Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
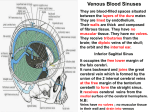
CEREBRAVASCULAR ANATOMY VENOUS SYSTEM&PATHOLOGIES Eylül YERAL • The cerebral venous system, unlike the majority of the rest of the body, does not even remotely follow the cerebral arterial system • The cortical veins lie superficially, unlike cortical arteries, and are adherent to the deep surface of the arachnoid so that they keep the sulci open • Cortical veins then drain to the nearest dural venous sinuses. Such as the superior sagittal sinus and the straight sinus to the the confluence of sinuses, then to the transverse sinuses, sigmoid sinuses and internal jugular veins. • The whole system may be divided into some sections: • Cerebral Veins • superficial • deep • Dural venous sinuses • The cerebral veins drain the brain parenchyma and are located in the subarachnoid space. They pierce the meninges and drain further into the cranial venous sinuses. • The cerebral veins lack muscular tissue and valves. -superficial (cortical) cerebral veins -deep (subependymal) cerebral veins Superficial Venous System • Comprised of the sagittal sinuses and cortical veins. • The cortical veins course along the cortical sulci, drain the cortex and some of the adjacent white matter. • Can be subdivided into superior, middle and inferior groups. • Important veins of superficial cerebral venous system; -Superficial middle cerebral vein -Superior anastomotic vein of Trolard -Vein of Labbé Superficial Middle Cerebral Vein • Runs along the lateral sulcus-also known as Sylvian Vein • Drains into the sphenoparietal sinus or cavernous sinus • Connected with superior sagittal sinus via great anastomotic vein of Trolard, and with transverse sinus via posterior anastomotic vein of Labbé. Vein Of Labbé • Largest channel that crosses the temporal lobe between the Sylvian fissure and the transverse sinus • Surgically it is of importance in planning temporal lobectomy for refractory temporal epilepsy, as the vein should be preserved, often requiring some cortical tissue to be left behind. This is especially the case in the 10% of cases where the vein is located anteriorly. Deep Cerebral Veins • Drain deeper parts of hemispheres, basal nuclei, internal capsule, diencephalon and choroid plexus • Consists of the lateral sinuses, sigmoid sinuses, straight sinus and draining deep cerebral veins (subependymal and medullary veins) -Medullary veins are numerous and originate 1-2 cm below cortical gray matter and pass through deep medullary white matter and drain into subependymal veins. -Subependymal veins receive medullary veins and aggregate into greater tributaries, mainly into septal veins, thalamostriate veins, internal cerebral veins, basal vein of Rosenthal and vein of Galen. Vein Of Galen • Formed by the union of the two internal cerebral veins and basal veins of Rosenthal • Drain into the confluence of the inferior sagittal sinus and the anterior extremity of the straight sinus Vein Of Galen Malformation • The most frequent arteriovenous malformation in neonates. • Results from an aneurysmal malformation with an arteriovenous shunting of blood • Develops during weeks 6-11 of fetal development as a persistent embryonic prosencephalic vein of Markowski • Typically result in high-output congestive heart failure or may present with developmental delay, hydrocephalus, and seizures.(vary with the type of malformation) • Has been associated with capillary malformationarteriovenous malformation (CM-AVM), which is a newly recognized autosomal dominant disorder, caused by mutations in the RASA1 gene in 6 families • Presentation commonly with high output cardiac failure in neonates while mostly hydrocephalus in infants and children • Angiography:gold std • Classification - Lasjaunias classification: Choroidal: tend to present earlier (neonate) with more severe shunts&high output cardiac failure Mural: present later (infant) and typically with hydrocephalus. Fewer fistulas-high outflow restriction -Yasargil Classification type I: small pure cisternal fistula between the vein of Galen and either the pericallosal arteries (anterior or posterior) or posterior cerebral artery type II: multiple fistulous communications between the vein of Galen and the thalamoperforating vessels type III: high flow mixed type I and II type IV: parenchymal arteriovenous malformation (AVM) with drainage into the vein of Galen Tx&Prognosis • Arterial feeder and fistula occlusion • Transtorcular or transvenous embolisation of the dilated vein • Prognosis is largely determined by the presence or absence of cardiac failure. Thus choroidal types and those presenting in the neonatal period do poorly. Dural Venous Sinuses • Venous channels located intracranially between the two layers of dura mater (endosteal layer and meningeal layer) • Unlike other veins in the body they run alone, not parallel to arteries • They are valveless, allowing for bidirectional blood flow in intracranial veins. • Together the dural venous sinuses form the major drainage pathways from the brain, predominantly to the internal jugular veins. • https://www.youtube.com/watch?v=Dc-z7bDD-KM Dural Venous Sinuses Paired • • • • • • • transverse sinus sigmoid sinus superior petrosal sinus inferior petrosal sinus cavernous sinus sphenoparietal sinus basilar venous plexus Unpaired • • • • • superior sagittal sinus inferior sagittal sinus straight sinus occipital sinus intercavernous sinus Cavernous Sinuses Located on either side of the pituitary fossa and body of the sphenoid bone between the endosteal and meningeal layers of the dura. (lateral and superior to the sphenoid sinus and are immediately posterior to the optic chiasm) • Boundaries: Roof: fold of dura mater attached to the anterior and middle clinoid processes Anterior wall:medial end of the superior orbital fissure Posterior:petrous apex Medial: endosteum of body of the sphenoid bone Lateral:dura mater from the ridge of the roof to the floor of the middle cranial fossa Floor: greater wing of sphenoid bone Cavernous Sinus • Receive venous blood from the facial veins (via the superior and inferior ophthalmic veins) as well as the sphenoid and middle cerebral veins(-inferior &superior petrosal sinusessigmoid-ijv) • Because of this complex is made of valveless veins, blood can flow in any direction depending on the prevailing pressure gradients. Since the cavernous sinuses receive blood via this distribution, infections of the face including the nose, tonsils, and orbits can spread easily by this route. Cavernous Sinus Cavernous Sinus Thrombosis • Rare, high mortality&morbidity Etiology, • Infections: -Most commonly results from contiguous spread of infection from the sinuses or middle third of the face(furuncle), or less commonly dental abscess or orbital cellulitis -Staph. Aureus (%55) • Sinus compression, e.g. trauma, tumour • Procoagulable conditions, e.g. Protein C/S deficiency, OCP use, malignancy • Idiopathic (25%) • Headache(m.common) • focal cranial nerve abnormalities • periorbital edema and visual disturbances Cavernous Malformations • Mostly single lesions • Multiple lesions may be familial and screening of family members may be indicated (familial multiple cavernous malformation syndrome) • Along with capillary telangiectasias, are commonly seen following cerebral radiotherapy • Mostly asymptomatic- or hemorrhage and seizures • Composed of a "mulberry-like" cluster of dilated thin-walled capillaries, with surrounding hemosiderin.(Unlike AVMs,there is no normal brain between the interstices of these lesions. ) • %80 supratentorial • Characteristic popcorn appearance in MRI • Symptomatic lesions should, when possible, be resected and complete resection is curative Cerebral Venous Angioma(DVA) • A congenital malformation of veins which drain normal brain • Most common cerebral vascular malformation • Characterised by the caput medusae sign(collection of dilated medullary veins converge in an enlarged transcortical or subependymal collector vein) in angiography. The appearance has also been likened to a palm tree • Usually incidental findings but patients can present with intracranial haemorrhage(1-5%) and also with ischaemic stroke and epilepsy. • Most common location: frontoparietal region (36-64%) • %75 solitory lesions but %20 of cases are associated with cavernous malformations and are referred to as mixed vascular malformations (MVM) References • Handbook of Neurosurgery (ebook), 7th Edition, by Mark S. Greenberg • https://radiopaedia.org/articles/vein-of-galen-aneurysmalmalformation-1 • http://www.dartmouth-hitchcock.org/cerebrovascular/veingalen-malformation-vog.html • http://emedicine.medscape.com/article/1162804-overview • https://www.medschool.lsuhsc.edu/neurosurgery/nervecente r/icvensyspin.html • https://www.ncbi.nlm.nih.gov/books/NBK27437/figure/A52/? report=objectonly