untreated mortality 1-5%