Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
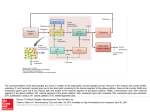
Patterns of Brain Iron Accumulation Luís Antônio Tobaru Tibana Nitamar Abdala Leonardo Modesti Vedolin Rene Leandro Rivero Renato Adam Mendonça Emerson Leandro Gasparetto Ernesto Duarte Alves Felipe Torres Pacheco Matheus Luis de Souza Silva Danilo Manuel Cerqueira Costa Alda Tiaki Sato Tibana Objective The paper presents a new algorithim to evaluate brain iron accumulation in MRI, crystallizing current concepts in radiological practice. Introduction Intracranial iron accumulation can occur in several diseases, with the involvement of the brain parenchyma (more common in the globus pallidus), pial surface, choroid plexus and / or pituitary gland. Iron accumulation appears as hypointense on T2-weighted imaging and isointense on T1. T2*-weigheted imaging may accentuate the degree of hypointensity (“blooming”). Kruer M.C AJNR 2012; 33:407-14 The final etiological diagnosis of brain iron accumulation is done with close clinical correlation. However, we are focusing in those conditions which image pattern is distinct Step 1 – Recognize the pattern Which structures are involved? Distinguish the iron deposit in one of three patterns: - Leptomeningeal - Bone marrow, choroid plexus and pituitary gland - Deep gray matter (globus pallidus) First Step - Recognize the pattern Superficial siderosis Hemochromatosis Hemosiderosis Leptomeningeal Bone marrow, choroid plexus and pituitary gland Deep gray matter (globus pallidus) Neurodegeneration with brain iron accumulation (NBIA) Multiple sclerosis Parkinsonian syndromes Cortical dementias Brain aging Leptomeningeal This is a specific pattern of a condition called superficial siderosis (SS) and results from hemosiderin deposition in the subpial layers of the brain and spinal cord, as a consequence of recurrent and persistent bleeding into the subarachnoid space. Kumar N AJNR 2010; 31:5-14 Accelerated ferritin synthesis in the Bergmann glia of the cerebellum may account for preferential cerebellar involvement Koeppen AH, J Neuropathol Exp Neurol 1988; 47: 249–70 The classic clinical presentation of SS includes ataxia, cerebellar dysarthria and sensorineural hearing impairment Fearnley JM, Brain 1995; 118: 1051–66 Axial T2-weighted brain MR images from patients with SS show hemosiderin deposition along the cerebellar folia and around the midbrain Sagittal T1-weighted brain MR image from a patient with SS shows severe cerebellar atrophy. MR images from the same patient with SS demonstrate superiority of the gradient-echo technique in detecting the characteristic T2 hypointensity (blooming effect) Bone marrow, choroid plexus and pituitary gland Primary or secundary hemochromatosis (patients with transfusiondependent b-thalassemia major) lead to intracranial iron accumulation at sites outside the blood-brain barrier, which include the pituitary gland, choroid plexus, pineal gland, and area postrema. The involvement of this p’s is highly suggestive of primary or secundary hemochromatosis. Another site that can be included as typical iron deposit in hemochromatosis is bone marrow Drayer B AJR 1986;147:103–10 Wahid S Lancet 2001;357:115 28-year-old woman with transfusion-dependent b-thalassemia major. Pituitary siderosis Bone marrow siderosis Sagittal T1-weighted The bone marrow shows markedly decreased signal intensity Coronal T2 - weighted The anterior lobe of the pituitary gland shows markedly decreased signal intensity 28-year-old woman with transfusion-dependent b-thalassemia major. Axial T2* - weighted GRE The choroid plexus shows markedly decreased signal intensity Choroid plexus siderosis Deep gray matter Unlike the previously shown image patterns, iron accumulation in the deep gray matter is usually not specific, being common in several diseases and even in the normal aging brain. Iron deposition occurs in multiple sclerosis, human immunodeficiency virus dementia, Freidrich ataxia, Alzheimer and Parkinson diseases, though to a lesser degree than that seen in NBIA. Regardless of etiology, the globus pallidus is usually the most involved region. Although in most cases of NBIA, the image pattern is nonspecific with the diagnosis being performed with clinical data and especially using genetic analysis, sometimes it is possible to distinguish specific subpatterns. Kruer M.C AJNR 2012 33:407–14 For this image pattern (deep gray matter), apply Step 2 Step 2 - Deep gray matter If your case fit into one of the image patterns below, there is good specificity! These five image patterns are distinct. Iron deposits in the globus pallidus + Eye of the tiger Midbrain T1 hyperintensity Linear hyperintensity of the medial medullary lamina (“Japanese eye of the tiger”) Widespread homogeneous iron deposits in deep gray matter Widespread heterogeneous iron deposits in deep gray matter If not, the diagnostic challenge continues, requiring a close correlation with clinical data, laboratory tests and in many cases, genetic analysis. Kruer M.C, Brain 2011;134(pt 4):947–58 Kruer M.C AJNR 2012 33:407–14 Amaral LLF J Neuroimaging 2014;00:1-13 Hogarth P Neurology 2013;80:268-275 “Eye of the tiger” Pantothenate Kinase-Associated Neurodegeneration (PKAN) is the most frequently encountered subtype of NBIA. Classic PKAN begins in childhood. The “eye of the tiger” sign is virtually pathognomonic of the PKAN (mutation in PANK2) and may become more intensified or may fade with time. This is characterized by a T2-weighted hypointense globus pallidus with a central T2 hyperintensity. Other forms of NBIA have been purported to exhibit an eye of tiger but feature subtle differences in the appearance of the globus pallidus lesion. Kruer M.C, Brain 2011;134(pt 4):947–58 Kruer M.C AJNR 2012 33:407–14 Chang CL Brain Behav 2011;1:55-56 PKAN Eye-of-the-tiger sign Axial FLAIR and axial T2-weighted image demonstrates increased T2 signal in the center of globus pallidus Axial GRE image through the same level demonstrates hypointensity secondary to iron deposition in the posterior and lateral aspect of globus pallidus Midbrain T1 hyperintensity Before named SENDA (Static encephalopathy of childhood with neurodegeneration in adulthood) due to the clinical course, BetaPropeller Protein-Associated Neurodegeneration (BPAN) is now known a X-linked NBIA subtype with an unusual pattern of neurodegeneration. The neuroimaging of BPAN is distinct. In addition to iron deposition in the globus pallidus and substantia nigra, BPAN features T1 hyperintensity of the substantia nigra with a central band of hypointensity. Amaral LLF J Neuroimaging 2014;00:1-13 Kruer M.C AJNR 2012 33:407–14 BPAN Axial T1-weighted demonstrates hyperintensity of the substantia nigra and cerebral peduncles with central linear hypointensity Axial GRE demonstrates hypointensity secondary to iron deposition in the substantia nigra and cerebral peduncles Linear hyperintensity of the medial medullary lamina (“Japanese eye of the tiger”) Distinctive imaging abnormality of Mitochondrial Membrane ProteinAssociated Neurodegeneration (MPAN) is linear T2 hyperintensity involving the medial medullary lamina between globus pallidus (internal and external segments). This imaging finding is present in about one-fifth of patients MPAN is caused by mutations in the C19orf12 gene (autosomal recessive) Hogarth P Neurology 2013;80:268-275 Hartig M, Int Rev Neurobiol 2013;110:73-84 The “japanese eye-of-the-tiger sign” Axial T2-weighted and axial GRE image demonstrates linear hyperintensisy of the medial medullary lamina in the center of globus pallidus The “japanese eye-of-the-tiger sign” Coronal T2-weighted image demonstrates linear hyperintensity of the medial medullary lamina in the center of globus pallidus. There is also iron deposition in the substantia nigra Widespread homogeneous iron deposits in deep gray matter In aceruloplasminemia (ACP), MR imaging demonstrates widespread brain iron accumulation, predominantly involving caudate, putamen, globus pallidus, thalamus, red nucleus, and dentate. This is similar to what occurs in neuroferritinopathy but in contrast to most other forms of NBIA. ACP is an autosomal recessive disease caused by mutation of the ceruloplasmin gene (CP), located on chromosome 3q In ACP, the iron deposition is homogeneous and widespread in deep gray matter Amaral LLF J Neuroimaging 2014;00:1-13 Kruer M.C AJNR 2012 33:407–14 Aceruloplasminemia Axial T2-weighted and axial GRE image demonstrates homogeneous iron deposition in caudate, putamen, globus pallidus and thalamus Widespread heterogeneous iron deposits in deep gray matter Neuroferritinopathy is the only subtype of NBIA inherited as an autosomal dominant caused by mutations in the FTL gene (Huntington disease phenocopy) Distinct MRI findings in NFT demonstrate bilateral, cystic degeneration and heterogeneous iron deposition involving caudate, putamen, globus pallidus and thalamus Kruer M.C AJNR 2012 33:407–14 Chinnery PF Brain 2007;130(pt 1):110 –19 Amaral LLF J Neuroimaging 2014;00:1-13 Courtesy of Lázaro L.F. Amaral Axial T2-weighted and axial GRE image demonstrates cavitations in putamen and globus pallidus, with heterogeneous iron deposition