Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
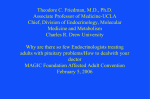
中華放射醫誌 Chin J Radiol 2004; 29: 171-176 171 Central Diabetes Insipidus in Patients Without Apparent Initial MR Imaging Findings: A 2-year Follow-up MR Imaging Study 1,2 M ING -S HIANG YANG C LAYTON C HI -C HANG C HEN C HUNG -M ING T SAI 2 S AN -K AN L EE 2 2 Y UNG -Y I C HENG 2 Y EU -S HENG T YAN 1 Y I -F EN WANG 3 Department of Radiology1, Chung- Shan Medical University Hospital Department of Radiology2, Taichung Veterans General Hospital 3 Department of Radiology , Taipei Veterans General Hospital The aim of this study is to describe the follow-up magnetic resonance imaging (MRI) findings in patients with central diabetes insipidus (CDI) patients and without having apparent initial imaging abnormality. This was a retrospective study. In the past 8 years (from 1995 to 2002), 26 patients (male 14, female 12, mean age 20.1 years) were diagnosed as CDI by water deprivation test, 1-desamino-8-D-arginine vasopressin (DDAVP) test, and the relationship between urine-plasma osmolarity. The major clinical manifestations are polyuria and polydipisia. We retrospectively analyzed the MR images. The subtle MR images included (1) loss of high signal intensity (SI) in posterior lobe on T1WI (26.9%, n=7), (2) an empty sella, (11.5%, n=3), (3) shallowing of the pituitary fossa (3.8%, n=1), (4) ectopic bright high signal intensity on T1WI at the hypothalamus (3.8%, n=1), (5) normal (23%, n=6), (6) thickened pituitary stalk thickness (PST) (26.9%, n=7). All these patients were followed at least 2 years with MR images. Seven patients were initially presented as increased pituitary stalk thickness (PST). In the following images, 5 of the seven patients had progressive thickened stalk and underwent the biopsy procedure. They were diagnosed as germinoma, histio- Reprint requests to: Dr. Yeu-Sheng Tyan Department of Radiology, Chung- Shan Medical University Hospital. No. 110, Sec. 1, Jian Guo N. Road, Taichung 402, Taiwan, R.O.C. cytosis, and sarcoidosis. Two cases of the PST group had static imaging findings in the follow-up images just as in other groups. In our limited experiences the causes of CDI were variable. It is most important to follow up the subtle MR findings. In group with progressive pituitary stalk thickness, we emphasize the necessities to make biopsy for definite diagnosis. Key words: Central diabetes insipidus, MR imaging; Diabetes insipidus; Germcell neoplasm; Histiocytosis; Sarcoidosis Central neurogenic diabetes insipidus (CDI) is a disorder, characterized by chronic polyuria and polydipsia, secondary to deficiency of arginine vasopressin. In many patients, especially the children and young adults, it is caused by the destruction and degeneration of neurons that originate in the supraoptic and paraventricular nuclei of the hypothalamus [1]. The causes of CDI include germinoma [2], craniopharyngioma [3], Langerhan’s cell histiocytosis (LCX), inflammation, autoimmune and vascular disease [4,5], trauma resulting from surgery or accident [6], and in rare occasions, the genetic defects in the synthesis of vasopressin, in which it is inherited as autosomal dominant or X-linked recessive traits. However, CDI are considered to be idiopathic [7] in 30 to 50% of the cases The most frequent MR findings in CDI patients include normal imaging appearance [8], thickened pituitary stalk [8], invisibility of the posterior lobe high signal intensity [8] (SI) on T1WI, focal suprasellar or hypothalamic mass lesions such as germinoma and craniopharyngioma, etc. Nevertheless, the long-term follow-up imaging studies of the subtle lesions had not been recognized very well. The purpose of the study is 172 The images of CDI mainly to focus on the subtle MR imaging findings and the follow-up imaging changes. MATERIAL AND METHODS In the past 8 years (from 1995 to 2002), 29 cases were diagnosed as CDI in our hospital. Three cases were excluded due to apparent causative gross tumor lesion on the initial images. The total case number is 26. The diagnosis of central diabetes insipidus was based on clinical history of polyuria and polydipsia, and the results of physical examination, laboratory evidence of arginine vasopressin deficiency and the imaging studies of the brain and pituitary gland. In cases without any identifiable causes and imaging findings, include the following images, were considered to be idiopathic. This was a retrospective study, including fourteen male and twelve female patients. The mean age at diagnosis was 20.1 year-old (ranged from 3 to 56 year-old). All of the patients had permanent central diabetes insipidus, and were treated with desmopressin acetate. The MRI pulse sequences included pre-contrast sagittal section T1-weighted imaging (T1WI), both axial and coronal section T2-weighted imaging (T2WI), post-Gadolinium DTPA coronal and sagittal T1WI images and dynamic study of pituitary gland. All of the pulse sequences were performed in either one of the two 1.5 Tesla MRI scanners (Horizon, L, GE Medical system, Milwaukee, USA and Sonata, Siemens AG, Erlangen, Germany). The parameter for pituitary gland in T1WI is TR = 400-650 ms, TE = 1220 ms, matrix = 256 × 256 and nex = 4. The parameter in T2WI is TR = 2000-3000 ms, TE = 70-100 ms, matrix = 320 × 256 and the nex = 4. The FOV is 16 × 16 cm in size. The slice thickness is 3 mm and the gap is 0.3 mm. The pituitary stalk thickness measured on the mid-sagittal section T1WI image [10]. The criteria of normal pituitary stalk is defined as 3 to 3.5 mm wide near the median eminence and 2 mm wide near its insertion on the pituitary gland [10]. All MR images were reviewed by two neuroradiologists. All patients were followed at least two years and at least five years in PST group. The imaging follow-up schedule is about 3 to 6 months interval. RESULTS The characteristic MRI findings and clinical data of the 26 patients are listed in the Table 1 and Table 2. In the thickened pituitary stalk group, about 71.4% (5/7) of cases showed progressive thickening on the Table 1. Patient list of general data and images findings. Case No. Age Sex Image findings 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 8 25 7 40 7 51 7 19 45 12 56 5 11 16 7 34 10 20 44 3 8 19 34 10 15 11 F M M F M M F F M F M M M M F F F F F M M M F M M F empty sella normal shallowing of pituitary fossa PLBSD PST and PLBSD PLBSD PLBSD PST and PLBSD partial empty sella and PLBSD normal normal (post-operative sequale) other PST ectopic neurohypophysis normal (post-operative sequale) empty sella PST PLBSD PST normal PST normal (post-operative sequale) pituitary stalk transection PST other other PST: pituitary stalk thickness PLBSD: posterior lobe bright signal disappearance on T1WI Note 1: case 13 and case 17 progressed to germinoma Note 2: case 21 and case 23 progressed to histiocytosis. case 19 progressed to sarcoidosis Note 3: case 12 is Menkes disease. Case 25 and 26 are Wolfram syndrome. following images (Fig 1). These five patients all had received the biopsy procedures. Two of them had germinoma, two had histiocytosis and one had sarcoidosis. Another two patients in this group did not reveal any significant change in at least 5 years period. The loss of brightness of posterior lobe in the T1WI group (n = 7), in the ectopic posterior lobe of pituitary gland (n = 1), in the initial normal imaging finding group (n = 6), and in the empty sella group (n = 3) did not reveal any significant change in the following imaging for at least two years. In the initial normal MR imaging group, three of the six cases were complicated by previous surgery at the suprasellar area, such as craniopharyngioma or meningioma, operation etc. The initial and following images of the pituitary gland were almost normal. Other rare causes of CDI also presented in this study, such as pituitary stalk transection (n = 1) (Fig 2), Menke’s disease (n = 1). The ectopic short T1 tissue over median eminence with contrast enhancing pattern in pituitary transection case could be defined. In general, it was believed to be the ectopic neurohypophysis tissue. And it was only categorized into the The images of CDI 1a 173 1b Figure 1. Histiocytosis: T1WI sagittal section, a. (650/20/4/256x256), b. (450/10/4/256 × 256), c. T1WI (450/20/2/256 × 224) Progressive enlargement of the pituitary stalk is noted in the serial following images (A, B, arrows). Multiple levels of vertebra plana over T-, L-spine vertebral bodies were also seen (C, arrows). Patient received the biopsy procedure, confirming the diagnosis of histiocytosis. 1c pituitary transection group in the retrospective study. In this study, 2 cases were diagnosed as Wolfram syndrome. They are sibling from a diabetic family. Their images revealed diffuse central nervous system degenerative process (Fig 3) with clinical manifestations of diabetes insipidus and diabetes mellitus. DISCUSSION Figure 2. Pituitary transection: Sagittal section T1WI (450/12/4/256 × 256) A disruption of pituitary stalk (long arrow) is identified in this patient. Contrast enhancing foci was seen over median eminence (short arrow). It is thought to be ectopic neurohypophysis. In many normal subjects, the posterior pituitary showed high signal intensity on the sagittal T1weighted magnetic resonance image (MRI). The absence of this image finding serves as a nonspecific indicator of central diabetes insipidus, because of the frequency of hyperintensity decreased with aging in normal subjects [8]. The posterior pituitary bright signals on T1WI, initially thought to be due to fat within the sellar turcica, was attributed to the arginine vasopressin (AVP) content in the neurosecretory granules or intracellular lipid droplets in the glial cell 174 The images of CDI pituicytes of the posterior lobe. This signal, reported in 90-100% of normal subjects, appears to be closely related to the normal hypothalamic-neurohypophyseal axis function [8]. Many patients with central diabetes insipidus (CDI) did not have posterior pituitary hyperintensity on T1WI images, indicating that the absence of hyperintensity, although nonspecific, is a cardinal feature of CDI. The absence of posterior bright signal was the most common finding in our study. The size of normal pituitary stalk is 3 to 3.5 mm in width near the median eminence and 2 mm near its insertion on the pituitary gland [10]. Thickening of either the entire pituitary stalk or just the proximal portion was another common abnormality on MRI scans. It is quite helpful in differential diagnosis of idiopathic diabetes insipidus from those associated with germinomas or Langerhan’s-cell histiocytosis, but it was not specific for any subtype. Other studies have reported the thickened pituitary stalk in association with autoimmune or inflammatory disease recognized as “lymphocytic infundibuloneurohypophysitis” [10], “lymphocytic hypophysitis” [11], or “necrotizing infundibulohypophysitis” [12]. The follow-up MRI scans of central diabetes insipidus patients with a thickened pituitary stalk showed a variable range of changes, from a spontaneous resolution of the abnormality to further enlargement, or without significant change [1]. In the PST group (n = 7), five patients showed progressive thickening of the stalk and underwent biopsy. Two cases of thickened pituitary stalk were found to have germinoma, two with histiocytosis, and the other one with sarcoidosis. The incidence of progressive change in the PST group was 71.4% (5/7). Due to the high incidence of progressive change of pituitary stalk thickness, the follow-up images and even biopsy are essential for these patients. Other than the PST group, the following images did not reveal significant change for at least two years. The MR evidence of progressive reduction in the size of the pituitary gland was usually associated with a higher risk of an additional endocrine defect. The decrease in size may be a consequence of vascular damage or a deficiency of hypothalamic hormones [13-14]. In the study, no evidence of progressive reduction of the stalk size was shown. Some patients, who suffered from CDI, were due to the complication of operation at the pituitary region or suprasellar area. In the normal imaging group (n = 6), three of them suffered from CDI were complicated by previous surgery. The causes might be due to local vascular injury or direct pituitary gland injury. Table 2. Summary of images findings in CDI Findings Normal Increased PST*** Loss bright SI of post.lobe (T1WI) Empty sella Shallowing of pituitary fossa Ectopic posterior lobe Pituitary stalk transection1 Other Case No. (%) 6 (23%) 7 (26.9%) 7 (26.9%) 3 (11.5%) 1 (3.8%) 1 (3.8%) (3.8%) 3 (11.5%) M/F (4/2) (4/3) (3/4) (0/3) (1/0) (1/0) (0/1) (1/0) PST: pituitary stalk thickness SI: signal intensity *** 2 cases progressed to histiocytosis, 2 cases progressed to germinoma, 2 cases were stationary, and 1 case progressed to sarcoidosis. Other: Menke’s disease and Wolfram syndrome Note 1: Two cases have both the PST and loss bright SI of post.lobe on T1WI. Note 2: One case have both the partial empty sella and loss bright SI of post.lobe on T1WI. Figure 3. Sagittal section T1WI (450/12.5/4/256 × 256): The eleven years old girl disclosed pineal cyst and absence of shorter T1 effect of posterior pituitary lobe (short white arrow). Brain stem atrophy (long white arrow) was noted, in addition to mid-brain and pons. Marked neurodegnerative process was also noted. However, the initial and follow-up images of pituitary gland were normal. Other rare causes of CDI are Menkes’s disease and pituitary stalk transection. Disruption of the pituitary stalk was seen in the images of a case of pituitary transection. The ectopic short T1 lesion over median eminence with contrast enhancement could be seen in the patient with stalk transection. It was thought to be ectopic neurohypophysis. One patient suffered from CDI had shallow pituitary fossa on the MR images. The shallow pituitary fossa may impair the normal function due to too small space for pituitary gland. Local hemodynamic change or other vascular abnormality on the pituitary gland may result in CDI clinical appearance. The images of CDI However the real relationship is still not clear. Two patients with Wolfram syndrome were identified in the study. They are sibling. They came from a diabetes family and suffered from CDI and DM. Both poor visual acuity and hearing impairment were also noted. MRI revealed marked atrophic change of brain stem and cerebellum. Both cases could not demonstrate the short T1 effect of posterior pituitary gland. But they were not categorized into the PLBSD (posterior lobe bright signal disappearance) group due to the rare disease and more complicated image appearance. CONCLUSION In the variable causes of CDI, MRI plays an important role. With subtle MR findings in CDI patients, follow-up images is most important of all especially in the thickened pituitary stalk group. High percentage of progressive change is clearly shown in this group as compared to other images group. The progressive increase in the size of the pituitary gland should alert the physicians to the possibility of tumor growth such as germinoma or histiocytosis. On the other hand, a decrease in size can suggest the presence of an inflammatory or autoimmune process. Biopsy should be employed for the patients with progressive thickening of the pituitary stalk, since spontaneous recovery may occur in patients with this feature. In patients with CDI and normal MRI or questionable increased PST, a regular follow-up at 3-month interval is highly recommended since normal MRI does not exclude the possibility of tumor. ◆ REFERENCES 1. Maghine M, Cosi G, Genovese E, et al: Central diabetes insipidus in children and young adult. N Engl J Med 2000; 343: 998-1007 2. Mootha SL, Barkovich AJ, Grumbach MM, et al: Idiopathic hypothalamic diabetes insipidus, pituitary stalk thickening, and the occult intracranial germinoma in children and adolescents. J Clin Endocrinol Metab 1997; 82: 1362-1367 3. Maghie M, Villa A, Arico’ M, et al: Correlation between magnetic resonance imaging of posterior pituitary and neurohypophyseal function in children with diabetes insipidus. J Clin Endocrinol Metab 1992; 74: 795-800 4. Imura H, Nako K, Shimatsu A, et al: Lymphocytic infundibuloneurohypophysitis as a cause of central diabetes insipidus. N Engl J Med 1993; 329: 683-689 5. Maghnie M, Genovese E, Sommaruga MG: Evolution of children central diabetes insipidus into panhypopituitarism with a large hypothalamic mass: is “lymphocytic 175 infundibuloneurohypophysitis” in children a different entity. Eur J Endocrinol 1998; 139: 635-640 6. Verbalis JG, Robinson AG, Moses AM: Postoperative and post-traumatic diabetes insipidus. Front Horm Res 1985; 13: 247-265 7. Blotner H: Primary or idiopathic diabetes insipidus: a system disease. Metabolism 1958; 7: 191-200 8. Tien R, Kucharczyk J, Kucharczyk W: MR imaging of the brain in patients with diabetes insipidus. AJNR Am J Neuroradiol 1991; 12: 533-542 9. Brooks BS, el Gammal T, Allison JD, et al: Frequency and variation of the posterior pituitary bright signal on MR images. AJNR Am J Neuroradiol 1989; 153: 10331038 10. Simmons GE, Suchnicki JE, Rak KM, et al: MR imaging of the pituitary stalk: size, shape, and enhancement pattern. AJR 1992; 159: 375-377 11. Sheen KC, Chang CC, Chang TC, Liu HM: Thickened pituitary stalk with central diabetes insipidus: report of three cases. J Formos Med Assoc. 2001 May; 100: 198204 12. Thodou E, Asa SL, Kontogeorgos G, et al: Lymphocytic hypophysitis: clinicopatholiogical findings. J Clin Endocrinol Metab 1995; 80: 2302-2311 13. Ahmed SR, Aiello DP, Page R, et al: Necrotizing infundibulo-hypophysitis: a unique syndrome of diabetes insipidus and hypopituitarism. J Clin Endocrinol Metab 1993; 76: 1499-1504 14. Roberston GL: Diabetes insipidus. Endocrinol Metab Clin North Am 1995; 24: 549-572 15. Maghnie M, Genoveses E, Arico’ M, et al: Evolving pituitary hormone deficiency is associated with pituitary vasculopathy: dynamic study in children with hypopituitarism, diabetes insipidus, and Langerhan cell histiocytosis. Radiology 1994; 193: 493-499 176 The images of CDI 中央性尿崩症不明顯的初步核磁共振影像表現: 兩年的核磁共振影像追蹤經驗 楊明祥 1,2 陳啟昌 2 鄭永宜 2 中山醫學大學附設醫院 放射線部 台中榮民總醫院 放射線部 2 3 台北榮民總醫院 放射線部 田雨生 1 王憶芬 3 蔡仲明 2 李三剛 2 1 本研究的主要目的是介紹及討論,中央性尿崩症患者不明顯的核磁共振影像表現以及追蹤 影像的變化。 本研究是壹回溯性的研究。在最近 8 年,共搜集 26 位病例,其中男性 14 位,女性 12 位, 平均年齡 20.1 歲。診斷主要是依據 DDAVP 試驗以及血液-尿液之間滲透壓的關係。主要的症狀 為多尿,多渴。本研究是回溯性的分析核磁共振影像表現。 26 位病例中,有 7 位(26.9%)腦下垂體後葉的高訊號消失,有 3 位(11.5%)為空白蝶 鞍,有 1 位(3.8%)腦下垂體窩變淺,有 1 位(3.8%)為異位性腦下垂體後葉.有 6 位(23%) 是正常的核磁共振影像表現.有 7 位(26.9%)是腦下垂體蒂肥厚。 在腦下垂體蒂肥厚組的病人中,其中有 5 位持續變厚並接受手術組織檢體檢查,分別被診 斷為生殖細胞瘤,組織細胞症及類肉瘤病。其中有 2 位與其他它組的病人一樣,追蹤的核磁共 振影像持續不變。 在有限的經驗中,中央性尿崩症的原因相當多,在不明顯的核磁共振影像表現的病人中, 持續追蹤是最重要的。特別在腦下垂體蒂持續變厚的病人,組織檢體檢查尤其重要。 關鍵詞:磁振造像,尿崩症,生殖細胞瘤,組織細胞症,類肉瘤病