Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
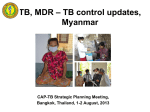
V-QUIN MDR Trial Overview RESIST TB Webinar | 3 November 2016 Q UIN V MDR-TB prevention study SYDNEY MEDICAL SCHOOL Greg Fox, PI VQUIN MDR Trial University of Sydney Trial Registration: ACTRN12616000215426 (Australian and New Zealand Trials Registry) Background VQUIN MDR-TB prevention study Background: the global burden of MDR-TB › MDR-TB affects 480,000 (360,000-600,000) people each year1 and is responsible for 13% of all TB deaths2 › Second-line treatments are prolonged, complex, toxic and costly compared to first-line therapies › MDR-TB consumes 20% of TB control budgets in resourcelimited settings2 › New strategies are urgently needed to prevent MDR-TB 1WHO Global TB Report 2015 2WHO Global TB Report 2014 3 Infection with M. tuberculosis › Latent tuberculosis infection TST/IGRA 4 Background: MDR-TB in contacts › Contacts of patients with MDR-TB have a high risk of LTBI and TB - Our study in Ho Chi Minh City, Vietnam, found 40.8% of 151 contacts of RR-TB had TST ≥ 10mm or above (OR 2.0, 95% CI 1.3-3.2 compared to new TB)3 - 5% of contacts of MDR-TB patients in Peru developed TB within 3 years4 › Not all TB in MDR-TB contacts is MDR-TB - 72% (36/50) of MDR-TB contacts in Peru developed MDR-TB4 - In our study 3/7 contacts with incident or prevalent MDR-TB had MDR-TB (however 2/2 incident cases had MDR-TB.)3 1Marks et al, AJRCCM 2000 et al, Chest 2016 3Fox et al, IJTLD 2016 (accepted for publication) 4Grandjean et al, 2011 2Trauer 5 Approach to preventive therapy for MDR-TB contacts › Preventive therapy aims to: - Reduce the risk of progression from LTBI disease - Reduce transmission › In treating LTBI due to MDR-TB or XDR-TB, antibiotic selection is based upon the confirmed or suspected drug resistance pattern of the presumptive source case › Decision to use preventive therapy must weigh the likely benefits and risks of therapy 6 Preventive therapy for MDR-TB › Randomized studies of 6-12 months of isoniazid preventive therapy (IPT) for contacts of drug susceptible TB have been shown to reduce the incident of TB by 40-90%1 › Fluoroquinolones are well tolerated and appear effective against M. tuberculosis in vivo2 › Small observational studies have been promising: - 110 MDR-TB contacts in Micronesia received 12 months (including FQ) – no incident cases3 - 184 children received 6 months of therapy including FQ – well tolerated4 › No randomized trials of preventive therapy for MDR-TB contacts have been conducted. 1Lobue et al, Respirology 2010 2Gillespie et al, REMOX trial 2014 3Bamrah et al, 2010 4Seddon et al, 2013 7 Levofloxacin for treating TB Levofloxacin for treating MDR-TB › Levofloxacin (LFX) is a 3rd generation FQ - FQNs inhibits DNA gyrase and are highly active against M. tuberculosis - Batericidal and sterilising actions (murine models) › LFX is commonly used in backbone of MDR-TB treatment regimen › Levofloxacin has a long history of use and is generally well-tolerated 9 Fluoroquinolone and MDR-TB 10 “Moxifloxacin, gatifloxacin and high-dose levofloxacin have excellent EBA, only slightly less than INH, and greater EBA” (5 days) Gatifloxacin 400mg / Moxifloxacin 400mg / levofloxacin 1000mg (5 days) Gatifloxacin 400mg / Moxifloxacin 400mg / levofloxacin 1000mg (5 days) 14 Fluoroquinolones in treating LTBI Prospective cohort study in the Federated States of Micronesia Setting: › FSM is a Western Pacific nation affiliated with the USA › TB incidence 127 / 100,000 in 2007 › Outbreaks of MDR-TB between 2007-2009 › 232 contacts identified 119 contacts with LTBI (5mm cut-off) offered preventive therapy by DOT; regimens included: - Monthly compensation ($5) provided to contacts completing 90% of doses Source M.tb resistance Age (y) MDR LTBI regimen INH, RIF, ETH >12 MFX 400mg + EMB 15mg/kg daily for 12 mo. ≤12 LFX 20mg/kg + EMB 15/mg/kg for 12 mo. >12 MFX 400mg daily for 12 mo. ≤12 LFX 20mg/kg daily for 12 mo. Bamrah et al, IJTLD 2014 INH, RIF, EMB, PZA, SM 16 Prospective cohort study in the Federated States of Micronesia Results - 119 TST positive individuals offered treatment - Contacts followed to February 2012 - Findings during follow-up (a) 104 accepted treatment 93 completed treatment (89%), 0 MDR-TB cases (b) 15 refused MDR-TB treatment 3 developed MDR-TB - Contacts who took treatment had a median age of 24, those who did not had a median age of 32 - 56 (54%) of treated contacts reported at least one adverse effects, with 16 (15%) reporting adverse effects 3 times or more. - No individuals tested positive for HIV Bamrah et al, IJTLD 2014 17 Tolerability of regimens in FSM 18 Prospective cohort study: child contacts in South Africa › Small observational studies have been promising: - 186 children (<5 or HIV+ <15 years), regardless of TST status - Treated with OFX, EMB and high dosed INH for 6 months - Treatment was were well tolerated1 - Adherence 141 / 186 (75.8%) - 7 (3.7%) developed Grade 3 or Grade 4 - 1 death (0.5%), 6 (3.2%) cases of incident TB during 219 years follow-up 1Seddon … Schaaf, 2013 19 Levofloxacin for LTBI › Optimal duration of therapy? › Optimal dose in LTBI? 20 Current guidelines for preventive therapy in MDR-TB Institution (Year) Recommended treatment for LTBI that is presumed multidrug resistant WHO (2014) Strict clinical observation for 2 years is preferred over provision of preventative therapy. Benefits of preventive therapy may outweigh harm for children <5 years. If preventive therapy is given, monitor for acquired drug resistance. US CDC (2000) Not stated UK NICE Guidelines (2016) Not stated European Union Standards for TB care (2012) Clinical monitoring and no preventive therapy. Canadian TB Standards (2013) MDR-TB: 9LFX or 9MOX with close monitoring. Harvard – UAE (2015) At least 6 months LFX or MOX, following all exposed individuals at least 18 months 21 Adverse events and levofloxacin Common side effects A decision about using prolonged antibiotics to treat LTBI requires an evaluation of the likely risks vs benefits Common side effects of levofloxacin include: › nausea, diarrhea, headache, dizziness, lightheadedness, or trouble sleeping. US FDA July 2016 23 FDA Drug Safety Communication: FDA updates warnings for oral and injectable fluoroquinolone antibiotics due to disabling side effects Safety Announcement [07-26-2016] The U.S. Food and Drug Administration (FDA) approved changes to the labels of fluoroquinolone antibacterial drugs for systemic use (i.e., taken by mouth or by injection). These medicines are associated with disabling and potentially permanent side effects of the tendons, muscles, joints, nerves, and central nervous system that can occur together in the same patient. As a result, we revised the Boxed Warning, FDA’s strongest warning, to address these serious safety issues. We also added a new warning and updated other parts of the drug label, including the patient Medication Guide. We have determined that fluoroquinolones should be reserved for use in patients who have no other treatment options for acute bacterial sinusitis (ABS), acute bacterial exacerbation of chronic bronchitis (ABECB), and uncomplicated urinary tract infections (UTI) because the risk of these serious side effects generally outweighs the benefits in these patients. For some serious bacterial infections the benefits of fluoroquinolones outweigh the risks, and it is appropriate for them to remain available as a therapeutic option. Patients must contact your health care professional immediately if you experience any serious side effects while taking your fluoroquinolone medicine. Some signs and symptoms of serious side effects include unusual joint or tendon pain, muscle weakness, a “pins and needles” tingling or pricking sensation, numbness in the arms or legs, confusion, and hallucinations. Talk with your health care professional if you have any questions or concerns (see List of Serious Side Effects from Fluoroquinolones). 1997-2015: 178 cases of disabling potentially irreversible Health care professionals should not and prescribe systemic fluoroquinolones to patients who have other treatment options for acute bacterial sinusitis (ABS), acute bacterial exacerbation of adverse reaction chronic bronchitis (ABECB), and uncomplicated urinary tract infections (UTI) because the risks outweighpatients the benefits in these patients. fluoroquinolone immediately if a patient In 2014, 22 million in the USStopreceived a treatment prescription for reports serious side effects, and switch to a non-fluoroquinolone antibacterial drug to complete the patient’s treatment course (see List of Currently Available FDA-approved FQN (cipro, moxi, ofloxacin, gemifloxacin) Fluoroquinolones for Systemic Use). US FDA July 2016 Update to boxed warning on the labels24 Fluoroquinolones are antibiotic medicines that work by killing or stopping the growth of bacteria 25 Study setting MDR-TB in Vietnam VQUIN MDR-TB prevention study › Vietnam has approximately 5,000 cases of MDR-TB / year - Notifications were approx. 1,500 (2013), 2,000 (2014), 2200 (2015) - Global Fund has set target of 3,000 new patients treated by 2017. - 16.7% of MDR-TB is FQ resistant (ofloxacin)1 › Treatment for MDR-TB is through District TB Units - Diagnosis and initial treatment in inpatient facilities (e.g. Pham Ngoc Thach Hospital in Ho Chi Minh City, or Hanoi Lung Hospital) - Provided free of charge (PMDT program) 14th National DR Survey, Nguyen VN et al 2015 27 VQUIN study objectives VQUIN MDR-TB prevention study › Principal research question: What is the effectiveness of levofloxacin given for 6 months, compared to placebo, in the prevention of active TB among household contacts of patients with MDR-TB who have latent tuberculosis infection?” › Secondary objectives (1): - Evaluate the tolerability, adherence, severe adverse events (Grade 3, 4 and 5) and cost-effectiveness of 6 months of levofloxacin therapy, compared to placebo, in contacts of patients with MDR-TB - Determine the rate of acquired fluoroquinolone resistance among contacts taking six months of levofloxacin compared to placebo who develop incident tuberculosis 28 VQUIN study objectives VQUIN MDR-TB prevention study › Secondary objectives (continued): - Determine the difference in specific biomarkers: (a) between infected contacts from therapy initiation to six months later among compliant contacts allocated to levofloxacin, compared to placebo, (b) between tuberculosis infection and disease. - Compare the effectiveness of levofloxacin compared to placebo among contacts of patients with MDR-TB bacilli that are susceptible to fluoroquinolones - Evaluate the cost-effectiveness of 6 months of levofloxacin therapy, compared to placebo, in contacts of patients with MDR-TB 29 Study design › Double blind placebo controlled RCT - Randomize 2,006 contacts over 30 month period - Children <15 years screened for active TB, and LTBI, but not treated (due to ethics committee concerns) – will aim to expand later 30 VQUIN V-QUIN Trial design 6LEV Active arm Control arm Placebo Screening Phase Treatment Phase Months 0 1 Days 0 0 Visit MDR-TB prevention study 1 2 12 18 24 30 30 60 90 120 150 180 365 540 720 900 1 7 8 9 10 2 3 Follow-up Phase 3 4 5 4 5 6 6 6LEV = six months of daily oral levofloxacin Q UIN V Sample size: 2,006 contacts randomized MDR-TB prevention study TB incidence in 2 years (in group taking placebo) Total infected household contacts to be randomized Estimated total household contacts to recruit in 3 years if 60% infected Estimated MDRTB patients to recruit within 3 years 2.5% 2414 4,023 1,915 3.0% 2,006 3,344 1,592 3.5% 1,711 2,852 1,358 32 Source: http://wikipedia.org China Hà Nội Capital V V-QUIN MDR QUIN Trial candidate recruitment sites Vietnam 2015 - 2020 MDR-TB prevention study Nam Định Province Laos National Tuberculosis Program Vietnam Thanh Hóa Province Đà Nẵng City Quảng Nam Province Cambodia An Giang Province Cần Thơ City Khánh Hòa Province Hồ Chí Minh City Tiền Giang Province Eligibility: index patients VQUIN MDR-TB prevention study › Index patients with microbiologically confirmed MDR-TB, and enrolled on treatment through the NTP, are eligible to enrol Inclusion criteria for index patients Exclusion criteria for index patients Any age A diagnosis of bacteriologically proven pulmonary MDR-TB * Commenced on treatment for MDR-TB Unwilling or unable to provide informed consent Usual residence is outside of the Provinces participating in the study by the Vietnam National TB Program within the past 90 days Have at least one household contact that is likely to be eligible for the study *Definition of bacteriologically proven MDR-TB: • Acid fast bacilli (AFB) smear positive, M. tuberculosis (MTB) culture positive, OR MTB positive based on the PCR-based sputum test Xpert MTB/RIF; AND • Rifampicin (RIF) resistant on Xpert, OR has phenotypic resistance to rifampicin and isoniazid on DST, OR has rifampicin and isoniazid resistance on other approved molecular assays. Eligibility: household contacts Inclusion criteria Exclusion criteria Any age Living in the same household** as the index patient within the previous 3 months VQUIN MDR-TB prevention study Unwilling or unable to provide informed consent Suffering from a condition likely to lead to uncooperative behaviour (e.g. severe psychiatric illness or alcoholism). 35 Criteria for randomization of household contacts Eligibility criteria for randomization Age ≥15 years [to be reviewed in 2017, to extend to children] Tuberculin skin test positive (a size of 10mm or greater at first reading); OR Any TST size if known to be HIV positive or severely malnourished; OR New TST conversion on the second reading, defined as: If the first test was <5mm o a size of 10mm or greater at second reading; OR If the first test was 5-9mm: o an increase of 6mm or greater at the second reading 36 Criteria for randomization of household contacts • Exclusion criteria (1) • Diagnosis of current active TB disease made during initial assessment¶ • Known to be pregnant* • Unable to take oral medication • Body weight < 3kg • Unwilling or unable to participate in follow-up for 30 months • Currently breast feeding** • Known allergy to fluoroquinolone antibiotics, or history of severe tendinopathy related to fluoroquinolones • Currently taking another medication reported to increase the cardiac QTc interval (e.g. amiodarone, sotalol, disopyramide, quinidine, procainamide, terfenadine) • Documented previous treatment for MDR-TB • Documented treatment with antibiotics that are active against MDR-TB in the previous month (including fluoroquinolones). • Prior severe blistering reaction to tuberculin • End stage liver failure (class Child-Pugh C). • Dialysis-dependent chronic kidney disease 37 Criteria for randomization of household contacts • Exclusion criteria (2) • For adults aged 15 and above only: • A baseline liver function test (AST, ALT or ALP) more than 3 times the upper limit of normal • Baseline ECG shows the QT segment (corrected for the R-R interval) is >450ms • Kidney tests show end stage kidney disease (defined as an EGFR < 20mL/min) • The platelet count is < 50x109 cells/L 38 Initial assessment of contacts › Symptom screen (cough, sputum, haemoptysis, weight loss etc) › Chest Xray › Tuberculin skin test (RT23) › Sputum Xpert (if can produce sputum) Tuberculin skin test: All contacts will have a Mantoux tuberculin skin test (2 tuberculin units of RT23) placed subcutaneously, with reading after 48-72 hours to establish LTBI status. 39 Levofloxacin dosing and duration Levofloxacin / Levofloxacin / Levofloxacin / Weight placebo placebo placebo Daily dose (mg) 250 mg tablets 500mg tablets 750mg tablets 12.0– 24.99 kg 1 tablet -- -- 250mg 25.0 – 49.99kg -- 1 tablet -- 500mg 1 tablet 750mg 50kg & above • 180 doses of levofloxacin will be given (and treatment extended if patients do not adhere to therapy). • If the estimated creatinine clearance is <20mL/min then the subject will not be eligible for therapy. If the creatinine clearance is <50mL/min then the dose will be adjusted to half that of the normal adult dose (US FDA Levofloxacin Product information). If the subject’s creatinine clearance is ≥ 50mL/min then the usual dose will be given. 40 Investigation of suspected TB In contacts aged ≥ 5 years In child contacts aged < 5 years Symptoms are defined as one or more Symptoms are defined as one or more of: of: Cough a for 2 weeks or more • Coughb Sputum production for 2 weeks or • Fever more • Night sweats Night sweats • Lethargy Haemoptysis • Failure to thrive Documented weight loss • Documented weight loss • Moderate or severe malnutrition 41 Investigation of TB suspects › The appropriate tests for suspected pulmonary TB in contacts aged 5 and above will include: - 2 sputum samples, both tested for sputum smear and culture and (if applicable) DST - 1 sputum sample, tested for Xpert (or equivalent PCR based diagnostic test) › Sputum will be collected from suspects using sputum induction, where this is available (not currently available). 42 Blinding › Participants and staff are blinded to treatment allocation › Unblinding can only occur on the basis of approval by the PI - Unblinding will be restricted to the clinician involved in the case 43 Outcome definitions Outcome definitions for subjects 15 years and over Primary outcome (1) › Bacteriologically-confirmed TB is defined as a positive identification of Mycobacterium tuberculosis by culture, Xpert or another PCR-based diagnostic test in a contact with clinical or radiological evidence of disease. › A result will be considered positive if: - (a) at least one sample of sputum, or other body fluid or tissue is positive by culture, Xpert or another PCR-based diagnostic test; or - (b) at least 2 samples of sputum or other body fluid or tissue are positive by smear) 45 Outcome definitions Primary outcome (2) › Extrapulmonary TB will be considered “bacteriologically confirmed” if based upon either: additional investigations seeking microbiological confirmation (e.g. lymph node aspirate, CSF) with either a positive culture, Xpert or another PCR-based diagnostic test; OR two or more samples that are AFB positive on smear. › Bacteriologically confirmed TB should be classified as pulmonary, extrapulmonary or both. › Microbiologically confirmed MTB should be classified as: - MDR-TB - Rifampicin Resistant TB - Not MDR-TB - Drug susceptibility unknown 46 Outcome definitions Probable Clinical TB › Definition: Known exposure to TB plus “Well-defined” clinical evidence AND supportive radiological or laboratory evidence of pulmonary or extrapulmonary disease in a contact that is not bacteriologically-confirmed. › The diagnosis of clinically probable TB is equivalent to the secondary outcome of “Clinical TB”. The End Point Review Panel will reach a conclusion about the diagnosis of clinically probable TB 47 Outcome definitions: others Possible clinical TB – Known exposure to TB plus clinical or radiological evidence/abnormality that is not consistent with above definitions AND a decision was made to treat for TB. Possible clinical TB should be classified as pulmonary, extra-pulmonary or both. 48 Death Death › The secondary mortality outcome will be death from any cause except for violent (e.g. homicide) or accidental (e.g. motor vehicle accident) causes. › A TB death is a death where TB is considered by the IDMC to be the most likely/major contributing cause of death. 49 Other outcomes Acquired drug resistance › Acquired antibiotic resistance will be deemed to have occurred when (a) molecular testing of paired isolates (index patient and contact with incident TB) demonstrates transmission has occurred (ie. the strain is the same) and, (b) the isolate of the Proportion of contacts successfully treated › Contacts will be classified as successfully treated if they either achieve outcomes of (a) treatment success, or (b) cure according to WHO treatment definitions 50 Adverse event classification Adverse events › Adverse events will be graded according to a scale derived from the: - American Thoracic Society Guidelines for hepatotoxicity, published criteria for joint, muscle and bone complications - National Cancer Institute Common Terminology Criteria for Adverse Events v4.0 › The Endpoint Review Panel will perform the grading of adverse events and establishment of their cause, blinded to the study drug. 52 Process for adverse event reporting Monitoring for AEs › Subjects will be assessed frequently during the study: - Once monthly on treatment - Then every six months › Routine blood tests: - LFTs and EUC at baseline, 1 month and 2 months › ECG - Performed at baseline, 1 month 53 Definitions of AEs and SAEs Definition of Severe Adverse Event › Any adverse event that: - results in death, - is life-threatening, - requires inpatient hospitalization or prolongation of existing hospitalization, - results in persistent or significant disability/incapacity, or - is a congenital anomaly/birth defect Definition of USAE (Unexpected Serious Adverse Event) › An event which is SERIOUS (SAE) AND UNEXPECTED. Definition of SUSAR (Serious Unexpected Suspected Drug Reaction) › An SAE for which there is some degree of probability that the event is an adverse reaction to the administered drug, and the adverse reaction is unexpected. 54 Interim analyses Interim safety analysis › The trial Independent Data Monitoring Committee (IDMC) will conduct an interim analysis after 1/3 of participants (600 contacts) have completed 6 months of therapy for grade 3 and 4 adverse events. Interim analysis for LFTs › After 600 contacts with LFTs at 1 and 2 months; IDMC will review need to continue for 1 and 2 month tests 55 Ethical issues › Ethical approval from: - the University of Sydney Human Research Ethics Committee and - the Institutional Review Board of the Vietnam Ministry of Health › Participants provide written informed consent › Oversight by an Independent Data Monitoring Committee 56 Study timeline › Recruitment at first site commenced 14/3/2016 › 8 Provinces currently recruiting, with 2 additional provinces to commence by 31/12/2016 › Completion of study expected in late 2020 57 VQUIN investigators NHMRC Project Grant #1081443 (2015-2019) › Dr Greg Fox (Principal Investigator), University of Sydney, Australia › Professor Guy Marks, University of New South Wales, Sydney, Australia › Professor Dick Menzies, McGill University, Montreal, Canada › A/Professor Nguyen Viet Nhung, National Lung Hospital, Hanoi, Vietnam › Professor Steve Graham, Melbourne University, Melbourne, Australia › A/Professor Ben Marais, Sydney University, Sydney, Australia › Professor Marcel Behr, McGill University, Montreal, Canada › A/Professor David Dowdy, Johns Hopkins University, BA, USA › A/Professor Andrea Benedetti, McGill University, Montreal, Canada 58 Trial Governance › Trial Steering Committee (Chair: Dr Greg Fox) › Scientific Advisory Committee (Chair: Prof Bill Burman) › Independent Data Monitoring Committee (Chair: Prof Andrew Nunn) › Expert Clinical Panel (Chair: Dr Hazel Goldberg) 59 Questions 60