Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
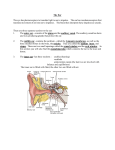
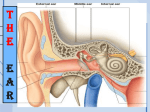
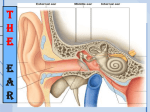
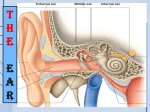
LEC:1 E.N.T عماد ناظم الكواز.د 16/3/2017 EAR Anatomy The ear can be divided anatomically and clinically into three parts; the external, the middle and the inner ear. The external and the middle ears are concerned primarily with the transmission of sound. The inner ear functions both as the organ of hearing and as part of the balance system of the body. The External Ear It consist of the auricle (pinna) and the external auditory meatus (EAM). The auricle consist of a skeleton of yellow elastic cartilage ( except the lobule which is composed of fat) covered with a skin and attached to the side of the head by ligaments and functionless anterior, superior and posterior auricular muscles. The external auditory meatus measures 24mm in adults. It is composed of two portions; an outer cartilaginous 1/3 about 8mm long and an inner bony 2/3 16mm long. The sebaceous glands, ceruminous glands and hair follicles are present only in the cartilaginous portion. Owing to the closer union of cartilage and skin, any inflammatory lesion such as boil in the cartilaginous meatus is an acutely painful infection. The epithelium lining the bony meatus is much thinner and is devoid of those structures which characterize the thicker skin of the outer canal. The general direction of the cartilaginous meatus is medially, upwards and backwards, while that of the bony meatus is medially, downwards and forwards. The meatus may be partially straitened in adults by pulling the auricle upwards, outwards and backwards. There are two constrictions in the EAM; one at the junction of the cartilaginous and bony part and the other is in the osseous part. Nerve Supply of the external Ear 1. Auriculotemporal nerve (V). 2. Auricular branch of the vagus (Arnold). 3. Lesser occipital nerve (C2). 4. Greater auricular nerve (C2C3). The Tympanic Membrane (Ear Drum) The tympanic membrane separates the EAM from the middle ear. It is thin, nearly oval disk, forming an angle of about 55 with the floor of the meatus. The TM has an outer layer of squamous epithelium continuous with that of the meatus, a middle layer of fibrous tissue and an inner layer of mucous membrane continuous with the lining of the middle ear. The TM is supported around its periphery by a fibrous thickening known as the annulus. The fibrous annulus in turn fits into a slot in the tympanic bone called the sulcus. Landmarks of the ear drum The tympanic membrane has a pearly grey colour with a triangular bright area, the cone of light, extending from the centre (umbo) downwards and forwards. The most prominent landmark is the handle of malleus, at its upper end lie a small projection known as the lateral process. The anterior and posterior mallear folds stretch from the lateral process and the part of drum above this level constitutes the pars flaccida. The TM is divided into two parts; the pars tensa and the pars flaccida. The latter forms the upper most part of the TM where the fibrous layer is absent and frequently referred to as the attic part of the ear drum. Chronic perforations of this area are potentially unsafe. The Nerve Supply of the outer surface of the TM is similar to that of the EAM. The inner surface is supplied by the tympanic branch of the IX (Jacobson nerve) The Blood supply is by the postauricular and maxillary arteries. Middle Ear Cleft The middle ear cleft includes the Eustachian tube, the middle ear and the aditus which leads posteriorly to the mastoid antrum and air cells. I. The Eustachian Tube The ET connects the tympanic cavity with the nasopharynx and in the adults is about 36mm in length. In infants the tube is shorter, wider and its course is more horizontal than adults hence acute SOM is common in this age. The tube has two parts, an upper bony portion which forms 1/3 of its length and a lower cartilaginous portion forming the remaining 2/3. The tube is closed at rest but is opened on yawning or swallowing by contraction of the tensor palati muscle and thus equality of air pressure is maintained on both sides of the TM. II. Middle Ear (Tympanic cavity) The cavity may be described as six-sided box frequently linked in shape to a match box. Roof; is formed by a thin pate of bone (tegmen tympani). This plate separates the tympanic cavity and mastoid antrum from the middle cranial fossa. Injury of the tegmen tympani leads to CSF otorrhea. Floor; a thin plate of bone separates the cavity from the bulb of the internal jugular vein. Posterior wall; contains an opening high up which is known as the aditus connecting the tympanic cavity with the mastoid antrum which communicates with mastoid air cells. Just below the aditus is a small projection of bone, the pyramid, which contains the stapedius muscle. The tendon of this muscle passes forwards to its insertion in the neck of the stapes Anterior wall; a thin plate of bone separates the cavity from the internal carotid artery. The anterior wall has two openings; one being the Eustachian tube which connects the tympanic cavity with the nasopharynx. Above it is the canal for tensor tympani muscle which is inserted into the neck of malleus. Lateral wall; is the TM. Medial wall: The promontory which is the bony covering of the basal turn of the cochlea. The facial nerve runs horizontally superior to it enclosed in a thin bony canal (canal of Fallopius) which is sometimes deficient. Posteroinferior to the promontory is the round window whereas, posterosuperior to the promontory is a somewhat similar opening; the oval window; which is occupied by the footplate of the stapes. Contents 1. Air. 2. Ossicles: Malleus, incus and stapes. The handle of malleus is firmly embedded in the middle layer of the TM and its head articulates with the body of the incus. The long process of the incus articulates with the stapes which in turn occupies the oval window. 3. Muscles: Tensor tympani and stapedius. The former tenses the tympanic membrane. The latter comes into action reflexly in response to loud noise and this serves to stiffen up the conducting mechanism and possibly to protect the inner ear against damage. 4. Nerves: a. Chorda tympani: Arises from the facial nerve in the Fallopian canal. b. Tympanic plexus: Lies on the promontory. It's formed by the tympanic branch of the 9th nerve (Jacobson) and branches from the sympathetic plexus. This plexus supplies the lining mucosa of the ET, tympanic cavity and mastoid air cells. The Inner Ear The inner ear lies within the petrous part of the temporal bone. It is called the labyrinth (from it's complexity) and it consist of a membranous labyrinth enclosed in a bony labyrinth (otic capsule). The membranous labyrinth contains fluid known as endolymph which is similar to the intracellular fluid. The space within the bony labyrinth between it's wall and the membranous labyrinth contains another fluid known as perilymph. The composition of the perilymph is very similar to the extra cellular fluid. The Bony Labyrinth 1. Anteriorly;lies a snail like cochlea. 2. In the middle; lies the vestibule. The fenestra ovale (oval window) is situated on it's lateral wall and is closed by the footplate of the stapes. 3. Posteriorly;lie three semicircular canals. The Membranous Labyrinth 1. The membranous cochlear duct; is situated in the bony cochlea. The neuroepithelium of the cochlea is arranged along the entire length of the cohlear duct and is known as the organ of Corti.Nerve fibres from the organ of Corti pass centrally as the cochlear nerve. 2. Saccule and utricle; lie in the bony vestibule. Saccule and utricle are stimulated by linear acceleration. 3. The membranous semicircular canals (SCC); occupy the corresponding bony canal and are set at right angles to each other, each represent a plane in space. The stimulus which excite the SCC is angular acceleration. The SCC, utricular and saccular nerves unite to form the vestibular nerve. The vestibular and cochlear nerves together constitute the 8th cranial nerve. Blood Supply The main supply comes from the labyrinthine artery (internal acoustic artery) which arises from the basilar or anterior inferior cerebellar artery. Facial Nerve The nerve emerges the pons and after crossing the cerebellopontine angle it enters the temporal bone at the internal auditory meatus. It passes over the labyrinth until it reach the medial wall of the tympanic cavity. Here it bends backwards at right angle where the geniculate ganglion is situated and passes almost horizontally, enclosed in the Fallopian canal, above the oval window. When it reaches the aditus it turns downwards behind the pyramid and continues almost vertically till it emerges from the stylomastoid foramen. The nerve to the stapedius is given off close to the pyramid. The chorda tympani nerve leaves the descending part of the facial nerve and enters the tympanic cavity. Physiology of Hearing Mechanism of Hearing The auricle collects the sound waves and they pass along the EAM to the TM. The vibration of the TM is transmitted to the malleus, incus then to the stapes in the oval window causing vibration to set up in the endolymph and perilymph. This stimulates the hair cells of the organ of Corti. Its these hair cells which convert the mechanical energy into electrical impulses which travel along the auditory nerve. Symptoms of ear disease 1. Hearing loss ( Deafness) : It may be conductive, sensorineural or mixed. In CHL the sound appears quieter but it is not distorted. Sound and speech are well heard when amplified. In some cases the patient may hear better in the presence of background noise e.g. railway carriage or bus. This is called paracusis Willisii and it is found most typically in otosclerosis. It results from the fact that in these places people with normal hearing raise their voice to overcome the background noise. In otosclerosis, patients don't hear the background noise which is usually a low-frequency sound. The quality of speech is well maintained because the patient hears his own voice clearly (by bone conduction). In SNHL the sound not only seems quieter but it is distorted as in majority of cases the higher frequencies are more affected than the lower, leading to difficulty in hearing the consonant sounds which are so important for speech discrimination. In severe SNHL the patient does not hear his own voice and leads to speech which is indistinct or expressionless. Tinnitus is commonly associated with SNHL. Common Causes of conductive hearing loss Impacted wax, secretory otitis media, chronic suppurative otitis media, otosclerosis. Common Causes of Sensorineural hearing loss Congenital hearing loss: ( Deaf Mute if bilateral) Ototoxic drugs: e.g. aminoglycoside, furosemide, aspirin, quinine, cytotoxic drugs. Aging: hearing loss is symmetrical, and usually progressive (Presbycusis) Infection: Mumps deafness is unilateral, measles: bilateral Endolymphatic hydrops: Meniere's disease ( vertigo + deafness + tinnitus ) Noise-induced hearing loss, Acoustic trauma 2. Discharge( Otorrhea) : Serous discharge; Otitis externa. Mucopurulent discharge, foul smell long duration: chronic suppurative otitis media. Unilateral watery discharge following head injury or aural surgery: CSF otorrhea. It occurs as a result of damage to tegmen tympani. Bloody discharge; due to granulation tissue in chronic suppurative otitis media or due to malignant disease. 3. Pain (Otalgia) : It arises within the ear (otogenic or primary) or outside the ear (referred otalgia) . Earache can be referred to the ears in the following ways: 5th cranial nerve; diseases of the upper and lower molars, dental 1/ extraction and temporomandibular joint (TMJ) problems. 2/ Jacobson (auricular branch of 9th) and Arnold (auricular branch of 10th) nerves; pharyngeal causes of otalgia include acute tonsillitis, tonsillectomy, ulcers in the mouth and pharynx, malignant disease of the nasopharynx, oropharynx, and hypopharynx. Glossopharyngeal neuralgia is a primary neuralgia causing intermittent agonizing paroxysms of pain affecting base of tongue, fauces and ears. 3/ 2nd and 3rd cervical spinal nerves (lesser occipital and greater auricular) : intervertebral disc disease and cervical spondylosis. DIFFERENTIAL DIAGNOSIS OF EAR PAIN Otogenic: External auditory canal:, otitis externa, trauma (e.g. cotton bud A. abuse), auricular haematoma, foreign body. Middle ear: acute otitis media, bullous myringitis, CSOM. B. Referred Otalgia: A. Oropharynx (IX nerve): tonsillitis/post-tonsillectomy, carcinoma of post. 1/3 of tongue B. Laryngopharynx (X nerve): pyriform fossa tumor. C. Molar teeth, TMJ, parotid gland ( V nerve). D. Cervical spine (C2, C3): pain is often worse at nigh 4. Tinnitus: It is a subjective sensation of sound in the ear or head in the absence of any relevant external signals. (Occasionally it is objective e.g. in palatal myoclonus and glomus tumors). It is regarded as a symptom of irritation of the cochlea or auditory pathways. Tinnitus may be met with any form of ear disease and is commonly associated with SNHL, and is also a symptom of some general diseases which indirectly affect the ear through the circulation. It is a common symptom of anaemia, thyrotoxicosis, hyperdynamic circulation, renal failure and some intracranial tumors. It may be caused by ototoxic drugs, such as quinine, salicylates and aminoglycoside. 5. Vertigo: It is defined as hallucination of movement or subjective sense of imbalance. Vertigo is considered as a symptom of irritation of the vestibular apparatus and it must be differentiated from conditions such as fainting, dizziness, drop attack and postural hypotension. Vertigo may be central in origin (cerebellum), or peripheral (labyrinth /vestibular nerve). Peripheral lesions tend to produce intense vertigo of sudden onset. Nausea and vomiting are common (which indicate severe vertigo). Central lesions -on the other handproduce less intense vertigo. Positional changes have less effect, but the patient tends to have more disturbance of gait.