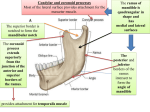
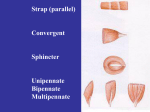
Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Gross: 8:00-9:00 Scribe: Sally Hamissou Friday, February 20, 2009 Proof: Sunita Jagani Dr. Salter Temporal and Infratemporal Fossae Page 1 of 7 Abbreviations: MMA = Middle Meningeal Artery, TMJ = Temporomandibular joint, CN = Cranial Nerves Temporal and Infratemporal Fossae I. Temporal and Infratemporal Fossae [S1] a. This is a dissection that can be carried out easily within the prescribed time and is important. b. Trigeminal nerve is included, we have already looked at V1, today we will look at V3, and V2 will be discussed next week when we talk about the pterygopalatine fossa. II. Temporal Fossa [S2] a. Depression in side of head and is bounded by superiorly 2 temporal lines and inferiorly by supramastoid crest b. All of this is the temporal fossa c. Floor: frontal, parietal, vertical portion sphenoid, squamous portion temporal bones (remember there are 5 parts) d. 4 cm superior to zygomatic arch is an important area, referred to as a pterion i. Deep to it lies the MMA- if you lacerate the skull, you may lacerate the vessel and you will have an epidural hematoma III. Temporal Fossa [S3] a. Temporal lines i. Superior Temporal Line 1. Attachment of temporalis fascia ii. Inferior Temporal Line 1. Superior attachment of temporalis muscle 2. The temporalis muscle arises from this fossa but has superior attachment to the inferior temporal line IV. Netter Skull View [S4] a. The temporal fossa is bounded superiorly by the two temporal lines and bounded inferiorly by the zygomatic arch, superficially speaking. If we take a horizontal section, you would find the inferior aspect of the temporal fossa more deeply located than the zygomatic arch and that would be represented by removal of zygomatic arch. b. Removal of Zygomatic Arch allows one to view the deep, inferior boundary of temporal fossa deeply represented by the infratemporal crest of the greater wing of sphenoid bone. c. Bones and what attaches to them are very important d. Notice irregular border- temporalis muscle arises from that i. Deep temporal nerves and vessels run in between the juts of bones. The roughened edges and these passage ways are filled with deep temporal vessels and nerves, the temporalis muscle arises there. V. Infratemproal Fossa [S5] a. “An irregular space inferior and deep to the zygomatic arch and posterior to the maxilla” RTW b. The fossa is inferior to temporal fossa VI. Surgical Access to Infratemporal Fossa [S6] a. Take off ramus of mandible, that is where the infratemporal fossa is b. Here is the surgical access to infratemporal fossa, accessed by mandibular fossa. c. The masseter muscle lies right in here. d. Today in the dissection, we are asked to remove masseter muscle from zygomatic arch, and when we reflect it inferiorly, you will find the nerves and vessels to the masseter to reach the masseter muscle by way of the mandibular notch and it also allows for surgical access to region as well. VII. No Title [S7] a. However, removing the zygomatic arch & the ramus of the mandible allows greater access to the infratemporal fossa- this is what we will accomplish in the laboratory today VIII. Netter Skull View [S8] a. Remove zygomatic arch and ramus of mandible (which is the lateral border), and we encounter the infratemporal fossa IX. Infratemporal Fossa Boundaries [S9-10] a. Medial: lateral surface of lateral pterygoid plate i. The lateral surface of the lateral pterygoid plate is the medial boundary here b. Lateral: ramus of the mandible c. Superior: zygomatic arch and horizontal part of greater wing of sphenoid, including infratemporal crest d. Inferior: is open e. Anterior: space posterior to the maxilla f. Posterior: temporal bone specifically the styloid process- one of five portions of the temporal bone. i. The deep portion or deep lobe of parotid gland wraps itself around styloid process, so its possible that the gland is a part of infratemporal fossa X. Netter Skull View [S10] Gross: 8:00-9:00 Scribe: Sally Hamissou Friday, February 20, 2009 Proof: Sunita Jagani Dr. Salter Temporal and Infratemporal Fossae Page 2 of 7 a. What we will see in lab filled with the components of the infratemporal fossa XI. Communications of Infratemporal fossa [S11-12] a. Communicates medially with pterygopalatine fossa via pterygomaxillary fissure i. Here is the maxilla, this is the pterygoid process of the sphenoid bone, so the fissure in between is the pterygomaxillary fissure ii. Pterygomaxillary fissure leads to the pterygopalatine fossa b. [S12] Communicates anterior/superiorly with orbit via inferior orbital fissure i. Inferior orbital fissure leads to the orbit ii. If one injects too much anesthetic into the infratemporal fassa, some will leak through inferior orbital fissure and manifest as eye muscle paralysis, as diplopia because of the communication here. c. Communicates superiorly with the middle cranial fossa through both the foramen ovale & the foramen spinosum d. Communication here with pterygopalatine fossa through pterygomaxillary fissure (you should realize these words and how you associate these words is important) remember pterygopalatine fossa, and the fissure that leads to that is the pterygomaxillary fissure e. Fossa also communications inferior orbit through the inferior orbital fissure. i. More than just an anesthetic can get in tooth region. ii. Also a venous channel that runs into region. XII. Holes in Roof [S13] a. Roof/Tangential view b. Foramen of roof communicate with the middle cranial fossa via the two foramen: Foramen spinosum and ovale, which lie in the roof of the infratemporal fossa c. Points out the pterygomaxillary fissure and the inferior orbital fossa. d. Foramen Spinosum i. Called spinosum because ‘spine of sphenoid’ to which a ligament attaches and we will show you the sphenomandibular ligament lies there ii. Spine of sphenoid sits right there near the foramen, you should know exactly where the spine of the sphenoid is XIII. Figure of the Face [S14, 15] a. Components of the infratemporal fossa b. Take off venous plexus, you can see the muscles of mastification, V3, maxillary artery, and sphenomandibular ligament- these are the main components. XIV. Primary Contents [S16] a. Muscles of Mastication i. How many? 4 b. Maxillary Artery there are two parts divided into 3 parts by a muscle. i. We have talked about arteries that have been divided into three parts because of muscles like Anterior scalene muscle divides subclavian artery into 3 parts, proximal, posterior, distal c. Pterygoid Plexus of Veins i. Important to dentists, abscesses from maxillary and mandibular teeth may drain into the pterygoid plexus of veins and concern is where it goes from there? d. Mandibular Nerve (V3) i. About all that we will see in the infratemporal fossa, we will see a small branch of V2. e. Chorda Tympani Nerve- looks like a cord in the middle ear, after it passes through middle ear into the infratemporal fossa, and carries on different modalities. f. Otic Ganglion- can’t identify, even harder to tag on practicals and has never been tagged, and he doesn’t expect us to find the otic ganglion. g. Sphenomandibular Ligament i. Can be seen and we will talk about it. h. Deep Lobe of Parotid Gland i. Nerve that runs through the gland is the facial nerve. If one injects into infratemporal fossa too much anesthetic, it may make its way into parotid gland and paralyze the facial nerve and the muscles supplied by the nerve. ii. Local dentist called and had paralyzed the inferior alveolar nerve of his patient. This is an important issue because if you inject too much anesthetic, it can produces anesthesia in areas that supply the inferior alveolar nerve, lingual nerve, and also the facial nerve, so one has to be careful of that. XV. Muscles of Mastification [S17] a. Temporalis i. Origin: temporal fossa Gross: 8:00-9:00 Scribe: Sally Hamissou Friday, February 20, 2009 Proof: Sunita Jagani Dr. Salter Temporal and Infratemporal Fossae Page 3 of 7 ii. Insertion: into the coronoid process of the ramus of mandible and inserts all the way down posterior to the third molar. 1. The temporalis insertion is important 2. It’s a big muscle to remove in lab because of it’s origin. iii. Action: elevates mandibular and - primary elevator of the mandible and closer of orifice. Posterior fibers (run horizontally) retract mandible, so if the mandible was protruded out, you would use the posterior fibers to bring it back. So it is a retruder or retractor of the mandible. b. Masseter i. Origin: zygomatic arch, has a superficial origin, and the muscle peaking out deeply is the deep head of the masseter muscle, we won’t be focusing on there being a superficial and deep head of the masseter, but we will be identify this in lab. ii. Action: Elevates mandible XVI. Medial and Lateral Pterygoid Muscles [S18] a. Deeply lined muscles b. Lateral Pterygoid Muscle i. Superior head arises from the roof of infratemporal fossa ( roof formed by the sphenoid bone). Since muscle arises from greater wing of sphenoid and attaches to the disk of the TMJ and the superior head is sometimes referred to as sphenoid meniscus head. ii. Inferior head arises from the lateral surface of the lateral pterygoid plate. It is the larger of the 2 heads and arises from lateral surface of the lateral pterygoid plate. You can’t see the medial boundary of the infratemporal fossa of the pterygoid plate because it is covered up by the muscle. 1. The inferior head runs and attaches to fovea (depression) in the neck of the mandible and this may be tagged on the next exam c. Medial pterygoid muscle i. Deep head arises from the medial surface of lateral pterygoid plate. The lateral surface of the lateral pterygoid plate arises is the lateral pterygoid muscle. Arising from the medial surface of the lateral pterygoid plate is the medial pterygoid muscle. ii. Superficial head (we will have to identify this) arises from the maxillary tubercle. Insertion is the same, into the internal aspect of the angle of the mandible. Here is the masseter muscle inserting into the external aspect of the ramus of mandible, particularly at the angle and you can see the internal or medial pterygoid doing the same thing. iii. Some dentist refer to this as pterygoid masseteric sling, there is the masseter here and underneath the angle is the medial pterygoid maxillary sling. XVII. Muscles involved in Mastification (Deep) [S19] a. Lateral Pterygoid- superior & inferior heads- protrude & depress mandible (by the inferior head) i. The inferior head depresses the mandible and it doesn’t take much to depress the mandible because gravity will bring it down. b. Medial Pterygoid- deep and superficial heads-- they elevate the mandible. c. [SQ] clarification on lateral pterygoid muscle. [A]: both heads might protrude the jaw and the inferior head depresses it. XVIII. Another View of the Pterygoid Muscles and Another Function [S20] a. Another view and another function of the pterygoid muscles: Here is the lateral pterygoid and medial pterygoid muscles, they rise from opposite sides of the lateral plate of the pterygoid process of the sphenoid bone. b. Arising from the lateral surface of the lateral pterygoid plate is the inferior head of the lateral pterygoid. The medial surface of lateral pterygoid plate has the origin for the deep head of the medial pterygoid muscle. XIX. Another View & Function of the Pterygoids [S21] a. When both muscles contract unilaterally, as in grinding, the mandible moves horizontally in the contralateral direction. b. If the muscles contract, it will pull right side of mandible over to the other side, if it contracts and shortens it will pull the mandible, and therefore the other side of the mandible will deviate to the other side, so the muscles contract and will pull the right side of the mandible to the contralateral side c. If V3 injured or the muscles themselves are injured, so the muscle contralateral side will pull mandible over to the contralateral side, like the effect of a V3 lesion. XX. Effect of V3 Lesion [S22] a. Opened jaw deviates towards the side of lesion. XXI. Maxillary Artery [S23, S24] a. 2 terminal branches around the neck of the mandible, we may have seen these in the dissections already. b. Around the head/neck of the mandible, the maxillary artery terminates into its two branches, superficial temporal and maxillary artery. Gross: 8:00-9:00 Scribe: Sally Hamissou Friday, February 20, 2009 Proof: Sunita Jagani Dr. Salter Temporal and Infratemporal Fossae Page 4 of 7 XXII. Remove Ramus of Mandible [S25] a. If we remove the mandible, we can see more of the maxillary artery. XXIII. Maxillary Artery [S26] a. 3 parts are designated because of the relationship of the second part of the artery to the lateral pterygoid muscle. b. 2/3 of the time, the second part lies superficial to the lateral pterygoid muscle and 1/3 of the time it lies deep to the lateral pterygoid muscle. c. 1st part (mandibular)- part proximal to lateral pterygoid i. Branches enter foramina/canals, remember that! d. 2nd part (pterygoid) i. All muscular branches- artery to masseter, buccinator, and pterygoid muscles all come off the second part of the maxillary artery ii. Lies superficial to the lateral pterygoid muscle but sometimes it is deep to it and you may see both in the cadavers. e. 3rd part (pterygopalatine)- more distal or medial to lateral pterygoid muscle. i. Lies within the pterygopalatine fossa XXIV. 1st part --Mandibular Part [S27] a. Concentrates on MMA, Inferior Alveolar Artery, and Accessory MMA. b. Inferior alveolar artery i. Passes through the mandibular foramen and passes with the inferior alveolar nerve. Sometimes it is damaged during the TMJ dissection/surgery. c. Deep to lateral pterygoid muscles: two branches- MMA and accessory MA d. MMA passes through the foramen spinosum, the middle cranial fossa, and the holes in the roof communicate the middle cranium fossa with the infratemporal fossa. e. The accessory MMA passes through foramen ovale, so if you see an artery passing through the foramen ovale, then it is the accessory MMA, no matter where it comes from. It can come from MMA or second part of the maxillary artery. XXV. Mandibular Nerve (V3)- Lateral View [S28] a. MMA i. Seen after removal of lateral pterygoid muscle. ii. Take out lateral pterygoid muscle in order to see most of MMA. iii. MMA runs in between the rootlets auriculotemporal nerve, we will identify it as being a large structure in the infratemporal fossa iv. Usually passes in between the two roots but it may or may not do that. XXVI. 2nd part –Pterygoid Part [S29] a. Located superficial to lateral pterygoid muscle b. All branches are muscular i. If we see an artery going to muscle of the buccinator or temporalis muscle and ask you from what part of the maxillary artery do they originate, it is from the 2nd part because all branches from the 2nd part are muscular. c. These are the deep temporal arteries that enter the deep aspect of the temporalis muscle. d. This is the buccal artery that runs with buccal branch of V3. These are branches to the pterygoid. XXVII. 3rd part-Pterygopalatine Part [S30] a. 3rd part Is located in the pterygopalatine fossa and the fossa is medial to pterygomaxillary fissure. b. Today we will only see one branch of the third part of the maxillary artery, which originates within the pterygopalatine fossa, extends back out of the fossa, and extends thus. c. Posterior alveolar nerves which runs with the posterior superior alveolar artery, which you dentists will anesthetize on occasion. XXVIII. Blood Supply [S31] a. Here is the maxillary artery and the Inferior alveolar is seen on the slide also. b. From 1st part various branches i. MMA seen here, and you will have to remove a lot of lateral pterygoid to see expanse of the artery. ii. Inferior alveolar artery and accessory MA is not seen here but we will see it in the lab downstairs. c. From 2nd part all muscular branches d. From 3rd part Posterior superior alveolar Artery i. The only one we will have to identify today, it runs and enters foramen on posterior aspect of superior alveolar arch, the arch is part of the maxilla. This is an artery that enters the superior/posterior aspect of the superior arch. XXIX. Pterygoid Venous Plexus [S32, S33] Gross: 8:00-9:00 Scribe: Sally Hamissou Friday, February 20, 2009 Proof: Sunita Jagani Dr. Salter Temporal and Infratemporal Fossae Page 5 of 7 a. When you take off ramus of mandible, the very first thing we will see is the pterygoid venous plexus b. Lateral pterygoid muscle is enveloped by pterygoid venous plexus c. The venous plexuses drains lower and upper teeth. d. Abscess from teeth, both mandible and maxilla can pass through the venous plexus XXX. Danger Triangle of Face [S34] a. Normally blood drains from medial angle of the eye, nose and lips into facial vein, via the deep facial vein back to something else. b. Because facial veins and tributaries don’t have valves, blood can drain deeply into pterygoid plexus and eventually into the cavernous sinus XXXI. Cavernous Sinus Venus [S35] a. Points out : Superior ophthalmic vein, Inferior ophthalmic vein, Angular vein (beginning of facial vein), Facial vein, Deep facial vein (connects facial vein to pterygoid plexus), Pterygoid venous plexus, Cavernous Sinus, Superficial Temporal Vein joins with the Maxillary Vein to form the retromandibular vein b. Routes for infection- infection and bacteria from the face, angular vein can lead to the superior ophthalmic vein, carries infection back to cavernous sinus. The veins don’t have valves. c. Inferior ophthalmic runs in inferior aspect of the orbit, runs back and connects to cavernous sinus, bringing about thrombosis of the cavernous sinus. d. Facial vein carries infection by deep facial vein to pterygoid plexus of veins and eventually to cavernous sinus. e. Pterygoid plexus of veins drains laterally via maxillary vein, the maxillary vein joins the superficial temporal vein to form the retromandibular vein. f. And there is the IJV XXXII. Mandibular Nerve V3 [S36] a. Very important b. Points out V1, V2, V3 XXXIII. CN (Motor and Sensory Distribution): Schema [S37] a. V3 eventually goes through the mandible so mandibular branch XXXIV. Mandibular Nerve [S38] a. Four Areas of Supply: i. Muscles derived from first pharyngeal arch 1. 4 muscles of mastification. Also the Anterior belly of digastric and mylohoid muscles are supplied by nerve of mylohyiod V3. 2. 2 tensor muscles: tensor to palate and tensor to tympanic membrane 3. 8 muscles are supplied by V3: 4 muscles of mastification, 2 tensors, and nerve to mylohyoid ii. Mandible via inferior alveolar nerve 1. Supplies the mandibular teeth 2. Enters alveolar process of mandible iii. Cutaneous via auriculotemporal, buccal and mental nerves; 1. 3 cutaneous nerves that supply skin: auriculotemporal nerve, buccal nerve, and mental nerve 2. Supplies skin, teeth, and muscles iv. Tongue (anterior 2/3’s), Floor of mouth, Vestibular mucosa and Mandibular gingiva (oral & vestibular) via lingual, buccal and mental nerves 1. General sensory fibers, PPTT (pain, pressure, temperature, touch) 2. Also does various branches that supplies floor of the mouth, the vestibular mucosa, and mandibular gingival (both oral and vestibular) via lingual, mental and buccal nerve. XXXV. Mandibular Nerve (SVE, GSA) [S39] a. V3 has GSA and SVE in motor root of trigeminal nerve b. Trunk has nerves to medial pterygoid muscles and the two tensors-not as important i. Anterior Division– all motor branches except the buccal nerve, goes anteriorly 1. All motor except buccal nerve ii. Posterior Division– all sensory branches except for Nerve to mylohyoid. 1. All sensory except nerve to mylohyoid XXXVI. Anterior/Posterior Division Diagram [S40] a. Points out anterior and posterior division of V3 i. Posterior division- inferior alveolar nerve is mainly sensory from mandibular teeth but gives off nerve to mylohyoid b. First branch off posterior division is auriculotemporal nerve i. When looking for the nerve and we see one that is large and runs horizontally within the superior aspect of the infratemporal fossa, that is the auriculotemporal nerve. Gross: 8:00-9:00 Scribe: Sally Hamissou Friday, February 20, 2009 Proof: Sunita Jagani Dr. Salter Temporal and Infratemporal Fossae Page 6 of 7 ii. It is large and runs a horizontal course and extends vertically, nerve runs posterior to TMJ. Main sensory to TMJ, in addition to being cutaneous, it also supplies the joint, remember the relationship to MMA. c. Inferior alveolar Nerve (end of the nerve as the mental nerve) runs through the ramus of the mandible i. Sensory from mandibular teeth and somatic motor and has the only motor branch of the posterior division (Nerve to mylohyoid muscle) ii. We have seen it supplying the mylohyoid and anterior digastric of the neck and we will see it exiting the from inferior alveolar nerve and the groove on the mandible where the nerve to the mylohyoid runs, and you should know where the groove is. d. Nerve to mylohyoid i. Special visceral motor e. Lingual Nerve branch of V3 i. Sensory branch for tongue, lingual gingiva & roof of mouth ii. Submandibular ganglion hangs from the lingual nerve f. Chorda tympani i. Enters lingual nerve and runs with lingual nerve ii. Carries taste to anterior 2/3 of tongue because that is where the lingual nerve runs iii. In middle ear looks like a cord, passes out the middle ear, through the petrotympanic fissure (have to know where that is), passes out and enters infratemporal fossa and joins with the lingual nerve. iv. Posterior contribution to lingual nerve is via the chorda tympani nerve carrying taste and parasympathetic fibers to wherever the lingual nerve goes v. Branch of CN VII vi. GVE and SVA join with general somatic fibers, the lingual nerve, and distributes downstream XXXVII. Anterior Division [S41] a. All motor branches except of one branch. These are the motor branches: temporalis, lateral pterygoid. Deep temporal branches because they end of deep aspect of temporalis muscle. b. Buccal nerve sensory portion, cutaneous i. If we are careful, there are two heads of lateral pterygoid muscle, notice the buccal nerve passes into the infratemporal fossa in between the two heads of the lateral pterygoid muscle into the fossa ii. Inferior alveolar and lingual nerves may be seen passing between the medial and lateral pterygoid XXXVIII. Mandibular Nerve- V3 Lateral View [S42] a. Three cutaneous nerves of V3: auriculotemporal nerve, buccal nerve as it passes in between the 2 heads, and mental nerve. b. Forms dermatome pattern on the face of the individual. XXXIX. Chorda Tympani [S43] a. Branch off facial nerve, can see facial coming out of the stylomastoid foramen b. (Medial View) Seen in the ear as a cord, passes into a canal, comes out of petrotympanic fissure, associates with lingual nerve and carries SVA (taste) and parasympathetic (GVE) to submandibular and sublingual glands c. Otic Ganglion- parotid gland, innervates the parotid gland, parotid is around the ear and otic is associated with gland around the ear. XL. Otic Ganglion Scheme [S44] a. Dr. Tubbs will talk about this later b. Tympanic branch off 9th nerve, which comes off just as it passes through the jugular foramen. Gives off the tympanic branch, goes into the middle ear, breaks off into plexus of nerves around the middle ear. If you have pain in the middle ear, the pain is because GVA sensations. c. From the inner ear, lesser petrosal nerve is continuation of tympanic branch of 9, passes through the foramen ovale, enters the otic ganglion, synapses on otic ganglion, postganglionic fibers pass with the auriculotemporal nerve to the carotid gland (I think he meant parotid gland), seen here. XLI. Chorda Tympani Nerve and Otic Ganglion Figure [S45] a. Figure shows both the branch from CN 9 tympanic branch middle ear and joins otic ganglion b. Postganglionic fibers follow the Auriculotemporal nerve out of the gland and in addition shows the Chorda tympani nerve joining that. XLII. Sphenomandibular Ligament [S46] a. 1st pharyngeal arch and is a strong ligament, runs from spine of spheniod to the lingula. XLIII. Inferior Alveolar Nerve Block [S47] a. Inferior alveolar nerve entering the mandibular foramen and the nerve on the mylohyoid coming from the inferior alveolar nerve lies in its own groove on the mandible. b. Points out inferior alveolar nerve and lingual nerve. c. The inferior alveolar block utilizes the sphenomandibular ligament as a trough & the lingual as a guide to that nerve. Gross: 8:00-9:00 Scribe: Sally Hamissou Friday, February 20, 2009 Proof: Sunita Jagani Dr. Salter Temporal and Infratemporal Fossae Page 7 of 7 i. Inject anesthetics that go lateral to ligament, like a trough, and the ligament guides the anesthesia into the inferior alveolar nerve ii. What else might be anesthetized by the same anesthetic? The lingual nerve. d. So when a patient comes out of dental chair, tell them not to chew because lingual nerve is anesthetized, and anterior 2/3 of the tongue, so you can’t feel anything and you will bite down on your tongue, so it’s a mess. XLIV. Temporomandibular joint (TMJ) [S48] a. Modified hinge and synovial joint b. Articulating structures: head of the mandible, Condyle of Mandible, covered by fibril cartilage c. This is the meniscus or disc. d. This is the mandibular fossa, where the head of the mandible articulates with the intervening TMJ disc XLV. TMJ [S49] a. In lateral view, you can see the meniscus. b. [MIC OUT 51:36-51:57] c. When you depress the mandible, translation occurs and translation is protrusion of mandible that naturally occurs when one depresses. Depression takes place at 25 degrees worth, automatic translation in the form of protrusion, so depression of the mandible, depresses the mandible here. And in addition, the mandible will protrude because the pull of the lateral pterygoid muscle d. Articular eminence prevents the head of the mandible from going too anteriorly and sliding under the articular eminence, possible test question i. The head of the mandible can slide under the articular eminence and find itself a part of the infratemporal fossa, unwanted of course. e. Mandible slides, translates, protrudes, and depresses i. Depression occurs initially and then protrusion because protrusion permits depression f. Clicking or locking occurs if condyle rides too far anteriorly over eminence XLVI. Herpes Zoster (also called shingles) [S50] a. A lot of pain is associated with the skin of the patient’s face b. Which branch of what nerve? CN V3- it is the dermatome of V3 c. Is considered a response to a latent chicken pox virus located in the sensory ganglion d. If trigeminal nerve, it is the trigeminal ganglion or semi lunar ganglion or caesarian ganglion. All are names of trigeminal ganglion XLVII. Lab [S51] XLVIII. Inferior Head of Lateral Pterygoid [S52] a. We will remove ramus of mandible be careful not to remove the inferior alveolar nerve and vessels that pass through the mandibular foramen. b. Take a saw, chisel, and hammer the rest of the way and carefully remove it. c. Remove the neck of the mandible and cut the entire ramus d. When you look inside you will see the lateral pterygoid muscle and medial pterygoid muscle- on the figure you can see the superior and inferior head of the lateral pterygoid muscle e. What is this? The superficial head of medial and deep head f. Identify these two nerves. Which is the most anterior? Lingual nerve going to the tongue. This is the inferior alveolar nerve. Buccal nerve runs with the buccal artery. Buccinator muscle with the parotid duct passes through it g. Vessel that run deep temporalis muscle are the deep temporal vessels and nerves XLIX. Figure [S53] a. Please note: for this slide, he was reviewing the major nerves that were covered in the lecture and pointing them out in the figure b. When you remove lateral pterygoid, then you can see the MMA coming off and going through the foramen ovale, accessory MMA c. Auriculotemporal nerve i. The nerve is horizontal and MMA is associated with it ii. As it passes around the neck of the mandible, this is where the nerve is anesthetized during TMJ surgery because this is the main sensory supply to the joint d. Inferior alveolar nerve and branch coming off is the Nerve to the mylohyoid. The nerve entering the posterior aspect of the lingual nerve is the Chorda tympani nerve. [End 57:57]