Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
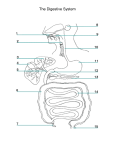
Gastrointestinal (GI) Physiology • • The abdomen is divided into 4 quadrants designated using the midline to separate left vs right, and the umbilicus which separates the superior vs inferior. These designated quadrants are called: • Right upper quadrant (RUQ), Right lower quadrant (RLQ), Left upper quadrant (LUQ), and Left lower quadrant (LLQ) When doing a physical exam upon a patient with an abdominal complaint it is very important to designate which quadrant the patient is complaining about. There are specific pathology associated which each quadrant that may narrow a differential diagnosis. Anatomy of the GI Tract • The gastrointestinal tract is one continuous tube which stretches from the mouth (oral cavity) all the way to the anus. • The primary function is to serve as a portal in the absorption of nutrients, drugs and water. • Colonized from birth with a large number of commensal bacteria especially in the colon which performed 2 functions: Metabolic functions & Protection against potential pathogenic microorganisms. • Alterations of bacterial content can introduce pathogenic bacteria such as Clostridium difficile causing Clostridium difficile diarrhea or a more severe condition Clostridium difficile infection • The GI Tract starts with the MOUTH (teeth & salivary glands) → esophagus → stomach → duodenum (Pancreatic enzymes and bile mix) → jejunum → ileum → through the Cecum (ileocecal valve located near the appendix) → Colon (Ascending, Transverse, Descending, and Sigmoid colon) → ANUS • SPHINCTERS • Gastroesophageal sphincter (between esophagus and stomach), Pyloric sphincter (junction between stomach/pylorus and the duodenum), Ileocecal valve (valve at the terminal ileum leading into the ascending colon and prevents colonic contents and bacteria from moving backwards), Inner and outer sphincters at the anus allowing bowel control. • Within the lining of the intestines are epithelial like projections called villi which increases the surface area. This is particularly TRUE in the jejunum where the majority of nutrient and drug absorption happens. This entire epithelium replaces itself every few days Oral Cavity The oral cavity (mouth) initiates the digestive process with teeth to chew up food Saliva: • Assist with the digestion of starches • Protection of the oral cavity • Lubricates the food bolus which allows easier swallowing Electrolytes: (LOW in ↓Na+ and ↓CL-) (HIGH in ↑K+ and ↑HCO3-) • • Our bodies produce 1000 - 1500 mL of saliva every day • Saliva is governed by the Parasympathetic nervous system • In flight or fight mode (sympathetic nervous system) hunger is not experienced Stomach • As we progress further down the esophagus through the Lower esophageal sphincter, and into the stomach. • The stomach has 3 major parts the Fundus (most upper portion), Antrum (holding place for food bolus and secretes mucus, pepsinogen and gastrin) and Pylorus. 1 • • • • • • • • • The stomach is responsible for controlling the rate of food / nutrition and medication delivery into the small intestine. The stomach requires at least 240 mL to empty. Counsel patients to take medications with a full glass of water so the stomach can empty. The stomach is also controlled by the parasympathetic nervous system via the vagus nerve with acetylcholine as a primary neurotransmitter. This is responsible for peristalsis and emptying. The stomach’s gastric parietal cells secrete hydrochloric acid (HCL). • This is accomplished by a mitochondrial driven hydrogen potassium ATPase pump a.k.a. “proton pump” moving hydrogen into the stomach in exchange for potassium. The stomach is normally acidic with a pH of ~ 1 causing a need for an active pump, to pump more acid into the stomach and against the concentration gradient. The pump is activated by three receptors gastrin, histamine, and acetylcholine. The stomach produces approximately ~2.5 L of fluid per day even if the person eats or not. The stomach electrolytes are important when talking about pathophysiology of different gastrointestinal disease states. The stomach is very high in potassium, chloride, hydrogen, and calcium. • Patients who are vomiting present with low serum potassium, chloride and calcium levels. Duodenum (1st portion of small intestine) • Again, progressing further down the GI tract past the pyloric sphincter and into the duodenum (1st segment of the small intestine). • The duodenum is the very critical regulator of both digestion and absorption. The ampule of Vader releases the contents of the pancreas and the common bile duct releases bile into the duodenum. • The pancreatic juice is extremely alkaline ~pH 8. This is due to the very high quantity of bicarbonate in the pancreatic juice (~113 mEq NaHCO3/L versus 24 mEq NaHCO3/L in plasma) • This digestion and regulation is facilitated by bile, and pancreatic enzymes (amylase and lipase) • The bicarbonate from the pancreatic juice will neutralize the acidic content of the stomach • The pancreatic enzymes amylase and lipase will facilitate digestion • The Bile will assist with digestion and absorption (via emulsification) of the fat content in a meal • ~ 95% of your bile acids are reabsorbed in the terminal ileum and reused via hepatic recirculation. • The pH of the duodenum is ~6-7 resulting from the bicarbonate within the pancreatic juice • The duodenum, unlike the stomach, is very high in sodium, chloride and magnesium (not potassium). • It is not uncommon in patients who have small bowel fistulas of the duodenum to become hyponatremic due to the loss of sodium or hypomagnesemia from loss of magnesium. Jejunum (2nd portion of small intestine) • The Ligament of Treitz separates duodenum from jejunum • There is minimal digestion occurring in the jejunum, but a Majority of drug and nutrient absorption due to the extremely high surface area • The jejunum is the shortest part of the small intestine, but has a surface area larger than the other 2 combined • Patients being fed into the jejunum (jejunostomy) will bypass bile and pancreatic enzymes requiring a ready to absorb nutrient formulation & altering drug dosage form • The pH of the jejunum is ~7 (neutral) this pH will remain constant throughout the remainder of the small intestine, and large bowel. • The major electrolytes are sodium, potassium, and chloride • A patient with a fistula (loss) within the jejunum will lose a high amount of sodium Ileum (3rd portion of small intestine) • The ileum serves as an anatomic reserve if jejunal absorption impaired • Patients who lose part of their jejunum can use their ileum to replace that section, and the Ileum will adapt by absorbing nutrients, and medications. This adaptation may take several weeks. 2 • • • The ileum has a very neutral pH of ~7, and the electrolytes are the same as those in the duodenum and jejunum with a high concentration of sodium, potassium, and chloride. Patients with an end ileostomy no longer have a large intestine causing large amounts of volume/electrolytes loss leading to dehydration and the need for electrolyte replacement The ileum contains liquid stool and electrolytes Colon • Past the terminal ileum and through the cecum valve we enter the Colon • The last portion of your intestine is the colon, and is a reservoir for storage of waste and indigestible materials (fiber, etc.). • There is a minimum nutrient absorption in the colon, BUT the majority of water reabsorption will occur in the colon. • The colon also has a neutral pH of ~7. • With the major electrolytes again being sodium, potassium, and chloride. • Again, in patients with diarrhea these are the electrolytes they are going to lose. Patient Case #1 • 37 year-old female • CC: Presented with the Right Upper Quadrant (RUQ) abdominal, that became worse after eating • PE: tender to palpation in the RUQ What diagnostic data do you need? Evaluating Your Patient • Thorough Past Medical History – has she ever had these symptoms before? Pain worse after eating? • Common Signs/Symptoms: • Abdominal pain • Heartburn or dyspepsia – Remember our patient said that the pain is worse after she eats. • Nausea/Vomiting/Diarrhea/Constipation – When was the last bowel movement? • Bleeding (melena, hematemesis, etc) – Asked patient if they are having dark tarry stools (melena). Is the patient having bright red blood in their feces? Are they throwing up blood? Complete medication history – Take a very detailed medication history remembering also over-the• counter medications. The patient may be taking (ibuprofen, naproxen, other NSAIDs, etc.). Asked the patient if they take an aspirin every day. Laboratory Studies commonly obtained • Complete Metabolic Panel (CMP) • This will show your common electrolytes, renal function (BUN, serum creatinine, serum glucose) • The CMP also includes liver function test (LTF) this can give you an idea, especially if the patient is having right upper quadrant pain, if the liver is involved by looking at the total bilirubin, liver enzymes, and albumin. This could suggest a bile outflow problem • Complete blood count (CBC) – High WBCs could suggest infection LOW Hgb/Hct could suggest bleeding • Lipase and Amylase • Especially with the patient who has right upper quadrant pain. • Everyone has a certain amount of pancreatic enzymes that are normally spilled into the bloodstream, but if these are profoundly elevated it denotes that the patient’s pancreas is inflamed. • Stool culture • Are minimally helpful, but do help in patients with an infectious diarrhea • Toxin Assay or Toxin PCR for C. Difficile • The assay looks for the toxin being produced whereas the PCR looks for bacteria. Particularly clostridium difficile in patients who have had recent antimicrobial therapy and diarrhea • Serum antigen for Helicobacter Pylori • Peptic ulcers may be caused by the bacteria H. Pylori 3 Patient Case #1 • RUQ pain • Pertinent Laboratory Results: patient has a mildly elevated AST, ALT, and total bilirubin. This would suggest that something is going wrong either in the gallbladder or the liver, and for both more information is needed. • Part of this lecture is to give practical applications for the various radiologic studies that are available, and decide which is more appropriate for a particular patient. • AST - 231, ALT - 291, and Total bilirubin - 4.3 (nl<2) are all elevated Which radiologic or invasive studies are most appropriate for this patient? Radiologic/Invasive Studies Listed in range of complication (easy → more invasive) KUB & Upper GI Series Kidney /Ureters /Bladder X-ray (KUB) - plan film of the abdomen cavity • Diagnostic for a couple of indications: • Free air (perforation) – which is air outside the GI tract • KUB also shows small bowel/colonic dilation • Upper GI Series – series of KUBs after contrast • This takes the KUB further by having patients take oral contrast to assess the integrity of the gastrointestinal tract. • Here the patient swallows oral contrast typically a water-soluble oral contrast (gastrographin®) • This helps us to diagnose where the small bowel obstruction is occurring, and look for anastomotic leaks after a bowel surgery. It also can help finding the location of a fistula. • If a patient has a fistula the KUB will determine how distal it is from the stomach. A distal ileum fistula can probably be fed enterally or orally. A proximal fistula in the duodenum/jejunum will lose a lot of volume and probably need parenteral nutrition Ultrasound It is very inexpensive, simple to do, and can be done at the bedside • Modality of choice for diagnoses of: • Cholelithiasis – gallstones • Cholecystitis – inflammation of the gallbladder +/– stones • May also identify choledocholithiasis – a gallstone that is obstructing the common bile duct. • Safe in pregnancy – cholelithiasis and cholecystitis are not uncommon in pregnancy CT Abdomen/Pelvis • Typically done both with & without contrast • IV + Oral is ideal +/– Rectal (which assesses the sigmoid colon or rectum) • Allows good visualization of abdominal viscera (liver or spleen) • IV Contrast enhances vascular system MRI / MRCP Magnetic Resonance Cholangiopancreatography (MRCP) • • Another alternative in pregnant patients when you need better visualization of the abdomen. • MRCP: • Provides good visualization of liver & common bile duct (CBD) • Used as a confirmatory test when trying to figure out: • Common bile duct obstruction • Pancreatic masses that maybe causing obstruction or pain (cancer) • Liver masses (cancer) 4 ERCP • Endoscopic Retrograde Cholangiopancreatography (ERCP) – this is more invasive procedure conducted by a gastroenterologist where a endoscope is inserted through the mouth and passed through the esophagus, stomach and into the duodenum and up the ample of Vader looking into the common bile duct. • Performed under conscious sedation • Both diagnostic and treatment • Dilate the ampulla of Vater, Retrieve/remove CBD stones, or Place stents to relieve an obstruction • Complication: ~1-7% of patients develop post-procedural pancreatitis from the procedure Laparoscopy/Laparotomy • Laparoscopy • Minimally invasive surgery done through small incisions in the abdominal wall, and is videoassisted. Commonly used for cholecystectomy – removal of the gallbladder • Laparotomy – most invasive of all procedures • Open exploration of the abdomen typically this is a midline incision starting at xiphoid process and going down to the umbilicus. Allows surgeon direct visualization of the abdominal contents. Patient Case #1 • Working Diagnosis: cholelithiasis – “formation of gallstones” • She has right upper quadrant pain • She has an elevated total bilirubin, and mildly elevated AST and ALT • Gallbladder Ultrasound showed that she had: gallstones, mild gallbladder wall thickening (indicative of cholecystitis), and common bile duct (CBD) dilatation • MRCP showed that she had a 9 mm CBD stone DIAGNOSIS: choledocholithiasis with cholecystitis– “presence of a gallstone in the common bile duct • & mild gallbladder wall thickening” • ERCP was performed where they dilated ampulla of Vater for a CBD stone extraction • Post-ERCP Laboratory Results: AST-91, ALT-29, Total bilirubin-1.9, and Lipase-208 • Patient does develop mild post ERCP pancreatitis with a Lipase of 208. Total bilirubin is now 1.9, and this is because the stone has been extracted. • The plan now is to allow the patient to rest for a day to let her pancreas “cool-down” (lipase < 100) and to do a laparoscopic cholecystectomy (removal of the gallbladder) Summary • GI tract is one continuous tube from mouth to anus • The physiology changes from stomach to small intestine to the colon • Stomach is acidic, the we enter neutral pH in the small intestines and colon, most drug absorption is in the jejunum (important to keep in mind) • Thorough history & physical – important to have before making diagnosis of gastrointestinal pain, and do not forget medication history especially over-the-counter agents • Multiple diagnostic modalities Enteral Medication Administration Key anatomical landmarks Pyloric sphincter – (1st and most important landmark) post-pyloric feeding into the duodenum/jejunum Ligament of Treitz – differentiates the transition from duodenum to jejunum • Feeding the jejunum bypasses the large majority of the digestive system (stomach, duodenum, pancreas) • Good way of feeding patients with pancreatitis. Feeding here will change medication dosage form and type of feeding (pre-digested feeding) significantly once past the ligament of Treitz. Enteral Access Routes 5 Gastric feeding – Feeding into the stomach Types of Feeding Tubes • Nasogastric (NG) tube – Placed nasally and ends in the stomach (uncomfortable, maybe result in sinusitis) • Orogastric (OG) tube – Placed orally and ends in the stomach (uncomfortable) • Percutaneous endoscopic gastrostomy (PEG-tube) – placed percutaneously • Gastrostomy tube (G-tube) – placed surgically • PEG-tube, and G-Tube are for long-term use and allows removal NG & OG tubes • Used for decompression of the stomach OR provision of enteral nutrition • All of these tubes are large bore making it more difficult to clog and easy to flush • Allows bolus (intermittent) or continuous feeding • Bolus dosing 250-500 mL / dose • Continuous infusions – no maximum rate • May have residuals – Some of the CONCERNS • Gastroparesis – not having appropriate emptying of the stomach (check residuals q4hrs with the goal of < 250ml) • Increase the risk of aspiration – Because tubes are keeping the esophageal sphincter open • Drug / nutrient dissolution approaches normal physiology (BIGGEST advantage of gastric feeding) Small Bowel Feeding Duodenum • Small tube (patient comfort) • Post-pyloric sphincter feeding – Bypasses the stomach, Decreased risk of aspiration, and No gastric residuals due to continuous peristalsis • No gastroparesis as seen with gastric feeding • Most are placed nasally Nasoduodenal) • Continuous feeding only • Tolerates tube feed rates up to ~120ml/hr • Normal bile / pancreatic enzyme activity • Not a significant decrease in both nutrient/drug digestion and absorption Jejunum • Nasojejunal feeding • Jejunostomy tube (J-tube) – permanent • Surgically placed, Very small bore, and Clogs very easily Reason for a J-tube is because the use of the • stomach or duodenum or NOT an option (e.g. Cancer, etc.) • Continuous feeding only – Maximum rate ~80 ml/hr • Bypasses pancreas – May require “pre-digested” enteral nutrition • Drug formulation important for a maximal absorption and NOT to clog the feeding tube Enteral Access & the Pharmacist • Clarify the type of feeding tube • Profile review for medications: • Medications that can’t be crushed (sustained release, etc.) • Enteric coated medications • Medications dependent on stomach acid for activity • Medication site of action (sucralfate, antacids only work in stomach) • Gastric tubes (NG, OG, PEG, G-tube) • Large bore • May crush medication and administer • Bolus or continuous feeds • Duodenal or Jejunal tubes • Liquid medication preferred, because it to be so small • Avoid crushing any medications to give via J-tube • Continuous feeds (bigger problem with drug-nutrient interactions) 6 Type of Feeding Tube Naso/Orogastric (short term) Nasoduodenal/jejunal (short term) Gastrostomy (long term) Jejunostomy tube (long term) Pros Cons • Large bore • Feeding the stomach bolus/continuous feeds • High aspiration risk • Reflux • Sinusitis • • • • • Clog easily • Bypasses stomach Small bore Post-pyloric feeding Minimizes aspiration risk Continuous feeds only • Large bore • Feeding the stomach bolus/continuous feeds • Increased aspiration risk • Dislodgement • Small/medium bore • Continuous feeding only • Bypass stomach/duodenum • Leaks at insertion site • Clog easily • Dislodgement Drug delivery Drug Delivery • GI tract absorption dependent on • Surface area • Blood flow to site of absorption • Water solubility of the drug • Drug concentration at the absorption site • Majority occurs in duodenum & jejunum Drug Properties • Physical state of the drug • Solution versus Suspension, versus Solid (tablet / capsule) • Immediate release preparation • Enteric coating • Controlled release formulation Drug Properties: Physical State Solution: • Clear ± Color • No dissolution required • Rapid absorption in duodenum & jejunum • Ideal for small bowel feeding/drugs Suspension • Particles in a suspending vehicle • Requires further dissolution • Better for drugs poorly water soluble Solid • Requires initial breakdown in the stomach • Absorption rate governed by rate of dissolution • Allows for controlled release formulation • Difficult to administer to patients without oral access Controlled Release • Intended to decrease dosing frequency • May not be chewed or crushed • Crushing a controlled release formulation destroys the controlled release mechanism and causes a High risk for adverse drug events • Must be converted to “immediate release” dosage forms • MICROMEDEX® – complete list of drugs that cannot be crushed 7 Common CR Conversions Controlled release dose/frequency → Immediate release conversion Diltiazem CD 240 mg PO Q24 hours → Diltiazem 60 mg PT Q6 hours Metoprolol succinate XL 100 mg Q24 hours → Metoprolol tartrate 50 mg PT Q12 hours (compound susp) Isosorbide mononitrate 30 mg PO Q24 hours → Isosorbide dinitrate 10 mg PT tid Nifedipine XL → do not convert to immediate release “call physician” for alternative medication Morphine sulfate SR 60 mg PO Q12 hours → Morphine sulfate IR 30 mg PT Q6 hours Oxycodone SR 40 mg PO Q12 hours → Oxycodone 20 mg/ml PT Q6 hours Patient Case #2 • 70 year-old female presents in status epilepticus • Intubated by the ICU team and nasoduodenal feeding tube placed • Current medication orders: • Gabapentin 500mg PO Q8H, Amlodipine 10mg PO Q24H, Pantoprazole 40mg PO Q24H, Morphine XR 100mg PO Q12H, Morphine IR 15mg PO Q4-6H PRN pain, Prednisone 10mg PO Q24H, and Ranolazine XR 500mg PO Q12H • Convert to liquid formulation when possible What recommendations do you make? Current Therapy Recommendation Gabapentin 600mg PO Q8H Gabapentin solution 250mg/5mL 600mg (12mL) PT Q8H Amlodipine 10mg PO Q24H Amlodipine 1mg/mL compound susp. 10mg (10mL) PT Q24H Pantoprazole 40mg PO Q24H Pantoprazole granules 40mg PT Q24H Dissolve in 10mL apple juice (to provide acidic environment) Flush with additional 10mL apple juice Morphine XR 100mg PO Q12H Morphine 20mg/mL oral solution 50mg (2.5mL) PT Q6H Morphine IR 15mg PO Q4-6H PRN pain Morphine 4mg/mL oral solution 15mg (7.5mL) PT Q4H prn pain Prednisone 10mg PO Q24H Prednisone 1mg/mL oral solution 10mg (10mL) PT Q24H (in AM) Ranolazine XR 500mg PO Q12H Hold for now (no enteral alternative) 8 Drug properties and Administration Drug Properties: Enteric Coating • Enteric coat designed to: • Decrease gastric irritation • Protect the drug from stomach acid • To delay release of the drug • Crushing removes enteric coat • Enteric coating does not dissolve easily – clog tubes • Switch to non-enteric coated product or alternative agent Common Enteric Coated Medications • Aspirin, Proton pump inhibitors, Non-steroidal anti-inflammatory medications (NSAID), and Sulfasalazine Drug Administration • Flush feeding tube before and after • 30mL for adults & 10-15mL for pediatrics • Know location of feeding tube • Solid vs. Solution vs. Suspension • Avoid mixing medications with enteral nutrition • Pause enteral feeding, flush tubing, administer medication, flush tubing again, reinitiate enteral nutrition Drug-Enteral Nutrition Interactions • May decrease bioavailability when given with food – Levothyroxine & Phenytoin • Enteral nutrition may bind & inactivate medication (Iron) – Fluoroquinolones & Tetracycline • Acid vs. Basic administration – Proton pump inhibitors (apple juice with pantoprazole granules) Drug-enteral nutrition interactions Drug Interaction Possible Solutions Levothyroxine • Decreased absorption • Hold TF 1hr before & 1h after each dose • OR increase dose Fluroquinolones • Binding by divalent & trivalent cations in tube feed • Hold TF 1h before & 1h after each dose Lansoprazole Omeprazole • Inactivation of delayed-release base-labile granules • Clog feeding tube • Extemporaneous oral suspension • Dissolve granules in juice • Flush feeding tube thoroughly Phenytoin • Reduced bioavailability • Hold TF 1h before & 1h after each dose • Monitor serum phenytoin levels • Change to IV phenytoin Warfarin • Increased Vitamin K in enteral nutrition formulas • Increase warfarin dose • Frequent PT/INR checks Special Situations • Gastroparesis – inadequate emptying of the stomach. Use metoclopramide or erythromycin or convert patient from gastric feeding to duodenum/jejunum feeding till gastroparesis resolves • Gastric dumping – Common in patients with gastric bypass surgery. Caused by high concentrations of sugars resulting in a rapid stomach emptying resulting in inadequate absorption and diarrhea • Small bowel fistulas – cause significant problems in absorbing nutrition/ medication and volume losses with electrolyte abnormalities requiring parenteral nutrition & convert drugs to IV when possible • Proximal (duodenum/jejunum) • Distal (ileum) 9 • Colonic fistulas – may have volume loss/diarrhea, but otherwise functions as an end colostomy with little impact on medication/nutrient absorption Patient Case #2 • 87 - year-old female s/p auto versus pedestrian • Multiple facial fractures • Subarachnoid hemorrhage • Enteral nutrition started (nasogastric tube) • Current (pertinent) medications: • Metoprolol 5 mg IV Q4H • Levetiracetam 500 mg IV Q12H • Famotidine 20 mg IV Q24H • Can we now switch her medications to enteral formulations? This could save nursing time, cost for the institution, and patient cost for their hospitalization. Levetiracetam IV is very expensive. Recommendations: • Metoprolol 5 mg IV Q4H → Metoprolol 25 mg NG Q12H (~ 50% oral bioavailability) (compound susp.) • Levetiracetam 500 mg IV Q12H → Levetiracetam 500 mg NG Q12H (liquid) • Famotidine 20 mg IV Q24H → Famotidine 20 mg NG Q24H (liquid) Patient Case #3 • 65-year-old male s/p acute myocardial infarction • PMH: HTN, atrial fibrillation • Home Meds: • Diltiazem CD 240 mg PO Q24H • Lisinopril 20 mg PO Q24H • Enteric coated Aspirin 81 mg PO Q24H • Clopidogrel 75 mg PO Q24H • Physician starting enteral nutrition • • • • • Recommendations: Diltiazem CD 240 mg PO Q24H → Diltiazem 60 mg PT Q6H (crush) Lisinopril 20 mg PO Q24H → Lisinopril 20 mg PT Q24H (crush) EC ASA 81 mg PO Q24H → Aspirin (baby) 81 mg PT Q24H (crush) Clopidogrel 75 mg PO Q24H → Clopidogrel 75 mg PT Q24H (crush) Patient Case #4 • 65 - year old female, nursing home resident • S/p (status post) stroke • Enteral nutrition through a percutaneous enteral gastrostomy (PEG-tube) • New urinary tract infection with Pseudomonas aeruginosa • Physician wants to discharge on enteral Ciprofloxacin • 3 dosage forms for Ciprofloxacin dosage forms: • Intravenous, Oral (tablet), and Oral suspension (microcapsules) • Enteral feeding concerns • Decreased bioavailability ~ 30% if given in conjunction with enteral nutrition • Suspension may bind to feeding tube • Recommendations: • Avoid suspension • Crush tablet • Hold tube feeds 1 hour before and 1 hour after each dose • Adjust tube feed rate to compensate • Alternatives: • Continue IV therapy • Choose alternative IV agent Take Home Points • GI Physiology • Identify the various portions of the GI tract • Anticipate potential problems depending on the location • Enteral Medication Administration 10 • • • Know your enteral access route • Know your dosage forms and intervene • Make sure the orders reflect the route Some patients will have both a gastrostomy tube and a jejunostomy tube. The gastrostomy tube will be used for stomach decompression and the jejunostomy tube will be used for feeding and drug delivery. Make SURE all medications go through jejunostomy tube 11