Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
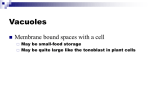
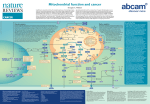
Hallmarks of Cancer Stem Cell Metabolism Patricia Sancho*, David Barneda and Christopher Heeschen* Centre for Stem Cells in Cancer & Ageing, Barts Cancer Institute, Queen Mary University of London, UK, EC1M 6BQ * Correspondence: Dr. Patricia Sancho, PhD, [email protected] or Dr. Christopher Heeschen, MD, PhD, [email protected]; Centre for Stem Cells in Cancer & Ageing, Barts Cancer Institute, Queen Mary University of London, UK. Keywords: Cancer stem cells, Tumour-initiating cells, Oxidative phosphorylation, Glycolysis, Metastasis, Metformin, Myc. Acknowledgements: This work was supported by the ERC Advanced Investigator Grant (Pa-CSC 233460 to C.H.), the European Community's Seventh Framework Programme (FP7/2007-2013) under grant agreement n° 256974 (EPC-TM-NET to C.H.) and n° 602783 (CAM-PaC to C.H.), the 2015 SU2C Lustgarten CRUK Pancreatic Cancer Dream Team Award (to C.H.) and the Pancreatic Cancer Research Fund (to P.S.). ABSTRACT To cope with their high proliferation rate, cancer cells adapt their cellular metabolism using glycolysis instead of from oxidative phosphorylation (OXPHOS) for production of ATP and building blocks (Warburg effect). However, not all cancer cells behave equally due to substantial (epi-)genetic heterogeneity. Despite having an identical genetic background, a subset of cells bears stemness features, thus termed cancer stem cells (CSCs), resulting in a hierarchical organisation of the tumour reminiscent of normal tissues. As opposed to differentiated cancer cells representing the bulk of the tumour, CSCs in various, but not all human cancer types preferentially rely on mitochondrial OXPHOS, thus rendering CSCs less dependent on the sparse supply with nutrients in the tumour microenvironment. Moreover, the metabolic plasticity as the ability to switch between OXPHOS and glycolysis depending on circumstances, is also limited in CSCs of various cancers. This apparent fixation of CSCs on mitochondrial function for energy supply, but also for maintenance of their stemness properties represents a previously unrecognised Achilles heel amendable for therapeutic intervention. Elimination of highly chemoresistant CSCs as the root of many cancers via inhibition of mitochondrial function may prevent relapse from disease and thus improve patients’ long-term outcome. I. INTRODUCTION Cellular Metabolism In non-transformed, mostly slowly proliferating or even quiescent somatic cells, mitochondria are the main source of energy production through the tricarboxylic acid (TCA) cycle coupled to oxidative phosphorylation (OXPHOS), which takes place in the mitochondrial matrix. Several carbon fuels such as pyruvate, glutamine and fatty acids can feed the cycle to produce reducing equivalents (nicotinamide adenine dinucleotide phosphate, NADH; Flavin adenine dinucleotide, FADH2) that are subsequently used as electron donors for the electron transport chain (ETC). The transport of electrons across the different complexes of the ETC is coupled to the generation of a proton motive force, used by the ATP synthase (complex V) to generate ATP1. Cancer cells, however, are characterised by a high proliferation rate and thus need to adapt their cellular metabolism in order to provide support for increased division rates: rapid ATP generation to maintain energy status, increased biosynthesis of macromolecules and tight regulation of the cellular redox status2. Moreover, tumour cells must evade the checkpoint controls that under physiological conditions inhibit proliferation in challenging metabolic conditions as found in the tumour microenvironment. Levels of glucose, glutamine and oxygen are spatially and temporally heterogeneous and frequently sparser as compared to conditions in well-perfused organs. Accordingly, tumour cells reprogram their metabolic pathways to meet their needs during the process of tumour growth, but also during metastasis. For this purpose, cancer cells shift from ATP generation via OXPHOS to ATP generation via glycolysis, despite still sufficient oxygen concentrations in the tumour microenvironment (Warburg effect). As a result, many transformed cells derive a substantial amount of their energy via aerobic glycolysis, which is more rapid than OXPHOS, but also far less efficient in terms of ATP generated per unit of glucose consumed, resulting in an abnormally high rate of glucose uptake. Under these circumstances, glucose is also metabolised through the pentose phosphate pathway (PPP) and other alternative pathways2, which produce large quantities of reduced NADPH and other macromolecules to generate the necessary building blocks required for sustaining high rates of cellular division. Cancer Stem Cells It is important to note that not all cancer cells behave equally, both at the functional and metabolic level. Convincing evidence demonstrated that substantial (epi-)genetic heterogeneity exists within each individual tumour. First, multiple subclonal populations of cancer cells are assumed to foster tumour adaptation and therapeutic failure through Darwinian selection. Secondly, cancer heterogeneity also exists within each of these subclones, despite their identical genetic background, via the acquisition of stemness features in a subset of cells, thus resulting in a hierarchical organisation of the tumour that is vaguely reminiscent of that found in many normal tissues (Fig. 1)3. At the apex of this hierarchy are populations of cancer stem cells (CSCs) capable of self-renewal, bearing long-term in vivo tumourigenicity as well as generating more differentiated progenies constituting epigenetically defined intraclonal bulk4. This new view of intraclonal functional heterogeneity bears the potential to fundamentally change the way we analyse and treat cancer. This will require a thorough understanding of the mechanisms underlying this close relationship between stem cells and their malignant counterparts as well as their metabolic features. Although CSCs do not necessarily arise from tissue stem cells, these cells have acquired stemness features allowing them to indefinitely self-renew and give rise to their respective differentiated progenies. Epigenetic regulation mimicking, at least in part, normal differentiation contributes to the generation of these hierarchically organised clones that, although sharing common mutation profiles, bear diverse gene expression patterns and functions5. Accumulating evidence also suggests striking parallels between mechanisms orchestrating normal embryogenesis and those that invoke tumourigenesis and CSCs in particular6. Thus, it is of utmost importance to conclusively define the potentially distinct metabolic features of CSCs. II. METABOLIC PHENOTYPE OF CANCER STEM CELLS Originally, it was hypothesised that CSCs bear a metabolic phenotype in analogy to normal tissue hierarchy where multipotent stem cells are fundamentally glycolytic, while differentiated somatic cells rely on OXPHOS7. Similar patterns have been reported for induced pluripotent stem cells (iPSCs), where the reprogramming process is associated with a switch from OXPHOS to a glycolytic programme, which indeed is essential for effective acquisition of a pluripotent state. These findings suggested that not only are metabolic phenotype and stemness intrinsically linked, but rather cellular metabolism actually controls stemness properties. Thus, it was postulated that activation of the glycolytic programme favours stemness via different mechanism including enhanced antioxidant capacity via the PPP as the most relevant one8. Subsequently, a number of investigations aimed to validate this concept of glycolysis-driven stemness to the cancer field. Experimental evidence obtained for CSCs in breast cancer seemed to support such hypothesis. For example, Dong et al. demonstrated that the metabolic switch from OXPHOS to aerobic glycolysis was essential for maintaining CSC functionality, due to decreased ROS levels 9. Moreover, glycolysis was also found to represent the favoured metabolic programme of CSCs in nasopharyngeal carcinoma10 and hepatocellular carcinoma11. Interestingly, elevated expression of the oncogene MYC was defined as the main driver of stemness for these three cancer types12, which is well in line with findings for iPS cells as discussed above. While the MYC levels did not determine the metabolic wiring of iPS cells, their tumorigenic potential as evidenced by teratoma formation was intrinsically linked to a MYC-driven glycolytic program13. Therefore, MYC seems to be a likely candidate determining the connection between glycolysis and stemness, intimately associated to the tumorigenic potential of iPS cells, but also for certain cancer types as listed above. Importantly, however, accumulating evidence now demonstrates that CSCs in other cancer types may actually rely on mitochondrial OXPHOS as the preferred energy production. To date, this has been shown convincingly for glioblastoma14, lung cancer15, pancreatic cancer16 and leukaemia17. Interestingly, metabolic rewiring to OXPHOS rendered CSCs derived from these tumours resistant to inhibition of glycolysis, which may confer these cells with a higher degree of independency from microenviromental nutrient supply, as discussed in more detail below. Although the mechanisms of action for the observed OXPHOS phenotype have not been well characterised for all cited tumour types, regulatory proteins of mitochondrial biogenesis and structure seem to play a crucial role in maintaining stem-related properties and functionality14, 16 . Indeed, findings for pancreatic cancer clearly demonstrate that expression of the transcription factor PPARGC1A (PGC-1α), a master regulator of mitochondrial biogenesis, was essential for the OXPHOS functionality in pancreatic CSCs and, most importantly, self-renewal and maximal in vivo tumorigenic capacity16. Intriguingly, a MYC-driven glycolytic programme was only found in more differentiated tumour cells and overexpression of MYC actually counteracted stemness via negatively controlling PGC-1α expression. These data seem to challenge the concept for MYC favouring stemness via activation of glycolysis, as demonstrated for iPSCs and some other cancer types. However, those apparently contradictory findings may be reconciled by a concept where MYC serves as a general modulator of the differentiation state, promoting either stemness or differentiation in a context and cell typedependent manner. Still, the apparent inconsistency in the predominant metabolic phenotype of CSCs isolated from various cancer types may actually, at least in part, be related to the utilised model systems. Most early studies in breast cancer demonstrating a highly glycolytic phenotype for the contained putative CSCs were performed in established for cell lines, for which the existence of a true CSC subpopulation remains at least questionable. Moreover, contradictory results regarding the CSC metabolic phenotype for individual cancer types can be found, e.g. for ovarian cancer, where CSCs have been reported to be either primarily glycolytic18 and OXPHOS-dependent19. The latter was reported for primary cultures, which were derived from tumours obtained either directly from patients or following in vivo expansion in immunocompromised mice (PDX models); an approach also used for studies in glioblastoma14 and pancreatic cancer16. Thus, it remains to be determined if the glycolytic phenotype originally reported for some cancer types will eventually be validated in clinically more relevant models. This matter is further complicated by recent reports that the metabolic plasticity, the ability to switch between OXPHOS and glycolysis depending on circumstances, also appears to vary considerably between CSCs derived from different tumour types. For example, while ovarian CSCs are characterised by marked metabolic flexibility rendering them highly resistant to metabolic targeting18, limited metabolic plasticity of CSCs has been reported for other tumour entities 14, 16. Again, it appears that a more restricted metabolic phenotype was mainly found in primary cultures or cell isolated from freshly resected tumours, where CSCs were shown to mostly rely on OXPHOS. However, irrespective of the underlying primary metabolic phenotype, limited metabolic plasticity represents an important feature with significant implications for designing new metabolism-centred therapeutic strategies. Specifically, a strict dependency on mitochondrial OXPHOS with low plasticity should render CSCs highly vulnerable to mitochondrial targeting, thus eliminating the source of relapse and metastasis. Addiction to oxidative mitochondrial metabolism could also be considered an adaptation of CSCs to their respective microenvironment. Indeed, OXPHOS equips CSCs with increased resistance to nutrient deprivation and, in general, to the metabolic austerity characterising many solid tumours. Although OXPHOS operates at a significantly lower rate, it constitutes a far more efficient source for energy generation. Thus, CSCs may generate a selective advantage in the context of specific tumour microenvironments, as they use more efficiently limited nutrients. In addition, lactate excreted by the more differentiated cancer cells running on glycolysis may serve as fuel for oxidative respiration in cellular subsets dependent on mitochondrial metabolism, such as CSCs, constituting a metabolic symbiosis system20. In line with this hypothesis, it has been demonstrated that certain glycolysis endproducts such as high-energy lactanes and ketones promote expression of stemness-associated genes and shifting cells towards OXPHOS21. In addition to constituting a major source of ATP for cancer cells, mitochondria participate in controlling multiple signalling pathways, including the release of Cytochrome C to initiate apoptosis, the release of bioactive ROS and the production of metabolites such as acetyl-CoA regulating protein acetylation1. As such mitochondria also appear to regulate stemness properties, irrespective of the underlying metabolic phenotype in individual cells 16, 22, 23. Indeed, enhanced mitochondrial biogenesis appears to represent a key factor for CSC functionality in both glycolytic and OXPHOS-dependent CSC14, 16. Increased mitochondrial mass, a surrogate marker for elevated biogenesis, can be easily tracked and may identify cells with increased self-renewal capacity and chemoresistance16 independently of the cancer type. Specifically, the use of this metabolic biomarker allowed to identify a subpopulation of CSCs with low mitochondrial mass but increased metabolic plasticity driven by MYC within the pancreatic CSC compartment (CD133+/Mitolow)16. Consequently, these cells showed increased resistance to mitochondrial targeting with respective inhibitors. However, this metabolic plasticity came at the expense of a reduced self-renewal capacity and in vivo tumorigenic potential, suggesting a delicate balance between stemness and metabolic plasticity, thus adding another level of complexity to the metabolic features of CSCs. Whether the state of these two different CSC subpopulations with differential plasticity and tumorigenic potential is dynamic and cells are able to transition between states, or is hard wired due to distinct genetic backgrounds remains to be elucidated. III. TARGETING CELLULAR METABOLISM The apparent OXPHOS dependence of CSCs in various tumours and the recently identified role of mitochondria in the regulation of stemness properties22, suggest that targeting mitochondrial metabolism could be an effective pharmacological strategy for the elimination of CSCs. Moreover, as mitochondria in cancer cells are often altered by mutations in their vulnerable DNA, the pharmacological disruption of certain mitochondrial processes could damage CSCs without affecting healthy tissues relying on OXPHOS. Pharmacological agents targeting OXPHOS at various levels are currently explored in preclinical and clinical studies for cancer treatment (Fig. 2) Targeting mitochondrial OXPHOS could be an effective strategy to eliminate cancer cells which cannot fully meet their energetic demands by glycolysis, either due to limited availability of glucose in poorly vascularised tumours, glycolysis inhibition by current therapies such as PI3K inhibitors, or restricted metabolic plasticity as observed in CSCs14, 16. Inhibition of mitochondrial respiration by agents blocking electron transport chain (ETC) complexes selectively induces apoptosis in CSCs versus non-CSCs16. The fact that such agents are also effective in eliminating primarily glycolytic CSCs in breast cancer or nasopharyngeal carcinoma24, 25 , highlights the importance of mitochondria for CSCs beyond energy production. In fact, tumour cells displaying mutations impairing TCA cycle or ETC, thus predominantly relying on glycolysis for ATP production, still require active mitochondria for the generation of metabolites from glutamine via reductive carboxylation26. Drug screens aiming for the identification of compounds that selectively eliminate CSCs resulted in the selection of several FDA-approved compounds that inhibit mitochondrial activity. For example, the antibiotic salinomycin, which inhibits OXPHOS, was identified in a screen targeting breast CSCs and eliminated the CSC gene expression signature in subsequent in vivo studies27. Remarkably, salinomycin was also selected in an independent screen aimed at targeting colorectal cancer cells in glucose-deprived multicellular tumour spheroids with inner hypoxia28, which could reflect the microenvironment of CSCs in solid tumours. Beside salinomycin, four other compounds were identified (nitazoxanide, niclosamide, closantel and pyrvinium pamoate), all of them inhibiting mitochondrial respiration. Niclosamide, an anti-helmitic drug which uncouples mitochondrial OXPHOS, was also among the selected compound in two independent drug screens in breast and ovarian CSCs29, 30. Apart from the direct inhibition of mitochondrial complexes, OXPHOS can also be suppressed by inhibitors of mitochondrial translation, e.g. the antibiotic tigecycline, which was selected in a drug screen because of its selective toxicity against leukemic cells, which depend on OXPHOS for energy production31. As mitochondria originally evolved from bacteria, it is not surprising that multiple antibiotics can disrupt mitochondrial function. Indeed, a recent study suggested that CSCs from multiple tumour types could be eradicated by treatment with certain widely prescribed antibiotics via disrupting mitochondrial respiration, either by inhibition of mitochondrial ribosomes or direct targeting of OXPHOS23. The anti-diabetic agent metformin has also emerged as a promising candidate for targeting OXPHOS in CSCs16. Interest in metformin rose when it was shown in retrospective studies that it is associated with a lower incidence of cancer in diabetic patients and improved survival when cancer has been diagnosed, respectively. Although the regulation of glucose and insulin levels may also contribute to the reported effects, compelling evidence demonstrated that the anti-tumoural activity of metformin involved the impairment of OXPHOS via direct inhibition of mitochondrial Complex I32. Remarkably, metformin selectively induced apoptosis in pancreatic CSCs as a result of their inability to switch to glycolysis and subsequent energy crisis16. Still, a minor subset of CSCs displaying low mitochondrial mass and a predominantly glycolytic metabolism were inherently resistant to metformin. The presence of these cells in pancreatic tumours appeared to account for the observed univocal relapse of tumours in mice treated with metformin and, among other factors including insufficient dosing in many patients, may also explain the negative outcome of the first clinical trials testing the effects of metformin in pancreatic cancer patients33. These data suggest that metformin and other drugs impairing mitochondrial ATP production need to be combined with agents targeting the mechanism of resistance allowing some CSCs to overcome OXPHOS inhibition, e.g. modulation of the PGC1-/MYC ratio. Intriguingly, metformin resistance in pancreatic CSCs was prevented/reversed by knockdown of MYC expression using RNAi or indirectly via BRD4 inhibition, suggesting the therapeutic potential of MYC inhibitors in combination with mitochondrial targeting. Alternatively, agents interfering with mitochondrial function at various levels may be more effective in targeting all CSCs. In fact, while drug resistance was observed with other OXPHOS inhibitors, such as rotenone or resveratrol, resistance was not seen for menadione, which acts via dual mechanism – inhibition of Complex I and induction of mitochondrial ROS. On the other hand, the efficacy of metformin may also be limited by its requirement of organic cation transporters (OCTs) for cellular uptake, which restricts its effects in healthy tissues, but also limits its potential use to tumour cells expressing OCTs. Phenformin, another biguadine formerly used in diabetes, could overcome these limitations as it is more hydrophobic and can be delivered to mitochondria more efficiently than metformin. Phenformin also promotes cancer cell death by inhibiting Complex I and has offered promising preclinical results in certain cancers such as non-small-cell lung carcinoma34. Thus, an important factor concerning the design of novel pharmacological strategies targeting mitochondria is to ensure the efficient delivery of the drug to the mitochondria of cancer cells. CSCs relying on OXPHOS will present an elevated Mitochondrial Membrane Potential (Δψm), which can be exploited for selectively increasing drug delivery to the mitochondria of these cells. Delocalised lipophilic cations (DLCs) such as triphenylphosphonium (TPP) accumulate in the mitochondrial matrix and can be conjugated to small compounds for selective drug delivery to mitochondria35. The mitochondrial accumulation of Mito-Chromanol, a vitamin E analogue conjugated to TPP induced cell death by inhibiting OXPHOS in breast cancer cells without affecting non-tumour cells36. Conjugation with TPP has also been utilised to selectively deliver the chaperone inhibitor Gamitrinib to active mitochondria and disrupt energy production in tumour cells by impairing protein folding in mitochondria37. However, mitochondria-penetrating peptides might be preferred for the treatment of certain tumours, as they can deliver cargo molecules irrespective of Δψm. Their conjugation to chemotherapeutic agents such as doxorubicin directs their activity towards mtDNA, promoting drug selectivity for cancer cells with reduced mtDNA integrity while their stable mitochondrial localisation prevents the acquisition of resistance by drug efflux38. IV. CONCLUSIONS In various cancers, CSCs have now been shown to bear a distinct metabolic phenotype and are highly dependent on OXPHOS with very limited metabolic plasticity. The reason for this may be multifactorial – beside gaining a greater independency from the sparse nutritional support in the tumour microenvironment, increasing evidence now also suggests that the tight control of mitochondrial ROS production in CSCs is a prerequisite for mainlining their stemness and high fidelity. This apparent metabolic vulnerability provides a vast set of new therapeutic opportunities to more efficiently eliminate these highly tumourigenic cells, even though resistance may arise in some instances. The latter could be related either to the acquisition of metabolic plasticity in a subset of CSCs or to the pre-existence of a small subset of CSCs with advanced metabolic features. As such CSCs display reduced stemness properties, they do not significantly participate in cancer progression in treatment naïve tumours, but metabolic targeting provides these cells with an advantage and they eventually take and drive relapse of the disease. Importantly, these resistant CSCs can be tracked by using tissue biopsies or by analysing circulating CSCs (liquid biopsies; Fig. 1) in order to monitor treatment response as well as arising resistance. A more effective strategy could be to combine distinct targeting strategies or to use mitochondria-targeting agents with dual mechanism of action, which may help to improve the still miserable outcome of many cancer patients. REFERENCES 1. Chandel NS. Mitochondria as signaling organelles. BMC Biol 2014;12:34. 2. Vander Heiden MG, Cantley LC, Thompson CB. Understanding the Warburg effect: the metabolic requirements of cell proliferation. Science 2009;324:1029-33. Garcia-Silva S, Frias-Aldeguer J, Heeschen C. Stem cells & pancreatic cancer. Pancreatology 2013;13:110-3. 3. 4. Hermann PC, Huber SL, Herrler T, et al. Distinct populations of cancer stem cells determine tumor growth and metastatic activity in human pancreatic cancer. Cell Stem Cell 2007;1:31323. 5. Visvader JE, Lindeman GJ. Cancer stem cells: current status and evolving complexities. Cell Stem Cell 2012;10:717-28. 6. Lonardo E, Hermann PC, Mueller MT, et al. Nodal/Activin signaling drives self-renewal and tumorigenicity of pancreatic cancer stem cells and provides a target for combined drug therapy. Cell Stem Cell 2011;9:433-46. 7. Folmes CD, Dzeja PP, Nelson TJ, et al. Metabolic plasticity in stem cell homeostasis and differentiation. Cell Stem Cell 2012;11:596-606. 8. Perales-Clemente E, Folmes CD, Terzic A. Metabolic regulation of redox status in stem cells. Antioxid Redox Signal 2014;21:1648-59. 9. Dong C, Yuan T, Wu Y, et al. Loss of FBP1 by Snail-mediated repression provides metabolic advantages in basal-like breast cancer. Cancer Cell 2013;23:316-31. 10. Shen YA, Wang CY, Hsieh YT, et al. Metabolic reprogramming orchestrates cancer stem cell properties in nasopharyngeal carcinoma. Cell Cycle 2015;14:86-98. Chen CL, Uthaya Kumar DB, Punj V, et al. NANOG Metabolically Reprograms TumorInitiating Stem-like Cells through Tumorigenic Changes in Oxidative Phosphorylation and Fatty Acid Metabolism. Cell Metab 2015. 11. 12. Gabay M, Li Y, Felsher DW. MYC activation is a hallmark of cancer initiation and maintenance. Cold Spring Harb Perspect Med 2014;4. 13. Folmes CD, Martinez-Fernandez A, Faustino RS, et al. Nuclear reprogramming with c-Myc potentiates glycolytic capacity of derived induced pluripotent stem cells. J Cardiovasc Transl Res 2013;6:10-21. 14. Janiszewska M, Suva ML, Riggi N, et al. Imp2 controls oxidative phosphorylation and is crucial for preserving glioblastoma cancer stem cells. Genes Dev 2012;26:1926-44. 15. Ye XQ, Li Q, Wang GH, et al. Mitochondrial and energy metabolism-related properties as novel indicators of lung cancer stem cells. Int J Cancer 2011;129:820-31. 16. Sancho P, Burgos-Ramos E, Tavera A, et al. MYC/PGC-1alpha Balance Determines the Metabolic Phenotype and Plasticity of Pancreatic Cancer Stem Cells. Cell Metab 2015. 17. Gurumurthy S, Xie SZ, Alagesan B, et al. The Lkb1 metabolic sensor maintains haematopoietic stem cell survival. Nature 2010;468:659-63. 18. Anderson AS, Roberts PC, Frisard MI, et al. Ovarian tumor-initiating cells display a flexible metabolism. Exp Cell Res 2014;328:44-57. Pasto A, Bellio C, Pilotto G, et al. Cancer stem cells from epithelial ovarian cancer patients privilege oxidative phosphorylation, and resist glucose deprivation. Oncotarget 2014;5:430519. 19. 20. Nakajima EC, Van Houten B. Metabolic symbiosis in cancer: refocusing the Warburg lens. Mol Carcinog 2013;52:329-37. 21. Martinez-Outschoorn UE, Prisco M, Ertel A, et al. Ketones and lactate increase cancer cell "stemness," driving recurrence, metastasis and poor clinical outcome in breast cancer: achieving personalized medicine via Metabolo-Genomics. Cell Cycle 2011;10:1271-86. 22. Diehn M, Cho RW, Lobo NA, et al. Association of reactive oxygen species levels and radioresistance in cancer stem cells. Nature 2009;458:780-3. 23. Lamb R, Ozsvari B, Lisanti CL, et al. Antibiotics that target mitochondria effectively eradicate cancer stem cells, across multiple tumor types: Treating cancer like an infectious disease. Oncotarget 2015;6:4569-84. 24. Vazquez-Martin A, Oliveras-Ferraros C, Cufi S, et al. Metformin regulates breast cancer stem cell ontogeny by transcriptional regulation of the epithelial-mesenchymal transition (EMT) status. Cell Cycle 2010;9:3807-14. 25. Pandey PR, Okuda H, Watabe M, et al. Resveratrol suppresses growth of cancer stem-like cells by inhibiting fatty acid synthase. Breast Cancer Res Treat 2011;130:387-98. 26. Mullen AR, Wheaton WW, Jin ES, et al. Reductive carboxylation supports growth in tumour cells with defective mitochondria. Nature 2012;481:385-8. 27. Gupta PB, Onder TT, Jiang G, et al. Identification of selective inhibitors of cancer stem cells by high-throughput screening. Cell 2009;138:645-59. 28. Senkowski W, Zhang X, Olofsson MH, et al. Three-Dimensional Cell Culture-Based Screening Identifies the Anthelmintic Drug Nitazoxanide as a Candidate for Treatment of Colorectal Cancer. Mol Cancer Ther 2015;14:1504-16. 29. Wang YC, Chao TK, Chang CC, et al. Drug screening identifies niclosamide as an inhibitor of breast cancer stem-like cells. PLoS One 2013;8:e74538. 30. Yo YT, Lin YW, Wang YC, et al. Growth inhibition of ovarian tumor-initiating cells by niclosamide. Mol Cancer Ther 2012;11:1703-12. 31. Skrtic M, Sriskanthadevan S, Jhas B, et al. Inhibition of mitochondrial translation as a therapeutic strategy for human acute myeloid leukemia. Cancer Cell 2011;20:674-88. 32. Wheaton WW, Weinberg SE, Hamanaka RB, et al. Metformin inhibits mitochondrial complex I of cancer cells to reduce tumorigenesis. Elife 2014;3:e02242. Kordes S, Pollak MN, Zwinderman AH, et al. Metformin in patients with advanced pancreatic cancer: a double-blind, randomised, placebo-controlled phase 2 trial. Lancet Oncol 2015;16:839-47. 33. 34. Shackelford DB, Abt E, Gerken L, et al. LKB1 inactivation dictates therapeutic response of non-small cell lung cancer to the metabolism drug phenformin. Cancer Cell 2013;23:143-58. 35. Murphy MP. Targeting lipophilic cations to mitochondria. Biochim Biophys Acta 2008;1777:1028-31. 36. Cheng G, Zielonka J, McAllister DM, et al. Mitochondria-targeted vitamin E analogs inhibit breast cancer cell energy metabolism and promote cell death. BMC Cancer 2013;13:285. 37. Chae YC, Caino MC, Lisanti S, et al. Control of tumor bioenergetics and survival stress signaling by mitochondrial HSP90s. Cancer Cell 2012;22:331-44. 38. Chamberlain GR, Tulumello DV, Kelley SO. Targeted delivery of doxorubicin to mitochondria. ACS Chem Biol 2013;8:1389-95. Figure 1 Cancer stem cells in pancreatic cancer progression and metastasis. Intraclonal heterogeneity is formed by CSCs and their differentiated progenies (Left). CSCs are capable of undergoing unlimited cell division while retaining their stem cell identity (self-renewal) and giving rise to non-CSCs with limited proliferative capacity (differentiation). CSCs evolve as the tumour progresses via (epi-)genetic alterations, but also in response to interactions with their niche, leading to diverse CSC subclones with distinct functionality4. Both CSCs and non-CSCs can acquire mobility, which may be driven by EMT processes, but only arising metastatic CSCs can initiate secondary lesions4 and are tractable as circulating CSCs in the blood. These cells must survive the hostile environment of the blood stream, evade immune surveillance and extravasate at a distant location to form metastatic lesions. (Centre) Importantly, circulating CSCs may also evolve, after a period of dormancy, from disseminated non-CSCs through still poorly understood processes. CSCs can also (re)colonize their tumours of origin, or other sites, in a process called “tumour reseeding”. Thus, CSCs circulating in the blood represent metastatic CSCs from various sources (Right). Figure 2 Figure 2. Targeting CSCs through mitochondrial disruption. OXPHOS-dependent CSCs could be eliminated via different strategies aiming to impair their mitochondrial energy metabolism. (1) Direct inhibition of OXPHOS using the antidiabetic agents metformin and phenformin, which inhibit the ETC Complex I. Subsequent energy crisis results in the specific induction of CSC death. (2) Conjugation of pharmacologic agents to mitochondrial carriers such as TPP or mitochondria penetrating peptides to selectively deliver and accumulate them in mitochondria. (3) Chemotherapeutic agents conjugated to mitochondrial carriers to selectively disrupt mtDNA integrity and indirectly block OXPHOS by impairing ETC proteins coded in mtDNA genes. (4) Blockade of mitochondrial protein biosynthesis via inhibition of mitochondrial ribosomes using Tigecycline and other FDA-approved antibiotics. These compounds impair OXPHOS and demonstrated toxicity against CSCs. (5) Similarly, the functionality of ETC components can also be targeted by the mitochondrial delivery of the chaperone inhibitor Gamitrinib. (6) Cell signalling by OXPHOS-generated mitochondrial ROS is crucial for cancer cell proliferation and can be targeted by the mitochondrial accumulation of anti-oxidants such as Mito-Chromanol. Conversely, CSCs can be eliminated by inducing toxic ROS levels in mitochondria using the ROS generator Menadione. (7) Finally, OXPHOS can also be impaired at the level of mitochondrial carbon metabolism, either by altering the enzymes involved in the TCA cycle or fatty acid oxidation (FAO) or by interfering with the supply of mitochondrial fuels.