Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Management of acute coronary syndrome wikipedia , lookup
Coronary artery disease wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Myocardial infarction wikipedia , lookup
Cardiac surgery wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Atrial septal defect wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
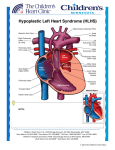
Pulmonary Flow Resistive Device Reported By: Taya Furmanski and Albert Attia Department of Biomedical Engineering Vanderbilt University April 22, 2003 Advisor: Dr. Thomas Doyle Associate Professor of Pediatrics and Director of Pediatric Catheterization Laboratory, Division of Pediatric Cardiology, Vanderbilt University Medical Center Instructor: Dr. Paul King Associate Professor of Biomedical and Mechanical Engineering, Vanderbilt University School of Engineering TABLE OF CONTENTS 1. ABSTRACT…………………………………………………………………………… 3 2. INTRODUCTION 2.1. HYPOPLASTIC LEFT HEART SYNDROME 2.1.1. DEFINITION……………………………………………………………... 4 2.1.2. ANATOMY AND PHYSIOLOGY……………………………………….4 2.1.3. CAUSE…………………………………………………………………… 6 2.1.4. CLINICAL EPIDEMIOLOGY……………………………………………6 2.2 CURRENT TREATMENTS 2.2.1. DRUG TREATMENTS………………………………………………….. 7 2.2.2. RECONSTRUCTIVE SURGERY……………………………………… 7 2.2.3. HEART TRANSPLANT………………………………………………… 8 2.3. DESIGN GOALS……………………………………………………………….. 8 3. METHODOLOGY 3.1. TIMELINE……………………………………………………………………….. 9 3.2. DESIGN AND PROTOTYPE 3.2.1. BACKGROUND…………………………………………………………. 10 3.3. TESTING 3.3.1. METHODS………………………………………………………………. 11 4. RESULTS 4.1. DESIGN 4.1.1. CONE DESIGN…………………………………………………………. 12 4.1.2. OTHER DESIGNS……………………………………………………… 14 4.2. SAFETY ANALYSIS…………………………………………………………… 15 4.3. EC0NOMIC ANALYSIS……………………………………………………….. 17 5. CONCLUSIONS……………………………………………………………………… 18 6. RECOMMENDATIONS……………………………………………………………… 19 7. REFERENCES……………………………………………………………………….. 21 APPENDIX A. SCHEMATIC OF HEART WITH AND WITHOUT DEVICE B. DESIGNSAFE REPORT C. INNOVATION WORKBENCH RESULTS 2 1. ABSTRACT Hypoplastic Left Heart Syndrome (HLHS) is a congenital disease that results in the underdevelopment of the left side of the heart. The embryologic cause of HLHS is not fully known; however it is thought to most likely result from either a reduction of left ventricular inflow or left ventricular outflow during development. Approximately 1440 babies are born each year in the United States with HLHS. Current treatments include reconstructive heart surgery and heart transplantation. The goal of our design is to eliminate the first two steps of reconstructive surgery while at the same time ensuring adequate systemic blood flow is achieved. Because the relative ratio of pulmonary to systemic blood flow depends on the balance between pulmonary and systemic vascular resistances, our device focuses on this relationship for treatment solutions. Thus, we have proposed a device that will increase the pulmonary resistance, thereby increasing the flow of blood through the ductus arteriosis and increasing oxygenated systemic blood flow. We began research and brainstorming HLHS in December of 2002. The completion date for this device is April 22, 2003. After exploring other options and presenting them to Dr. Doyle, we decided that the device should have a conical shape. Among the reasons for our conclusion were the effectiveness of the device in impeding flow, the ease at which it could be placed in the arteries, and the low health risks it provided for the patient. It was shown that the device decreased flow; however, the pressure drop across the device needed to be measured and this requires an in vivo model. In addition, animal testing needs to be conducted to test the effectiveness of the device. Afterward, human clinical trials would be required, with the approval of the FDA and the IRB. We believe these are the steps the next group should pursue. 3 2. INTRODUCTION 2.1 HYPOPLASTIC LEFT HEART SYNDROME 2.1.1 DEFINITION Hypoplastic Left Heart Syndrome (HLHS) is a congenital disease that results in the underdevelopment of the left side of the heart. With hypoplasia being defined as the underdevelopment of a tissue or organ, this disease extends to the cardiac structures of the left atrium and ventricle, the mitral valve, the aortic valve, and the aorta [4]. 2.1.2 ANATOMY AND PHYSIOLOGY A normal heart functions with both sides of the heart simultaneously pumping equal amounts of blood. The right ventricle is responsible for receiving oxygen-poor blood from the body and pumping it to the lungs, while the left ventricle is responsible for receiving the oxygenated blood from the lungs and pumping it through the aorta and to the body [7]. The right and left sides of the heart exist as two separate pumps and perform very important, individual tasks. However, in a hypoplastic heart, these functions cannot be completed normally because of the underdevelopment of the left side of the heart, which is the crucial mechanical component in delivering sufficient amounts of oxygenated blood to the organs of the body [1]. Figure 1: A comparison of the heart of an HLHS patient to a normal heart [2]. 4 HLHS is a collection of lesions and each case is unique in the extent to which the heart is malformed. Of all HLHS patients, 85% have some combination of atresia (congenital absence of normal opening or lumen) or stenosis (narrowing of any canal or orifice) of the aortic and mitral valves [9]. The remaining 15% have a common atrioventricular septal defect. On top of the malformations in valves of the heart, the left ventricle of the heart is grossly underdeveloped and in some cases is not present at all. These abnormalities result in inadequate heart function and thus reconstruction that is necessary to sustain normal metabolic function [1]. A hypoplastic heart has normal entry of the inferior vena cava and right superior vena cava into the right atrium; however, the right atrium is usually largely dilated. This enlargement, in addition to a larger tricuspid valve orifice, results in a hypertrophied (increased in bulk) right side of the heart (holding up to three times the normal blood volume). Along with the enlargement of right cardiac features, between 40% and 65% of patients have a posterior and leftwards displacement of the superior attachment of the septum premium relative to the septum secundum, resulting in the apex of the heart not being formed by the left ventricle but the right ventricle only. Because the left ventricle is not functional, pulmonary venous return must pass to the right atrium. This occurs either through an atrial septal defect, a stretched foramen ovale, or, in rare cases, by an anomalous pulmonary venous connection. Therefore, the right ventricle must maintain both pulmonary and systemic output [1]. The pulmonary orifice and main pulmonary artery are usually always enlarged and communicate with the descending aorta via the ductus arteriosus (connecting branch between the pulmonary arteries and aorta not seen in normal cardiac anatomy). Maintaining the presence of the ductus arteriosis is essential in attaining systemic perfusion. Otherwise blood would continuously circulate from the lungs to the heart and to the lungs again, not undergoing systemic circulation. The relative ratio of pulmonary 5 to systemic blood flow depends on the delicate balance between pulmonary and systemic vascular resistances. If pulmonary resistance is too low, oxygenated blood will not undergo systemic circulation. The pathologic ailment of children with HLHS is an elevated arterial oxygen saturation resulting from high pulmonary blood flow, and thus marginal systemic perfusion resulting in metabolic acidosis [1]. 2.1.3 CAUSE The embryologic cause of HLHS is not fully known, however is thought to most likely result from either a reduction of left ventricular inflow or left ventricular outflow during development. Theoretically, a displaced septum primum may limit left ventricular inflow by obstructing the normal shunting of inferior vena cava blood through the foramen ovale to the left ventricle. This decrease in blood flow may result in a small left atrium, mitral valve, left ventricle, aortic valve, and ascending aorta. Other possible causes of HLHS include a congenitally small or absent foramen ovale and abnormalities of the mitral valve [1]. 2.1.4 CLINICAL EPIDEMIOLOGY While the incidence of HLHS is relatively low (1.4-3.8% of congenital heart disease), it has been reported to cause 23% of deaths in the newborn period. Approximately 1440 babies are born each year in the United States with HLHS. Because the disease is rare, about 20 of those cases are treated at Vanderbilt University Medical Center each year. There is an approximate 75% 3-year survival rate as children born with HLHS undergo surgery for this disease [1]. Children are diagnosed using fetal echocardiography, and in cases where HLHS is diagnosed sufficiently early, many parents choose to terminate the pregnancy. In the cases where HLHS presents itself within 24 hours of birth, it is usually because of severe obstruction to blood flow at the interatrial level. With this ductal impediment the patient 6 develops metabolic acidosis and supportive treatment is necessary. Outside of the womb, electrocardiograms often reflect the underlying pathology showing no left ventricular signal [1]. 2.2 CURRENT TREATMENTS 2.2.1 DRUG TREATMENTS There are no drug therapies available to treat HLHS, however there are treatments that increase pulmonary resistance, thereby increasing systemic perfusion. Neuromuscular blocking agents accomplish this, and are administered preoperatively [1]. 2.2.2 RECONSTRUCTIVE SURGERY Goals of the reconstructive approach are to ensure systemic perfusion in the absence of a ductus arteriosus and to prepare the pulmonary vascular bed for an ultimate modified Fontan operation. There are three stages involved in the surgery, with each being very intensive and pervasive. The first stage of the three-step surgery is a surgical technique that reduces the inadequate supply of oxygenated blood to the body by placing in aortiopulmonary shunt. This allows blood to circulate from the right ventricle, through the pulmonary arteries, and consequently through the shunt and to aorta. After this first stage, the right ventricle is volume loaded and generates systemic pressure. This surgery has a mean survival rate of 73% for a 30-day hospital stay. Postoperatively, complications might occur as the aortic branch becomes obstructed (either in the distal or proximal arch). If this happens, immediate recognition is critical for the child’s well being. Another potential complication is the development of rapidly progressing cyanosis (blue or purple discoloration of the skin due to inadequate oxygenation) [1]. 7 The second stage is called a hemi-Fontan or bi-directional Glenn shunt surgery, and is performed at about 6 months of age. In this surgery, the heart is exposed through a midline sternotomy. The superior vena cava and right pulmonary artery are dissected free, and a cardiopulmonary bypass is performed. Significant complications include transient superior vena cava syndrome, pericardial effusions, pleural effusions, phrenic nerve palsy, and death. The operative survival rate following hemi-Fontan is approximately 94% [1]. The third stage of the reconstructive surgery is the Fontan operation. This is performed approximately one year after the hemi-Fontan surgery. This procedure involves remodeling the placement of the superior and inferior vena cava. Approximately 45% of patients develop significant serous effusions, resulting in prolonged chest tube drainage post-operatively. The survival rate for the Fontan operation is 90%, with the majority of patients described as doing well from a cardiovascular and developmental standpoint [1]. 2.2.3 HEART TRANSPLANT The other method of treating HLHS is to perform a heart transplant. The main problem with transplantation is the availability of donors. If availability was higher, this method would be the dominant treatment option because operative survival for children who undergo transplants is excellent. However, between 10 and 40% of children with HLHS either undergo staged palliation or die while waiting for a heart. Thus, alternative solutions are needed [1]. 2.3 DESIGN GOALS The goal of our design is to eliminate the first two steps of reconstructive surgery while at the same time ensuring adequate systemic blood flow is achieved. Because the relative ratio of pulmonary to systemic blood flow depends on the balance between 8 pulmonary and systemic vascular resistances, our device focuses on this relationship for treatment solutions. It is important to understand that when pulmonary resistance is too low oxygenated blood will not be circulated in sufficient amounts to the body. Thus, we have proposed a device that will increase the pulmonary resistance, thereby increasing the flow of blood through the ductus arteriosis and increasing oxygenated systemic blood flow [3]. 3. METHODOLOGY 3.1 TIMELINE We began research and brainstorming HLHS in December of 2002. The completion date for this device is April 22, 2003. In between these dates a consistent amount of work was completed each week. The first couple weeks were spent conducting research on HLHS and talking to Dr. Doyle about possible solutions. After intensive research, we acknowledged the complexity of our problem and realized the solution would not be easily attained. Moving from complex to simple approaches, we determined the design of our device by early February, 2003. Dr. Doyle was clear in defining the parameters of the device and the environment in which it will reside, and after weighing our alternative solutions we determined Nitinol as the most feasible material for this model. Progress in our prototype creation was halted by our difficulty in finding a device in which we could test the effectiveness of our design. Because calculations were 9 complicated and solving this problem has never before been attempted with this approach, the variable needed to solve for the exact dimensions of the device had to be obtained via in vitro testing. Finding and eventually creating a conical device was a slow process. After a week of shopping around Nashville, another week was taken to create a CAD drawing of the device to be sent to the NCIIA. From this point in time, another two weeks was spent waiting for the arrival of the prototype. Because of this delay in time, we were unable to complete the testing we had hoped to have originally finished to solidify the correct dimensions for the device. Ultimately, we concluded that in vitro testing would provide inconclusive results due to the unknown variables present in the testing design, such as availability of pulsating flow and inability to model vessel wall characteristics due to the static environment of the pipe. 3.2 DESIGN AND PROTOTYPE 3.2.1 BACKGROUND Our device uses fluid dynamics of the heart and circulatory system to solve for inadequate systemic blood flow, and because we have not had extensive fluid dynamics courses, we had to seek the help of Dr. Mark Stremler (ME department) and Craig Russell (ME 2003). Their fluid dynamics equations to solve for the dimensions of the nozzle are included below: One source (1) with three exits (2,3,4) Q1 = 5*10-5 m/s (flow of blood from right ventricle to pulmonary arteries) Q3 = Q2 +Q4 (same amount of blood goes into lungs as organs) d2 = 0.0035 m 3 Find: size of conical nozzle Solution: Conservation of mass: Q1 = 2v2A2 + v3A3 5*10-5 = 4 v2A2 For single nozzle: v2 = Q2/(d22/4) 4 2 1 10 v2 = 1.3 m/s conservation of energy: * look at single nozzle v2 = vi i e Q2 = Qi Qe = 1.25*10-5 m3/s Bernoulli equation—assume incompressible, inviscid flow along streamline: Pi + ρvi2/2 + gzi = Pe + ρve2/2 + gze + hL Pe – Pi = ρ(vi2 – ve2)/2 Need ΔP ΔP = 1(1.32-ve2)/2 ve2 = ? Solve for Ae from Ae = Q/ve2 As can be seen, the equations resulted in an unknown variable, ΔP. This is the only missing link, and solving for this would enable us to calculate the exact dimensions of our device. This would ensure the correct resistance of flow through the nozzle, and thus backflow of blood into the systemic arteries. This is a pressure difference that has never before been measured, nor could be measured at this stage in vivo. This is primarily because this device has never before been designed and thus the need for this measurement has never been expressed. While the blood pressure through the pulmonary arteries is estimated to be 20 mmHg, we cannot estimate how large the pressure drop will be across the device. 3.3 TESTING 3.3.1 METHODS With the prototype that we received from the NCIIA, we completed flow testing by running water through the device and measuring the flow difference across the device. Preliminary measurements were made, and to further solidify the results we have suggestions for future testing. Ultimately, testing should be done in vivo, primarily in animals, to determine the pressure drop actually using Nitinol wire. Because the development of the prototype 11 was such a long process, we were unable to reach this step in an in vitro model, and ultimately the actual pressure drop will be best assessed in an in vivo model where pressure differences associated with the cardiac cycle are in practice. 4. RESULTS 4.1 DESIGN 4.1.1 CONE DESIGN After our first meeting with Dr. Doyle, he recommended that we use some form of a cone (nozzle) device to impede the flow to the pulmonary arteries. After exploring other options and presenting them to Dr. Doyle, we 6-10 mm decided that the device should have a cone shape, as shown in figure 2. Among the reasons for our conclusion were the effectiveness of the device in impeding flow, Figure 2: The shape of our device. the ease at which it could be placed in the arteries, and the low health risks it provided for the patient. After conducting some tests in which water was run through the device, it was shown that the cone did indeed impede flow. Although a crude method of testing, using a bucket and a stop watch to measure the flow rate indicated to us that the first and main objective of the design was met, impeding the flow. Another factor that must be taken into account is the pressure drop across the device, which would in turn allow us to calculate the diameter of the smaller opening in the device. This pressure drop is something that is currently not possible to measure because we do not have an in vivo model. Having a more realistic model of the system would allow us to calculate the pressure drop correctly and determine the exact dimensions of the device [10]. 12 A study conducted by the University of Tel Aviv in conjunction with the Department of Surgery at the University of Louisville determined that altering the flow of the systemic and pulmonary flow improved the oxygen saturation in the blood going through the systemic arteries [8]. This design is based on the same principle in that we are trying to improve the systemic blood flow in hopes of improving the length and quality of life for the infant. Dr. Doyle predicts that a one liter per minute per meter squared blood flow rate through each of the pulmonary arteries would be sufficient to attain reasonable systemic blood flow rate and oxygen saturation; however, this theory has not been tested and is something that must be considered in the future before placing the device inside a patient. This sort of testing would also require an in vivo model such as a pig or sheep. However, using an animal model for testing requires FDA approval and would be a process the next group will have to accomplish due to our time limitation. Another major design issue was the implantation of the device. Dr. Doyle required the device to be implanted using a catheter. This in turn would be minimally invasive and deployment of the device in the pulmonary arteries would not be too complex of a procedure to complete. The cone shape of the device met these criteria best in comparison to the other designs that were considered. First, the shape of the cone would be easily retained from Nitinol due to its simplicity. This fact is very important or else the patient would have a defective device in place, which could cause serious injury or even death to the patient. Furthermore, it could be easily placed in the artery. Dr. Doyle intends to use a guidewire to ensure the cone is placed into the pulmonary artery (see figure 3). The wire would be placed in the catheter and then inserted into the pulmonary artery, without having the catheter leave the ventricle. Next, the Nitinol wire would be released from the catheter and retain its shape. It would then reach the pulmonary arteries as the guidewire uses the blood as a force to push it along 13 to its destination. The device would then fit snugly into the artery with scar tissue eventually forming around the device, keeping it in place. Again, an animal model would allow us to assess the effectiveness of the method of implantation for this device. Lastly, after considering all the other various designs, the cone design would provide the least amount of harm to the patient. First, it Figure 3: Method of implantation of device into the pulmonary arteries [11]. would not cause hemolysis by impeding the flow of blood, like the mesh device previously proposed. Secondly, the amount of tissue damage that would be caused by the device would be minimal due to the shape and smooth texture of the device. The safety issues of this device are discussed below in the section entitled, “Safety Analysis.” In addition, we decided that the nozzle should be made out of Nitinol wire since it is a form of memory wire. Having this design characteristic would ease the method of implantation since the wire could be stretched, placed inside a catheter, and then released into the artery, after which it would presume its conical shape. In addition, Nitinol is a material that is biocompatible. Hence, a very slight immune response would be initiated by placement of this device inside the patient. In fact, Nitinol is already being used in cardiology as a material for stents, so its biocompatibility is already acceptable and useable [6]. 4.1.2 OTHER DESIGNS Three alternate designs were considered: having the nozzle placed inside a stent, having a “bow-tie” shaped device, and a mesh-like device. The first option, placing the nozzle inside the stent was considered more for placement issues than flow 14 resistance. Considering the fact that stents do not move much, if at all in the arteries where they are attached, we were hoping to take advantage of this and place our nozzle inside this stent. However, Dr. Doyle told us that placement of such a device would be too complicated and almost impossible. The chances of having the device deployed correctly inside the stent are low and there could be complications such as having the Nitinol wire getting stuck to the stent when it is retaining its conical shape. The other option, a “bow-tie” shaped device, would provide the same problems as having the device placed inside a stent. The complication would lie in the fact that the device would have to be placed specifically in the artery since the two ends are the same size. Therefore, there would be the possibility of having the device not fit into the blood vessel. The shape of the device may pose a problem for its implementation using Nitinol wire because there would be a risk that the shape would not be retained once released inside the body due to the complicated structure. Lastly, we proposed having a mesh barrier placed at the opening of the pulmonary arteries to impede the flow. However, using a mesh device to impede the propulsive blood flow would cause hemolysis, the breakdown of red blood cells [3]. Of course, this device would cause severe health problems to the patient and would add to the problem as opposed to solving it. 4.2 SAFETY ANALYSIS There are many risk factors involved with the design of the device, as there would be with any medical device used on patients (see Appendix B). The first main risk would be the ability of the device to reach the pulmonary artery properly. The use of the guidewire should ensure that the device would reach its destination. Furthermore, the excellent training and expertise of Dr. Doyle decreases this risk even more. Since this risk is involved with the ability of the physician more than the device, we will not discuss 15 it in detail but will go more in-depth in regards to aspects of the design that we had control over during the design process and the risks involved. One of the main issues we had to look into was the risk of having the device severely damage the vessel walls. Although we can not know whether this event may occur until testing is performed, it is very unlikely to occur for two reasons. First, Nitinol wire is currently being used for stents, so it has been used in the arteries before and minimal damage has occurred. Moreover, the way the device is shaped minimizes the risk of puncture to the wall since the wire will be wrapped in a cone shape and so no part of the device will be in position to wound the blood vessel wall. Another safety issue that was investigated was the durability of the material used to create the device. Again, the risk level is very low since the device will not be in the patient for long, a duration of about eight months. As noted before, Nitinol wire is currently being used as the material for stents, which stay much longer in the body. Based on this information, we decided not to worry about the durability of the device after an extended period of time in the patient since there have been no problems with the resilience of Nitinol wire in the vascular system for extended periods of time [6]. The main issue of concern in this design is whether the device will retain its original form once released from the catheter. This is a possible risk for the patient and the only method of truly determining the risk level of this hazard would be to perform tests on an animal model. The probability of the Nitinol wire not retaining its shape is smaller if it is a newly manufactured wire, which would be the case for each patient. The key design factor was to ensure that the shape would be retained once the device was inserted in the body. Our simple design enables us to achieve this goal. All the risk factors involved in making and implanting this device were compiled on a program called designsafe. From this program, all the probabilities of the risks were determined to be fairly low; however, they were all taken into account for the 16 design process. As with any medical device, nothing is certain until the device is used on a patient, and even then the complete safety of the patient is not guaranteed; each patient is a special case. 4.3 ECONOMIC ANALYSIS At the current stage of the project, it is difficult to determine the price of the device exactly. The price of three feet of Nitinol wire is $6.80 for a wire with a diameter of 0.0051 inches. However, the exact dimensions of the device are not determined, so the total amount of wire required is still unknown and as a result, the total price of the device is unknown. Based on the price of the Nitinol wire and the small size of the device (it will have a large diameter of 6-10 mm), the price should be fairly cheap for the creation of the device. Most costs would be exhausted in the molding of the Nitinol wire to the conical shape. In terms of development, our group worked about fifteen hours a week for a total of fifteen weeks, which sums to 225 hours. A student hourly wage is $15/hour each; therefore, it would cost approximately $3375 for the engineering consultations. Unfortunately, the market potential for this device is not as exciting as other markets (such as cancer treatments or gene therapy) due to the fact that approximately 1440 babies are born with this disease each year in the U.S. [1]. Therefore, the demand for the device will be relatively low. However, because reconstructive surgery for HLHS can cost up to $100,000, finding a way to decrease these costs and bypass some of the surgical procedures involved is incredibly beneficial. As opposed to the medical costs that ensue while a child is undergoing the three-step surgery, the cost of implantation of our device is significantly less. The price of the three-step operation including the duration of hospital stays during this time can reach up to half a million dollars. With two of the surgical steps being eliminated and a noninvasive procedure being operated, hospital stays will be cut to a minimum and thus costs will be greatly decreased. The 17 price of the catheterization procedure and shorter hospital stay in the ICU for the implantation of the pulmonary resistive device will only cost approximately $15,00020,000. This is a minimum of 85% less in costs than the surgical procedure currently performed [3]. Another convincing point to investing in a device like ours is that it will save many lives since many of the infants die while waiting for a transplant. It is estimated that the value of a human life is $7,000,000, therefore, the investment of approximately $4000 to create a device that will save many human lives returns much more (in our opinion, human life is priceless) [5]. What is even more appealing to Vanderbilt University Medical Center is that it receives approximately twenty HLHS patients a year [3]. Therefore, investment in the pulmonary flow resistive device may pay even more dividends for VUMC than other medical centers that may have one or two HLHS patients a year. Since we have not reached the human testing stage or the patenting stage, we do not know the exact cost it would entail to patent the device and receive FDA approval for human testing. Moreover, monetary compensation may be needed for the human clinical trials, which would increase the price of development even more. These factors will have to be taken into consideration by next year’s group. 5. CONCLUSIONS As with most scientific or engineering experiments, the problem at hand usually becomes more complex than expected. Because no other group had previously tackled the design problems set forth in this project, the initial start-up process required significant time and effort. Thought the beginning steps of the project were slowprogressing and tedious, in the end we believe we met our objectives in developing a design that meets the needs of our set goals. 18 The first design objective was to make a device that would impede blood flow to the pulmonary arteries. This in turn would increase blood flow to the systemic arteries. Although no animal or human testing was conducted to verify this conclusion, it is safe to say, based on the testing we conducted using water, that the flow will decrease. The second objective was to make the device out of a material that is biocompatible. We have concluded that Nitinol is the right material to use due to its proven record of effectiveness in the medical instrument market for cardiology. Lastly, the Nitinol wire allowed us to design a device that meets our requirement of having a device that can be implanted using minimally invasive techniques (i.e., catheter). The main obstacle to overcome in proving the effectiveness of our device in impeding blood flow and finalizing the design specifications was solving the fluid dynamics calculations. We sought Dr. Mark Stremler’s advice; however, after calculations were completed we determined that we needed to know the pressure difference across the device while it is in the blood vessel to solve for the unknown smaller diameter of the conical device. Since no device has ever been created that would require this type of measurement to have been recorded previously and because this measurement could only be taken in vivo, we were unable to solve for this missing link. Therefore we were unable to determine the appropriate dimensions for the device to impede flow at the desired rate. 6. RECOMMENDATIONS We believe the next major step that needs to be taken in the design process is to find the pressure drop across the device. In order to do so, in vivo testing in animals would be required; possible animal models could be pigs or sheep. The next step would be to have clinical human trials, which would require FDA and IRB approval. Before that is completed however, a patent must be filed to guarantee that no one else has access to the design. Furthermore, the help of someone from the Mechanical Engineering 19 department is vital to the completion of the project due to the Biomedical Engineers’ insufficient knowledge of fluid dynamics. One last recommendation, which may provide some added insight to the design process, would be to create a computer simulation of the blood vessel with and without the device. However, the next group that may work on this should focus mainly on the previous suggestions mentioned earlier to ensure the complete success of this design project. 20 7. REFERENCES [1] Barber, Gerald. Hypoplastic Left Heart Syndrome. Structural Congenital Defects, section 3. [2] www.ucch.org/sections/cardio/new/hlhs.html; date accessed: January 30, 2003. [3] Dr. Thomas Doyle; Vanderbilt University Medical Center. [4] http://www.nemours.org/no/ncc/cardiac/crd1524.html; date accessed: February 25, 2003. [5] www.longevitymeme.org/articles/viewarticle.cfm?article_id=9&page=1; date accessed: April 18, 2003. [6] www.nitinol.com/4applications.htm; date accessed: April 18, 2003. [7] Sherwood, Lauralee. Human Physiology: From Cells to Systems. Fourth Edition. Brooks/Cole, United States. 2001 [8] Barnea, et al. Balancing the Circulation: Theoretic Optimization of Pulmonary/Systemic Flow Ratio in Hypoplastic Left Heart Syndrome. JACC. Vol 24, No. 5. November 1, 1994. p. 1376-81. [9] Pugh, Maureen B., ed. Stedman’s Medical Dictioary. 27th Edition. Lippincott Williams & Wilkins. Philadelphia. 2000. [10] Dr. Mark Stremler; Vanderbilt University School of Engineering. [11] www.wesleemedical.com/safetywedge.html; date accessed: April 7, 2003. 21