Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Quantium Medical Cardiac Output wikipedia , lookup
Pericardial heart valves wikipedia , lookup
Marfan syndrome wikipedia , lookup
Turner syndrome wikipedia , lookup
Artificial heart valve wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Aortic stenosis wikipedia , lookup
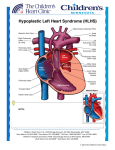
Case Presentation : Hypoplastic Left Heart Syndrome (HLHS) Dr.Ranjitha.G, Specialist Radiologist, NMC SH Al Ain, UAE Incidence: HLHS occurs in approximately 1 in 10000 live births. Definition: HLHS includes a spectrum of heterogeneous conditions characterized by severe hypoplasia of the left ventricle and left ventricular outflow tract. Anatomy: There are two forms of HLHS: first one is characterized by mitral and aortic atresia, the second by aortic atresia and a hypoplastic but patent mitral valve . The other cardiac anomalies, characterized by severe hypoplasia of left cardiac sections, that are unable to support systemic circulation , are also included under the term HLHS; and are represented by some forms of critical aortic stenosis, by the Shone complex (which is characterized by anomalies of mitral valve, coarctation of aorta and sub aortic stenosis) and by unbalanced ASD with right ventricular dominance. Aortic coarctation is associated with 70% of cases of HLHS. Ultrasound diagnosis: On the 4-chamber view, either a small globular left ventricle with endocardial fibroelastosis or a slit-like left ventricle (mitral and aortic atresia) are detected. The hypoplastic left ventricle never reaches the apex of the heart. The mitral valve is atretic or with a hypoplastic annulus. On the long axis view of the left ventricle it is possible to observe with difficulty a threadlike ascending aorta and extremely hypoplastic annulus of the aortic valve. Color doppler confirms the absence of filling of left ventricle and demonstrates reverse flow (left to right) flow across the foramen ovale and mitral regurgitation, in those characterized by patent and dysplastic mitral valve . On the 3 vessel view, color doppler demonstrates the retrograde flow in the hypoplastic aortic arch. Case discussion: A pregnant women ( G2P1L1A0) who conceived after 8 years of secondary infertility came for a routine antenatal screening at 24 weeks of gestation. The cardiac abnormalities were in favor of HLHS. The primary findings were hypoplastic left ventricle, aortic atresia and a hypoplastic but patent mitral valve. There were no other structural anomalies detected in the rest of the fetus. She was referred to a tertiary care center where the diagnosis was confirmed. The parents were councelled and are expected to deliver in a tertiary set up in their native country. The couple had refused chromosomal analysis. Figure A Figure B Figure C Figure A: Abnormal 4-chamber view with a small, non apex–forming left ventricle. Figure B: Long axis view of left ventricle showing thin threadlike ascending aorta. Figure C: 3 vessel view showing large ductus arteriosus. Figure D Figure E Figure F Figure D: Color doppler flow in 4-chamber view depicts patent mitral valve. The turbulence across the mitral valve suggest mitral regurgitation. Figure E: Color doppler flow shows retrograde flow in the hypoplastic aortic arch. . Risk of chromosomal anomalies in HLHS: High (up to 15%) in the fetus; 3-4% in post natal life Risk of non-chromosomal syndromes in HLHS : Low Outcome in HLHS : Poor, with high postnatal mortality and morbidity.