Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
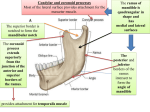
Dr. Sahar Taha, BDS, MS, Dip-(ABOD) Management of Temporomandibular Disorders and Occlusion, 6th edition Jeffery Okeson A complete medical and dental history should be taken. The history should be taken with the patient sitting upright in a quiet, relaxed atmosphere, ideally away from the treatment room. Use a questionnaire. Eye contact and a friendly, interested demeanor on the part of the clinician promotes body language that will enhance nonverbal communication. The history and examination should be directed toward the identification of masticatory pain and dysfunction. Masticatory pain is charachterized by two features: it originates in the masticatory structures and it is related to masticatory function. Some medical conditions might be associated with temporomandibular disorders like arthritis. The use of a questionnaire that the pt fills on their own can lead to a general evaluation of the condition then the dentist can focus on certain aspects of the history that pertain most to the condition and ask some more problem specific questions. Whenever a pain symptom is reported, special attention must be given to its location, behavior, quality, duration and degree. The more vaguely a patient localizes the pain, the more specific the examiner's inquiry must be. Report patient’s expectations. Report the social history of the patient. Some patients may want only to know what is their problem, others may want to relief their current symptoms only. Social history is very important as you can evaluate the psychological status of the patient. It is important to ask about the level of education, marital status, and employment. Seven critical questions as defined in the 1983 ADA President’s Conference on Temporomandibular Disorders: Difficulty in mouth opening? Pain or clicking in the jaw joint? Pain on chewing, yawning or wide opening? Pain in or about the ears or cheeks? A bite that feels “uncomfortable”or “unusual”? A jaw that “locks,” “gets stuck” or “goes out”? Noises in or from the jaw joints? It is also very important to ask when the dysfunction happened. History of previous treatment Other associated symptoms Symptoms like headache, neck pain, shoulder pain, or earache should be reported. Aims to detect masticatory dysfunction through examining: The muscles The joints The teeth Dentist either standing or sitting at the 12 o’clock position (range 11-1). The patient is semi-reclined or fullyreclined. The third position is probably the best. There is no pain usually associated with the function or palpation of a healthy muscle. The muscles can be examined by palpation or functional manipulation. When pain is felt during muscle palpation, it can be deduced that the muscle tissue has been compromised by either trauma or fatigue. Accomplished by the palmer surface of the middle finger, with the index and forefinger testing the adjacent areas. Soft but firm pressure should be applied with a slight circular motion. The patient is asked to classify the response to palpation into one of four categories (get away from subjectivity): 0= no pain felt at all 1= uncomfortable 2=definite discomfort or pain 3= evasive action or eye tearing, or a desire to not have the area palpated again. the temporalis muscle is divided into three functional areas. The anterior part is palpated above the zygomatic arch anterior to the TMJ. The middle part is palpated directly above the TMJ and superior to the zygomatic arch. The posterior part is palpated above and behind the ears. Superior and inferior attachments of the muscle should be palpated. The fingers are placed on the zygomatic arch then dropped down slightly to palpate the deep masseter just anterior to the TMJ. The inferior attachment (superficial masseter) is palpated on the inferior border of the ramus. This muscle is palpated at its insertion on the medial surface of the angle of the mandible. The fingers are placed on the inferior border of the mandible and rolled medially and superiorly. If uncertainty arises during palpation of this muscle, the pt can be asked to clench the teeth together, thereby, the medial pterygoid can be felt easier. A lot of false positive results for this method. This muscle is palpated intra-orally. It is best be seated in front of the patient. The index finger is placed in the maxillary buccal vestibule and the patient is instructed to close partially and to move the mandible to the side being examined. Having the patient partially close and moving the mandible to the site of palpation moves the coronoid process away from the site of examination. Palpation of this muscle leads to the highest false positive results. It is a narrow area and doing the palpation forcefully in the area may elicit pain. Sharp fingernails may also elicit pain. In addition, evidence suggest that this technique does not actually reach the attachment of the lateral pterygoid muscle to the lateral pterygoid plate. Therefore, this muscle can not be examined clinically. The discomfort caused by palpating this area is thought to be from the superior attachment of the medial pterygoid muscle. Posterior neck muscles Sternocleidomastoid Although these muscles do not directly affect mandibular movements, they can become symptomatic during certain TM disorders. Trapezius, splenius, capitis, semispinalis capitis. It is at this stage to evaluate any possible craniocervical disorders. The patient can be asked to rotate his head to the right and left and move it up and down. This is done to distinguish muscular from vertebral problems, and referring the patient to the right physician. Useful in case muscles are difficult to palpate. Relies on the fact that function will induce or increase pain in fatigued or traumatized muscles. Medial pterygoid, inferior and superior lateral pterygoids. Medial pterygoid is resnposible for closing the mouth. So pain will be elicited when the patient is asked to close his mouth or biting down on an object. Also, stretching of the muscle during opening the mouth would be painful. Pain would be elicited in the inferior lateral pterygoid if the patient is asked to protrude the mandible against resistance from the operator. Palpation Auscultation Extrameatal Intrameatal In the extrameatal joint examination the finger tips are placed on the lateral aspect of the TMJ on both sides simultaneously. And the patient is asked to open and close his mouth and if any pain was elicited it should be recorded using the same pain scale for the muscles. In the intrameatal joint examination the little finger of both hands is placed in the external auditory meatus, pushing slightly forward, pain should be evaluated in the static position, while opening and closing. The intrameatal examination aims to evaluate symptoms from the posterior and lateral aspects of the joints. Click Crepitation Sounds may be heard by the stethoscope or felt by placing the fingertips at the lateral aspect of the TMJs. It should be noted the severity of such sounds, unilateral or bilateral, on closing, opening or both. A click is a single sound of short duration, relatively loud, also referred to as a pop. Crepitation is a gravelike sound described as grating and complicated. Determination of maximum interincisal opening (53-58 mm) <40 mm Deviation ? Deflection ? Even a child can open to 40mm. The average mandibular opening measured interincisally is 53-58 mm. If the patient opens comfortably to a certain measurement and then opens more but with pain, both measurements should be recorded. The crude measurement of the opening is three fingers. Less than 40mm is restricted. Deviation in mandibular movement is a shift from the midline during opening that disappears with continued opening. Deflection is a shift from the midline that becomes greater when opening and does not disappear at maximum opening. Determination of lateral excursions (approximately 10mm) Movements of less than 8mmis considered restricted. Measure the distance moved from the midline. Determination of protrusion (5mm or >) Inspect the teeth and their supportive structures for any signs of breakdown. Common signs and symptoms: Tooth mobility Pulpitis Tooth wear It is important to distinguish functionally optimal occlusion and normal occlusion. Normal occlusion could be a deviation from ideal occlusion; however, it does not induce pathology. Centric occlusion (MIC)/centric relation discrepancies TMJ radiographs Used to gain additional insights especially when pathology is expected to rule out malignancy. Provide information regarding: Morphological characteristics of the bony components of the joint Certain functional relationships between the condyle and the fossa.