Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
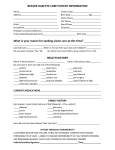
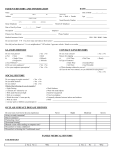
Patient Information Form Patient Name_________________________ Gender: ______ Date of Birth_______________ Mailing Address_______________________________________________________________ City__________________________ State_____________ Zip Code______________________ Home Phone___________________ Cell Phone________________ other_________________ Email________________________________________________________________________ Insurance Medical Insurance__________________________________________________ Vision Insurance____________________________________________________ Policy Holders Name________________________________________________ Policy Holders DOB_______________ Policy Holders Last 4 of SSN and work ID # if applicable____________________ Patient Visual Information Date of Last Eye Exam______________ Dr. Name and location__________________________ Do you wear contacts? ___________ Any interest in contacts today? ______________________ I am happy with comfort I am happy with the vision I am looking for multifocal contacts I am looking to have colored contacts I am looking to change current wear schedule of the contacts (daily, 2 week, monthly) Do you wear glasses? __________ What type of lenses? _____________________________ Please circle if you currently have or have experienced: Glaucoma Cataracts Iritis Uveitis Macular Degeneration Chronic Conjunctivitis Turned Eye(strabismus) Retinal Detachment Eye Patching Chronic Dry Eye Keratoconus Blepharitis LASIK Eye Injury(s) Please use this space and add additional comments concerns and surgical date that you have had: ________________________________________________________________________ ______________________________________________________________________________ ______________________________________________________________________________ ______________________________________________________________________________ ______________________________________________________________________________ Patient Medical Information Please circle any that you have had or are currently experiencing Cardiovascular Endocrine Gastrointestinal High Blood Pressure Stroke Heart Disease Vascular Disease Cholesterol Angina Congestive Heart Failure Crohn’s Diabetes Thyroid Dysfunction Gout Renal Disease Acid Reflux Ulcer Colitis Celiac Disease Hepatitis Diverticulosis OTHER _________________________________________________________________ Genitourinary Ear, Nose, Mouth, Throat Hematologic/ Lymphatic Kidney Disease Cancer Sexually transmitted Disease Herpes Chronic Cough Sinusitis Meniere Syndrome Dry Mouth Anemia Leukemia Hodgkin’s Disease Sickle Cell Disease OTHER______________________________________________________________________ Immunologic Integumentary Musculoskeletal Sjogren’s Syndrome Herpes Lyme Disease HIV AIDS Eczema Rosacea Psoriasis Lupus Osteoarthritis Fibromyalgia Muscular Dystrophy Arthritis Scoliosis OTHER________________________________________________________________________ Neurological Psychiatric Respiratory Bell’s Palsy Horner’s Syndrome Headaches Nystagmus Parkinson Multiple Sclerosis Vertigo Depression Anxiety Alzheimer’s Attention Disorder PTSD Autism Dementia Asperger’s Asthma COPD Bronchitis Emphysema Pneumonia Cystic Fibrosis Sarcoidosis Tuberculosis OTHER________________________________________________________________________ Woman only: Are you currently pregnant? __________________ Currently Breastfeeding: _______________ Anything that you feel should be known or any accommodations that would be helpful to make your eye exam more comfortable for you: ___________________________________________________________________________ ____________________________________________________________________________ Please list any and all medications, vitamins, and supplements you are currently taking ___________________________ _________________________ ___________________________ _________________________ ___________________________ _________________________ ___________________________ _________________________ ___________________________ __________________________ ___________________________ __________________________ Please indicate any immediate family members with any of the following disorders and their relation to you: Cataract: _________________ Glaucoma: _______________ Macular Degeneration: ______________ Other eye disorders: _______________ Diabetes: _______________ High Blood Pressure: _______________ High Cholesterol: _______________ Cancer: _______________ Thyroid Disorder: _______________ Other health issues: _______________