Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cardiac contractility modulation wikipedia , lookup
Electrocardiography wikipedia , lookup
Heart failure wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Coronary artery disease wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Cardiac surgery wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Jatene procedure wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
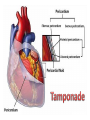
Anatomy and physiology of the cardiovascular system Dr Cath Spoors Consultant, Anaesthesia and Burns Intensive Care Broomfield Hospital, Chelmsford Cardiovascular system • Giant circular shuttle system • Transport – Oxygen, nutrients, cells – CO2, waste products • Distribution – The right stuff to the right place at the right time What price failure? What price failure? What price failure? What price failure? What price failure? 30% arteries 5% capillaries 65% veins Large arteries • Elastic arteries – large and proximal. Vessel wall distension in the presence of a competent aortic valve acts as a secondary pump • Muscular arteries – high-pressure conduits. Pressure waves within them are palpable as peripheral pulses. Arterioles • Control of local blood flow • Major determinant of systemic vascular resistance (SVR) and therefore blood pressure • Independent in any given organ bed (control distribution of cardiac output around the body) • Influence capillary hydrostatic pressure Control of blood flow • Myogenic – stretch causes vasoconstriction, slackening causes vasodilation. Important in brain and kidney Control of blood flow • Metabolic – substances produced by active tissues cause vasodilatation to “attract” more blood to the area (bradykinin, CO2). Hypoxia also causes vasodilatation • Sympathetic – basal arteriolar tone. α1 receptors – vasoconstriction (most beds esp skin, gut, kidneys). Β2 receptors – vasodilatation (skeletal muscle). Brain and heart less affected by neurogenic control • Hormonal – adrenaline on adrenoceptors Capillaries • Continuous – muscle, brain, connective tissue. Cells joined by tight junctions. Water, oxygen, carbon dioxide and small water-soluble molecules can pass relatively easily. Larger molecules must be transported across • Fenestrated – intestine, kidneys. Contain pores which allow rapid exchange of water and small molecules • Sinusoidal – liver, bone marrow – whole blood can pass out into the interstitium Capillaries • Gradients Capillaries • Gradients Capillaries • Gradients Veins and the venous reservoir • Low-pressure system for conducting blood back to heart • Valves to prevent stasis • Distend – can accommodate large volumes with little pressure change. “Buffer” for blood volume • Venous reservoirs in lungs, liver, gut and skin – under sympathetic control • Skeletal muscle augments return of venous blood to heart • Respiratory pump increases intrathoracic and right ventricular volume by sucking in blood from veins Cardiac output • The volume of blood pumped out of the left ventricle per unit time • Approx 3.5-7.5L/min in adults Cardiac output • The volume of blood pumped out of the left ventricle per unit time • Approx 3.5-7.5L/min in adults Cardiac output • The volume of blood pumped out of the left ventricle per unit time • Approx 3.5-7.5L/min in adults Venous return • The volume of blood returned to the right atrium per unit time Cardiac output • The volume of blood pumped out of the left ventricle per unit time • Approx 3.5-7.5L/min in adults Venous return • The volume of blood returned to the right atrium per unit time Determinants of stroke volume • Preload • Afterload • Contractility Determinants of heart rate • Autonomic function • Dysrhythmias • Pacemakers Preload • Myocardial muscle cells obey Starling’s law (force-length relationship) Preload • Myocardial muscle cells obey Starling’s law (force-length relationship) Preload • Myocardial muscle cells obey Starling’s law (force-length relationship) Determinants of preload • Volume status – Hypovolaemia reduces pre-load and cardiac efficiency – Hypervolaemia over-distends the right heart and reduces efficiency • PEEP – High PEEP (recruitment manoeuvres) can reduce venous return by increasing thoracic pressure which impedes flow into the heart • Arrhythmias – The chambers need time to fill; if the duration of diastole is reduced this will impede ventricular filling • Regurgitant cardiac valves • Cardiac tamponade Afterload • The force opposing shortening of muscle fibres during contraction • Increases in afterload will reduce the stroke volume • Increases with increased pressure in the chamber cavity • Increases with diameter of the chamber cavity • Decreases with wall thickness Afterload • Most afterload is provided by systemic vascular resistance • Arterial dilatation will reduce afterload but this may compromise coronary perfusion Afterload • Most afterload is provided by systemic vascular resistance • Arterial dilatation will reduce afterload but this may compromise coronary perfusion Contractility • This is the contractile energy of the heart not related to preload or afterload • Increased contractility will give an increased stroke volume • Increased by – Sympathetic stimulation (catecholamines) – Extracellular calcium levels – Increased heart rate (Bowditch effect) • Decreased by – – – – Ischaemia Drugs Sepsis Toxins Contractility • This is the contractile energy of the heart not related to preload or afterload • Increased contractility will give an increased stroke volume • Increased by – Sympathetic stimulation (catecholamines) – Extracellular calcium levels – Increased heart rate (Bowditch effect) • Decreased by – – – – Ischaemia Drugs Sepsis Toxins Determinants of heart rate • In sinus rhythm, the SA node determines the heart rate • Control is by reciprocal action of sympathetic and parasympathetic nerves • Circulating catecholamines also increase heart rate • β1 adrenoceptors in the SA node speed up; muscarinic (parasympathetic) slow down • Optimisation is the key to heart rate manipulations – trade off between cardiac work (oxygen demand), output, and venous return (filling)