Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
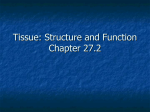
A B 50 µm 20 µm C D 20 µm 20 µm Figure 2. Histopathological analysis. A, Cytologic preparation from anterior chamber aspirates. Arrows indicate mononuclear epithelioid cells with abundant cytoplasm (Wright Giemsa). B-D, Histopathological specimens from the retrocorneal membrane. B, Descemet membrane and fibrous, retrocorneal membrane (hematoxylin-eosin). C, Diffuse positive staining with smooth muscle actin. D, Diffuse positive staining with CK7. partment of Pathology and Laboratory Medicine (Dr Yeaney) and Flaum Eye Institute (Dr Hindman), University of Rochester School of Medicine and Dentistry, Rochester, New York. Correspondence: Dr Hindman, Flaum Eye Institute, 601 Elmwood Ave, Box 659, Rochester, NY 14642 (holly [email protected]). Author Contributions: Dr Hindman had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Conflict of Interest Disclosures: None reported. Funding/Support: This work was supported by grant K23EY019353 from the National Eye Institute, National Institutes of Health. Additional Contributions: Flaum Eye Institute’s Diagnostic Imaging Service obtained the clinical images. 1. Vargas LG, Vroman DT, Solomon KD, et al. Epithelial downgrowth after clear cornea phacoemulsification: report of two cases and review of the literature. Ophthalmology. 2002;109(12):2331-2335. 2. Chen SH, Pineda R II. Epithelial and fibrous downgrowth: mechanisms of disease. Ophthalmol Clin North Am. 2002;15(1):41-48. 3. Haller JA, Stark WJ, Azab A, Thomsen RW, Gottsch JD. Surgical management of anterior chamber epithelial cysts. Am J Ophthalmol. 2003;135(3): 309-313. 4. Lai MM, Haller JA. Resolution of epithelial ingrowth in a patient treated with 5-fluorouracil. Am J Ophthalmol. 2002;133(4):562-564. 5. Shaikh AA, Damji KF, Mintsioulis G, Gupta SK, Kertes PJ. Bilateral epithelial downgrowth managed in one eye with intraocular 5-fluorouracil. Arch Ophthalmol. 2002;120(10):1396-1398. 6. Chiou AG, Kaufman SC, Kaz K, Beuerman RW, Kaufman HE. Characterization of epithelial downgrowth by confocal microscopy. J Cataract Refract Surg. 1999;25(8):1172-1174. 7. Jakobiec FA, Bhat P. Retrocorneal membranes: a comparative immunohistochemical analysis of keratocytic, endothelial, and epithelial origins. Am J Ophthalmol. 2010;150(2):230-242, e2. Chromoblastomycosis of the Conjunctiva Mimicking Melanoma of the Ciliary Body C hromoblastomycosis is a chronic subcutaneous mycosis that typically involves the lower extremities. The vast majority of causative microorganisms have melanized cell walls (ie, are dematiaceous fungi) and belong to 4 genuses of saprophytic fungi: Phialophora, Fonsecaea, Rhinocladiella, and Cladophialophora.1,2 Most human infections can be traced to traumatic implantation. We describe a unique case of conjunctival chromoblastomycosis that mimicked a uveal melanoma with scleral invasion. Report of a Case. A 75-year-old white woman was referred for evaluation of a pigmented lesion of her right na- ARCH OPHTHALMOL / VOL 130 (NO. 12), DEC 2012 1615 WWW.ARCHOPHTHALMOL.COM ©2012 American Medical Association. All rights reserved. Downloaded From: https://jamanetwork.com/pdfaccess.ashx?url=/data/journals/ophth/926063/ on 05/09/2017 Figure 1. An elevated pigmented mass is situated about 2.5 mm from the limbus. The leash of conjunctival vessels that surround the mass is not typical of deeper episcleral vessels (sentinel vessels) associated with a ciliary body melanoma. Inset, Irregular black surface of the mass through the epithelium, which retains some fluorescein. Figure 2. The pigmented mass, which is separated from the epithelium, consists of a tangle of septate fungal hyphae and spherical structures (periodic acid–Schiff; bar indicates 15 m). Inset, Spherical (or sclerotic) bodies, many of which are collapsed or weakly staining (Gomori methenamine silver; bar indicates 10 m). sal conjunctiva. The lesion had been present for 16 years, following a traumatic injury with a tree branch. The initial injury was minor and required no professional medical care. A pigmented lesion, however, developed at the site of injury and enlarged slowly over years. During the last several months, it began causing irritation and redness. When examined, best-corrected visual acuity in the affected eye was 20/25. The lesion was 2.5 mm from the limbus, just thicker than 1 mm, and 3.7 mm in its greatest diameter. Under slitlamp magnification, the surface resembled black cauliflower (Figure 1). The overlying epithelium was shaggy, and it pooled and retained fluorescein (Figure 1, inset). The remainder of findings from the eye examination, including dilated ophthalmoscopy, were unremarkable. Ultrasound biomicroscopy revealed no mass beneath the lesion. Although the history of trauma was reliable, the concern over an invasive melanoma persisted, so a biopsy was recommended with that prevailing clinical diagnosis. Metastatic cutaneous melanoma was possible, although there was no history of skin melanoma. Pigmented squamous cell carcinoma and pri- mary conjunctiva melanoma were less likely because of the location of the mass beneath the epithelium and, in the case of squamous cell carcinoma, the patient’s fair complexion. A shave biopsy was performed in the operating room. Microscopic examination showed mild epithelial hyperplasia with focal keratinization and nongranulomatous chronic inflammation of the substantia propria. The pigmented tissue consisted of tangled fungal hyphae admixed with spherical structures (Medlar bodies), measuring between 4 and 15 m in diameter (Figure 2). The mass of fungal elements was devoid of inflammation, and hyphae showed cross septa. The Medlar bodies stained with periodic acid–Schiff reaction and Gomori methenamine silver (Figure 2, inset). No budding yeasts were seen. Cultures from the conjunctiva were unsuccessful before the patient started treatment with topical natamycin, 5%, suspension. The patient was intolerant to topical antifungal medications and was treated with oral ketoconazole, 200 mg once daily. Comment. The dematiaceous fungi that cause chromoblastomycosis are found worldwide, but most human infections occur in the tropics or subtropics. Organisms usually incite epithelial hyperplasia and chronic granulomatous inflammation. The chestnut-colored spherical structure known as a Medlar body (or sclerotic body) is not to be confused with conidia, or the asexual reproductive spores used to classify species under standardized growth conditions in the laboratory. Medlar bodies are poorly understood structures but are characteristic of the tissue phase of chromoblastomycosis.1-4 They likely represent an adaptive form of dematiaceous fungus capable of surviving prolonged periods in an inhospitable environment.2,4 Although the particular fungus in this case could not be identified through microscopic examination of reproductive spores in culture, chronic mycosis of the conjunctiva of any type is exceptionally rare.5 Treatment is based on experience with cutaneous infection and consists of surgical excision and chemotherapy with a synthetic imidazole.6 Reports of late relapse with skin infection, however, are common. In the semitransparent conjunctiva, chronic infection from a dematiaceous fungus can resemble a melanocytic neoplasm and should be added to the list of pseudomelanomas of the ocular adnexa. Anh Q. Bui, MD Edgar M. Espana, MD Curtis E. Margo, MD, MPH Author Affiliations: Departments of Ophthalmology (Drs Bui, Espana, and Margo) and Pathology and Cell Biology (Drs Espana and Margo), Morsani College of Medicine, University of South Florida, Tampa. Correspondence: Dr Margo, Department of Ophthalmology, Morsani College of Medicine, University of South Florida, 12901 Bruce B. Downs Blvd, MCD Box 21, Tampa, FL 33612 ([email protected]). Conflict of Interest Disclosures: None reported. ARCH OPHTHALMOL / VOL 130 (NO. 12), DEC 2012 1616 WWW.ARCHOPHTHALMOL.COM ©2012 American Medical Association. All rights reserved. Downloaded From: https://jamanetwork.com/pdfaccess.ashx?url=/data/journals/ophth/926063/ on 05/09/2017 1. McGinnis MR. Chromoblastomycosis and phaeohyphomycosis: new concepts, diagnosis, and mycology. J Am Acad Dermatol. 1983;8(1):1-16. 2. Fader RC, McGinnis MR. Infections caused by dematiaceous fungi: chromoblastomycosis and phaeohyphomycosis. Infect Dis Clin North Am. 1988;2 (4):925-938. 3. Rosen T, Overholt M. Persistent viability of the Medlar body. Int J Dermatol. 1996;35(2):96-98. 4. da Silva JP, Alviano DS, Alviano CS, et al. Comparison of Fonsecaea pedrosoi sclerotic cells obtained in vivo and in vitro: ultrastructure and antigenicity. FEMS Immunol Med Microbiol. 2002;33(1):63-69. 5. Galor A, Karp CL, Forster RK, Dubovy SR, Gaunt ML, Miller D. Subconjunctival mycetoma after sub-Tenon’s corticosteroid injection. Cornea. 2009;28 (8):933-935. 6. Brandt ME, Warnock DW. Epidemiology, clinical manifestations, and therapy of infections caused by dematiaceous fungi. J Chemother. 2003;15(suppl 2): 36-47. 70 Ciprofloxacin 60 Levofloxacin Resistant Isolates, % Moxifloxacin 50 Gatifloxacin 40 30 20 10 0 1990-1994 (n = 29) 1995-1999 (n = 23) 2000-2004 (n = 26) 2005-2011 (n = 89) Evolving Fluoroquinolone Resistance Among Coagulase-Negative Staphylococcus Isolates Causing Endophthalmitis Figure. Percentage of fluoroquinolone-resistant coagulase-negative Staphylococcus isolates causing endophthalmitis at the Bascom Palmer Eye Institute during the past 21.5 years. Data are divided by each fluoroquinolone antibiotic. E lococcus, the frequency of resistance to these organisms is increasing. Recent evidence shows that repeated exposure of ocular and nasopharyngeal flora to ophthalmic antibiotics, including fluoroquinolones, creates resistant strains.1,2 It has further been shown that resistant strains of coagulase-negative Staphylococcus may be associated with greater ocular inflammation, greater virulence, and increased ocular infection rates compared with susceptible strains.3,4 Fourth-generation fluoroquinolones are significantly more expensive than generic traditional antibiotic eyedrops such as gentamicin sulfate and polymyxin B sulfate/trimethoprim, which have been shown to cover endophthalmitis isolates at least as well.5 Additional recent reports demonstrate that the fourth-generation fluoroquinolones achieve subtherapeutic levels in the aqueous humor and vitreous against the most frequently identified staphylococcal endophthalmitis isolates.6 Given the frequent and increasing resistance, subtherapeutic penetration, and higher cost compared with other antibiotic eyedrops, the widespread perioperative and periprocedural use of fourth-generation fluoroquinolone antibiotic eyedrops should be reevaluated. ndophthalmitis is a serious, sight-threatening condition resulting in substantial morbidity. With the widespread use of fluoroquinolone antibiotic eyedrops as a prophylactic agent, there is concern regarding increased frequency of fluoroquinolone resistance. We report the evolution of fluoroquinolone resistance among coagulase-negative Staphylococcus endophthalmitis isolates at the Bascom Palmer Eye Institute. Methods. The study was approved by the Institutional Review Board of the University of Miami School of Medicine Medical Sciences Subcommittee for the Protection of Human Subjects. This was a retrospective, noncomparative, consecutive case series. We reviewed the microbiological and medical records of all patients with culture-proven endophthalmitis (positive cultures from the vitreous cavity) caused by coagulase-negative Staphylococcus at the Bascom Palmer Eye Institute between January 1, 1990, and July 1, 2011. Susceptibility testing of the intraocular isolates was performed using an automated system—the VITEK automatic microbial system (Biomérieux, Inc) or the E test (AB Biodisk NA, Inc and Remel Products). Frozen isolates were reconstituted as needed to evaluate sensitivities of earlier cases to newer-generation fluoroquinolones. Results. During the 21.5 years of the current study, 168 patients were identified as having culture-proven endophthalmitis caused by coagulase-negative Staphylococcus. The increasing resistance rates are shown in the Figure for 1990 to 1994 (n = 29), 1995 to 1999 (n = 23), 2000 to 2004 (n=26), and 2005 to 2011 (n=89). The respective resistances (in percentages) of the first 3 periods are the following: ciprofloxacin resistance, 10.3%, 17.4%, and 38.4%; levofloxacin resistance, 0%, 17.0%, and 38.4%; moxifloxacin resistance, 0%, 21.8%, and 26.9%; and gatifloxacin resistance, 0%, 21.8%, and 30.7%. The mean resistance rates for January 1, 2005, through July 1, 2011 (n=89), were 60.5% for ciprofloxacin, 58.6% for levofloxacin, 57.8% for moxifloxacin, and 60.5% for gatifloxacin (Figure). Comment. Despite the dual mechanisms of fluoroquinolones to avoid resistance to coagulase-negative Staphy- Andrew M. Schimel, MD Darlene Miller, DHSc Harry W. Flynn Jr, MD Author Affiliations: Department of Ophthalmology, Bascom Palmer Eye Institute, University of Miami Miller School of Medicine, Miami, Florida. Dr Schimel is now also with the Center for Excellence in Eye Care, Miami. Correspondence: Dr Flynn, Department of Ophthalmology, Bascom Palmer Eye Institute, University of Miami Miller School of Medicine, 900 NW 17th St, Miami, FL 33136 ([email protected]). Conflict of Interest Disclosures: None reported. 1. Kim SJ, Toma HS. Ophthalmic antibiotics and antimicrobial resistance: a randomized, controlled study of patients undergoing intravitreal injections. Ophthalmology. 2011;118(7):1358-1363. 2. Kim SJ, Toma HS, Midha NK, Cherney EF, Recchia FM, Doherty TJ. Antibiotic resistance of conjunctiva and nasopharynx evaluation study: a prospective study of patients undergoing intravitreal injections. Ophthalmology. 2010; 117(12):2372-2378. ARCH OPHTHALMOL / VOL 130 (NO. 12), DEC 2012 1617 WWW.ARCHOPHTHALMOL.COM ©2012 American Medical Association. All rights reserved. Downloaded From: https://jamanetwork.com/pdfaccess.ashx?url=/data/journals/ophth/926063/ on 05/09/2017