Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Quantium Medical Cardiac Output wikipedia , lookup
Aortic stenosis wikipedia , lookup
Heart failure wikipedia , lookup
Electrocardiography wikipedia , lookup
Coronary artery disease wikipedia , lookup
Myocardial infarction wikipedia , lookup
Cardiac surgery wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Atrial septal defect wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Truncal Inversion with Biventricular
Pulmonary Trunk and Aorta from Right
Ventricle (Variant of Taussig-Bing Complex)
By AARON B. SHAFFER, M.D., JosE' F. LOPEZ, M.D.,
AND
IRWIN K. KLINE, M.D.,
MAURICE LEV, M.D.
SUMMARY
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
A heart is described pathologically in which the aorta emerged from the right ventricle and was not related to the ventricular septal defect, while the pulmonary trunk
emerged from both ventricles, but mostly the right, and was related to the ventricular
septal defect. This Taussig-Bing arrangement of vessels was coupled with the presence
of the aortic orifice to the left and the pulmonic orifice to the right, which is an inverted
position. The anatomic concept of inversion is an abnormality in position from the
standpoint of laterality. A careful study of the conal regions of the left and right
ventricles showed that those regions were not inverted. Therefore, this represents
a case of Taussig-Bing complex with exclusively truncal inversion, which is unique. This
may be explained on the basis of opposite metameric contribution to the development
of the truncus.
Additional Indexing Words:
Transposition of the great vessels
Congenital heart disease
Double-outlet right ventricle
Truncus
tion. Thus, there was isolated inversion of the
aorta and pulmonary trunk, which is unique;
hence, the present report.
W E HAVE RECENTLY studied a heart
with biventricular origin of the pulmonary trunk, in which the aorta arose from the
left side of the right ventricle anterior to the
pulmonary trunk, which arose from the right
side of the right ventricle posteriorly. The
heart was in levocardia (normal position) with
all organs in situs solitus. The atria and inlets
of the ventricles and coni were in normal posi-
Clinical Review
The subject was a 3-month-old white female
infant, with the following diagnoses, based on
clinical, hemodynamic, and angiographic findings: nearly complete transposition of the great
vessels with ventricular septal defect, bi-directional but predominantly left-to-right shunt, pulmonary hypertension, "infantile" or "transitional"
coarctation of the aorta, and patent foramen
ovale. The aortic root was found to be anterior to
the root of the pulmonary trunk; however, the
usual laterality of the ascending aorta was not
noted during life. It could have been recognized
by an unusual course of the catheter in the ascending aorta in the frontal plane. An aortogram
in this projection was not obtained. In view of
the precarious condition of the patient, surgical
correction of the coarctation was recommended.
At surgery (November 1961), a large patent
ductus arteriosus was found to join the left pulmonary artery to the aorta distal to the coarctation. The coarctated segment of the aorta was re-
From the Congenital Heart Disease Research and
Training Center, Hektoen Institute for Medical Research; the Division of Cardiovascular Disease, Department of Medicine, and the Otto Saphir Pathology Institute, Michael Reese Hospital and Medical
Center; the Departments of Pathology of Northwestern University Medical School, University of Chicago
School of Medicine, and University of Illinois College
of Medicine, Chicago, Illinois.
This investigation was supported in full by Grant
5 PO HE-07605-05 from the National Institutes of
Health, National Heart Institute, Bethesda, Maryland.
Dr. Lev is Career Investigator and Educator of the
Chicago Heart Association.
Circulation, Volume XXXVI, November 1967
783
SHAFFER ET AL.
784
ectasis (bilateral). The viscera were all in normal position.
Heart
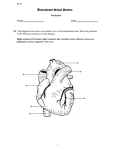
Figure 1
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
Diagramimatic sketch of the anterior viewl of the iniopened heart made fromti the opened heart. SVC supjerior venia ecav; P ==ptlmonary tr-uttk; and
A= aorta.
moved with an end-to-end anastomosis, and the
patent ductus arteriosus was also resected. The
patient did well initially, btut succumbed on the
second postoperative day.
Pathological Exainination
Aside from the findings in the heart, the pathological diagnosis was marked pulmonary atel-
Estimation of chamber size and muscle mass
of chambers was made by the method of Lev
and associates.' The heart was enlarged and
weighed 59 g (normal, about 28 g). The baseapex axis pointed toward the left and down.
The apex was formed by both ventricles. Txvo
arterial trunks emerged from the base: a
large ptulmonary trunk was situated posteriorly and to the right, and a smaller aorta anteriorly and to the left (fig. 1). The relationiships of the atria, inlets of the ventricles, and
coni were normal.
The right atrium was niormal in size and its
wall was of normal thickness. This chamber
received the superior and inferior venae cavae
and coronary sinus in a normal manner; the
eustachian and thebesian valves were normal.
The limbus was well formed, although small
in extent, and the foramen ovale was obliquely
patent, measuring 0.1 to 0.2 cm in greatest
dimension. The endocardium of this chamber
cu t enrAd
,)F P,
Figure 2
(Left) Right ventricular view showing emergence of pulmonary trunk. (Right) Diagrammatic
sketch of left panel. PT = pulmonary trunk; A
aorta; D - ventricular septal defect; TVtricuspid valve; P, first parietal band; and P, second parietal band. Arrowt voints to the
outflow tract into the aorta.
Circulazion, Volume XXXVI, November 1967
,-85
TRUNCAL INVERSION
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
Figure 3
(Left) Right veiitriciular view shiowing emergence of the aorta. (Righit) Diagratmmatic sketch
of left panel. A = aorta; S septal band group; an'd P, = first prarital band. Area enclosedc
in irregular black line is cutt end of first parietal hatnd.
dliffusely wvhitened. The tricuspid orifice
xvas enlarged; the tricuspid valve was normally
formed but presented increased hemodynamic
vas
change. 2
The right ventricle was enlarged and its wall
tlhickened. The inflow tract had the normal
architecture of the riglht ventricle. The outflow
tract howvever Wxas abnormal (figs. 2 and 3). A
septal band consisting of several components
proceeded from the left lateral wall to the base
of the aorta. Here it fornmed a wide muscular
parietal
structure. This structure gave off
band (first parietal band) xvhich extended
over the anterior wall of the right xventricle.
Part of the latter anchored on the septum again
in the lower part of the outflow tract. A second
parietal band extended fromr- the base of the
pulmonary trunk over the region adjacent to
the ainterior leaflet of the tricuspid valve. Thus
the outflow tract of the right veiltricle was
divided into tvo parts leading into the aorta
and pulmonary trunk xvith a more distinct
conus-like structure beneath the aorta. This
outflow tract, although abnormal, was clearly
was
a
Clt-cuZ{ation,! Voliiie XXXVI, Norlember 7967
that of a right venitricle. The endocardiumn of
the outflow tract xvas thickened. The aortic
orifice was somewhat larger than normal. The
aortic valve xvas normally formed, with mnarked
hemyiodynamic change and prominent hillock
formation at the commissures. Its annulus was
niot related to the tricuspid or mitral annulus.
The coronary ostia were situated in the posterior and right anterior sinuses of Valsalva. The
right coronary ostium gave rise to the anterior
descending coronary artery and to the right
circumflex. The latter gave off its usual
l)ranches to the right ventricle and terminated
in the posterior descending coronary artery.
The posterior coronary ostinin gave rise
to the left circumflex coronlary artery, wxhich
in tuirn gave off the ramus anterior ventriculi sinistri and the ramilus obtusus ventriculi sinistri. The coronary veins wvere not
dissected. The transverse aorta vas smaller
than- normal andI presented groups of sutures.
The pulmonary truniik emerged mostly from
the right ventricle but straddled the ventricular septum over a defect to be (lescribed later.
786j
SHAFFER ET AL.
Taussig-Bing lheart with truncal imxversion-i
1. Hypertrophy and enlargemenit of the
heart
a. Right xcentricular lhypertr-oplhv and
enlargement
I. Left atrial] hypertroplhy and enlargement
2.
3.
4.
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
Figure 4
Left ilcnticidar
liic.
)
= reentiicldai septatl dcfce.
The pulimonary
lvorifice wxas larger than
normiial,
its xalve was niorml-ally formned, and it presented imiarkedly incIreased lhemodynamiiic chanlge.
Its aInniulus wxxas in part related to the tricuspid valve. It xvas separated from the mlitral
annulus by
mnuscular ridge. The two pulmonoary arteries were given off normallv. The
aL
duictus arteriosus had been patent but
xvas
tied off at sutrgery.
The left atritm avas niarkedly enlarged and
its xvall xvas thickened. Its endocardium xvas
diffusely wlxitenied. The mitral orifice xwas enlarged, its valxe
xas
n-iormlnally formlUed,
and it
presented miarked hemiiodynainiic change.
The left ventricle (fig. 4) vas enlarged, but
its wall
normal iin thickness. The architecture of the inflow and outflow tracts reniormal left ventricle. Its
sembled that of
endocardium was diffusely whitenied. The ventricular septum at its base presented defect
imieasuring about 1 cm in greatest dim-ension.
This defect was situiated in the anterior part of
the ventricular septum and was confluent with
the left side of the mouth of the pulmonary
trunk. From this defect, a triangular muscle
l)and extended obliquely downward to the
base of the posterior papillary muscle and sent
a prong to the region of the anterior papillary
muscle.
The anatomic diaggnoses vere as follows:
xvas
a
a
5.
c. Left ventricular hypertrophy land enlargemenit
Veintricular septal defect
Fetal coarctation with an adult component with patenit ductus and surgical intervention (removal of adult coarctation ain-d closure of ductus)
Abnormal architecture of the xentrieular septumn
Patent foramyieni ovale.
DIiseussion
Hearts with l)iventricular orijin of the pulmonoary trunk wvith origin of the aorta fromii the
right ventricle, with or vithout pulmonaomry steniosis, have recently been studied by one of
us.4' A concept of xvhat we call the Taussigl3ing spectrum of hearts (or douille-outlet right
ventricle of the Taussig-Bing type) vas thereby developed. It xvas suggested that the Tanssig-Bing heart be considered anianatoml-ic entity, in which the aorta arises from the right
ventricle and is not related to the dlefect.
while the puliimonary trunk arises fromii the
right or 1)oth ventricles and is related to the
defect. In addition1, there is a distinct Imluscenlature of the conal region of the right ventricle, in which a septal band group proceeds
to the l)ase of the pulmonary trunk and connects to the first parietal band which separates
the aorta from the pulmonary trunk. A second
parietal l)and proceeds downward from the
aorta and is related to the anterolateral leaflet
of the tricuspid. Accordingly Taussig-Bing
lhearts xvere cl assified as (1) right ventricular
without overriding pulmonary trunk, (2) right
ventricular with overriding pulmonary trunk,
(3) intermnediate, and (4) left ventricular.
In our case the pulmonary trunk overrides
the defect but emerges mostly from the right
ventricle xvhile the aorta emerges exclusively
from the right ventricle away from the defect.
Circulaion, Volume XXXVI, November 1967
TRUNCAL INVERSION
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
The aorta and pulmonary trunk arise from
positions in the right ventricle opposite in
laterality to those in the usual Taussig-Bing
heart as described. This is accompanied by a
change in the conus of the right ventricle,
where the septal band is related to the aorta
and the second parietal band is related to the
pulmonary trunk. The first parietal band however continues to separate the aorta and pulmonary trunk.
Despite the alteration in muscular architecture of the conus of the right ventricle, we
consider this to be related to other hearts with
biventricular origin of the pulmonary trunk,
with the aorta emerging from the right ventricle. We consider the alteration in musculature as being related to the alteration in laterality of the aorta and the pulmonary trunk.
This alteration in laterality of the vessels, together with the anterior descending coronary
artery coming off the right aortic sinus of Valsalva, is the anatomic hallmark of inversion of
the truncal, trunco-conal or bulboventricular
regions.6-22
Inversion, anatomically, may be considered
to be a disturbance in laterality pursuant to a
certain axis. This axis is the longitudinal axis
of the body when the arterial trunks are considered, and the longitudinal axis of the heart
when the atria and ventricles are considered.
It is well known that the atria, ventricles,
or the trunco-conal areas may be selectively inverted. It is not known whether the coni or
arterial trunks may each be inverted alone,
separate from the other. In our case the atria
and sinuses of the ventricles were not inverted.
On the other hand, the bases of the two arterial trunks, derived from the truncus, were
clearly inverted. A problem arose in the interpretation of the conus. The normal conus has
a distinct right side with septal and parietal
bands, and an abbreviated left side fused with
the remainder of the left ventricle. Traditionally we consider a conus inverted when its
distinct portion with septal and parietal bands
lies in the left-sided chamber rather than in
the right. This was not true in our case, in
which the distinct portion, bearing facsimiles
of the septal and parietal bands, lay in the
Circulation, Volume XXXVI, November 1967
787
right-sided chamber. Therefore we judge the
conus not to be inverted.
A Taussig-Bing heart, as above defined, with
trunco-conal inversion should have the pulmonary trunk straddling the interventricular septum, while the aorta emerges completely from
the left-sided ventricle over a septal and parietal band; hence it would be similar to a corrected transposition. The aortic annulus, of
course, would be anterior and to the left of
the pulmonary annulus. This anatomic arrangement would not be physiologically the
same as Taussig-Bing heart without inversion,
or in our interpretation of the Taussig-Bing
heart with truncal inversion, in both of which
the aorta is in the line of systemic venous
blood.
This anatomic concept of inversion may be
expanded into a pathogenetic one, as Spitzer7
has done. We may be dealing with a reverse
contribution of metameres as may occur in any
one segment during the formation of the
original single heart tube from its two-sided
anlage.2 This inverse contribution of metameres in our case is assumed to occur only in
the aortic bulb (truncal) area. The sino-atrial
and ventriculobulbar contributions are presumed to be normal in this view, and the
bulboventricular loop is normally formed. In
this respect it may be recalled that the "aortic
bulb" (truncus) is a distinct structure separate
from the bulbus cordis.28 Together with the
reverse metameric formation of the truncus is
the unknown cause of transposition leading to
biventricular origin of the pulmonary trunk,
with the aorta emerging from the right ventricle.
Conclusion
A case is presented with biventricular origin
of the pulmonary trunk, and origin of the aorta from the right ventricle, with truncal inversion. The aorta emerged from the right
ventricle unrelated to a ventricular septal defect while the pulmonary trunk overrode the
septum over a defect, but emerged mostly
from the right ventricle. Altered septal and
parietal bands were found in the right-sided
ventricle. The aorta and pulmonary trunk
SHAFFER ET AL
788
were inverted, while the atria and the sinuses
of the ventricles were not inverted. Evidence
is presented toward the concept that the conus
was not inverted.
11.
References
1. LEV, M., ROWLATT, U.
2.
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
3.
4.
5.
6.
7.
8.
9.
10.
F., AND RIMOLDI, H. J.
A.: Pathologic methods for study of congenitally malformed heart: Methods for electrocardiographic and physiologic correlation. Arch
Path (Chicago) 72: 493, 1961.
LEV, M., AND ECKNER, F. A. O.: Embryologic,
pathogenetic and pathologic considerations. In
GASUL, B. M., ARCILLA, R. A., AND LEV, M.:
Heart Disease in Children: Diagnosis and
Treatment. Philadelphia, J. B. Lippincott Co.,
1966, p. 11.
LEV, M.: Some newer concepts of the pathology
of congenital heart disease. Med Clin N Amer
50: 3, 1966.
LEV, M., RIMOLDI, H. J. A., EcKNER, F. A. O.,
MELHUISH, B. P., MENG, C. C. L., AND PAUL,
M. H.: Taussig-Bing heart: Qualitative and
quantitative anatomy. Arch Path (Chicago)
81: 24, 1966.
NAVARRO LOPEZ, F., ET AL.: Taussig-Bing complex with pulmonary stenosis. Dis Chest 50:
1, 1966.
LEV, M., AND ROWLATT, U. F.: Pathologic anatomy of mixed levocardia: Review of thirteen
cases of atrial or ventricular inversion with or
without corrected transposition. Amer J Cardiol 8: 216, 1961.
LEY, M., AND VASS, A.: Spitzer's Architecture of
the Normal and Malformed Hearts. (Translation of Spitzer, A.: tber den Bauplan des
normalen und missbildeten Herzens: Versuch
einer phylogenetischen Theorie. Virchow Arch
Path Anat 243: 81, 1923.) Springfield, Illinois,
Charles C Thomas, Publisher, 1951.
CARDELL, B. S.: Corrected transposition of the
great vessels. Brit Heart J 18: 186, 1956.
ANDEHRSON, R. C., LILLEHEI, C. W., AND LESTER,
R. G.: Corrected transposition of the great vessels of the heart: Review of 17 cases. Pediatrics 20: 626, 1957.
DE LA CRUZ, M. V., ANSELMI, G., CISNEROs, F.,
R EINHOLD, M., PORTILLO, B., AND ESPINOVELA, J.: Embryologic explanation for the
corrected transposition of the great vessels:
Additional description of the main anatomic
12.
13.
14.
features of the malformation and its varieties.
Amer Heart J 57: 104, 1959.
SCHIEBLER, G. L., EDWARDS, J. E., BURCHELL,
H. B., DUSHANE, J. W., ONGLEY, P. A., AND
WOOD, E. H.: Congenital corrected transposition of the great vessels: Study of 33 cases.
Pediatrics 27: 851, 1961.
HONEY, M.: Anatomical and physiological features of corrected transposition of the great
vessels. Guy Hosp Rep 111: 250, 1962.
SHAHER, R. M.: Syndromes of corrected transposition of the great vessels. Brit Heart J 25:
431, 1963.
VAN MIEROP, L. H. S., AND WIGLESWORTH,
F. W.: Pathogenesis of transposition complexes: III. True transposition of the great vessels.
Amer J Cardiol 12: 233, 1963.
15. GRANT, R. P.: Morphogenesis of corrected transposition and other anomalies of cardiac polarity. Circulation 29: 71, 1964.
16. ROSENBAUM, H. D.: Simplified basic classification of spatial alignments of the heart, its
chambers, and the great vessels. Circulation
30: 194, 1964.
17. BERRY, W. B., ROBERTS, W. C., MoRmow, A. G.,
AND BRAUNWALD, E.: Corrected transposition
of the aorta and pulmonary trunk. Amer J Med
36: 35, 1964.
18. SHAHER, R. M.: Complete and inverted transposition of the great vessels. Brit Heart J 26:
51, 1964.
19. VAN PRAAGH, R., ONGLEY, P. A., AND SWAN,
H. J. C.: Anatomic types of single or common
ventricle in man: Morphologic and geometric
aspects of 60 necropsied cases. Amer J Cardiol
13: 367, 1964.
20. VAN PRAAGH, R., VAN PRAAGH, S., VLAD, P.,
AND KErrH, J. D.: Anatomic types of congenital dextrocardia: Diagnostic and embryologic
implications. Amer J Cardiol 13: 510, 1964.
21. VAN PRAAGH, R., AND VAN PRAAGH, S.: Isolated
ventricular inversion: Consideration of the morphogenesis, definition and diagnosis of nontransposed and transposed great arteries. Amer
J Cardiol 17: 395, 1966.
22. RAGHIB, G., ANDERSON, R. C., AND EDWARDS,
J. E.: Isolated bulbar inversion in corrected
transposition. Amer J Cardiol 17: 407, 1966.
23. DAVIS, C. L.: Development of the human heart
from its first appearance to the stage found in
embryos of twenty paired somites. Contrib
Embryol 19: 245, 1927.
Circulation, Volutme XXXVI, Novemnbet 1967
Truncal Inversion with Biventricular Pulmonary Trunk and Aorta from Right
Ventricle (Variant of Taussig-Bing Complex)
AARON B. SHAFFER, JOSÉ F. LOPEZ, IRWIN K. KLINE and MAURICE LEV
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
Circulation. 1967;36:783-788
doi: 10.1161/01.CIR.36.5.783
Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1967 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7322. Online ISSN: 1524-4539
The online version of this article, along with updated information and services, is
located on the World Wide Web at:
http://circ.ahajournals.org/content/36/5/783
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles
originally published in Circulation can be obtained via RightsLink, a service of the Copyright
Clearance Center, not the Editorial Office. Once the online version of the published article for
which permission is being requested is located, click Request Permissions in the middle column of
the Web page under Services. Further information about this process is available in the Permissions
and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation is online at:
http://circ.ahajournals.org//subscriptions/