Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Brachytherapy wikipedia , lookup
Medical imaging wikipedia , lookup
Positron emission tomography wikipedia , lookup
Proton therapy wikipedia , lookup
Radiation therapy wikipedia , lookup
Center for Radiological Research wikipedia , lookup
Neutron capture therapy of cancer wikipedia , lookup
Backscatter X-ray wikipedia , lookup
Radiosurgery wikipedia , lookup
Nuclear medicine wikipedia , lookup
Industrial radiography wikipedia , lookup
Radiation burn wikipedia , lookup
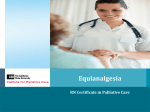
European Journal of Radiology 56 (2005) 413–417 Dose reduction in maxillofacial imaging using low dose Cone Beam CT Kostas Tsiklakis a,∗ , Catherine Donta a , Sophia Gavala a , Kety Karayianni a , Vasiliki Kamenopoulou b , Costas J. Hourdakis b a Department of Oral Diagnosis and Oral Radiology, School of Dentistry, University of Athens, Greece b Licensing and Inspection Division, Greek Atomic Energy Commission, Greece Received 14 January 2005; received in revised form 13 May 2005; accepted 18 May 2005 Abstract Objectives: (a) To measure the absorbed dose at certain anatomical sites of a RANDO phantom and to estimate the effective dose in radiographic imaging of the jaws using low dose Cone Beam computed tomography (CBCT) and (b) to compare the absorbed and the effective doses between thyroid and cervical spine shielding and non-shielding techniques. Study design: Thermoluminescent dosimeters (TLD-100) were placed at 14 sites in a RANDO phantom, using a Cone Beam CT device (Newtom, Model QR-DVT 9000, Verona, Italy). Dosimetry was carried out applying two techniques: in the first, there was no shielding device used while in the second one, a shielding device (EUREKA!, TRIX) was applied for protection of the thyroid gland and the cervical spine. Effective dose was estimated according to ICRP60 report (EICRP ). An additional estimation of the effective dose was accomplished including the doses of the salivary glands (ESAL ). A Wilcoxon Signed Ranks Test was used for statistical analysis. Results: In the non-shielding technique the absorbed doses ranged from 0.16 to 1.67 mGy, while 0.32 and 1.28 mGy were the doses to the thyroid and the cervical spine, respectively. The effective dose, EICRP , was 0.035 mSv and the ESAL was 0.064 mSv. In the shielding technique, the absorbed doses ranged from 0.09 to 1.64 mGy, while 0.18 and 0.95 mGy were the respective values for the thyroid and the cervical spine. The effective dose, EICRP , was 0.023 mSv and ESAL was 0.052 mSv. Conclusions: The use of CBCT for maxillofacial imaging results in a reduced absorbed and effective dose. The use of lead shielding leads to a further reduction of the absorbed doses of thyroid and cervical spine, as well as the effective dose. © 2005 Elsevier Ireland Ltd. All rights reserved. Keywords: Absorbed dose; Effective dose; Lead shielding; Low dose Cone Beam CT; Thyroid gland; Cervical spine; Maxillofacial imaging 1. Introduction In the last few years, computed tomography (CT) has become one of the most useful and significant examinations for the maxilla and mandible. Since implant treatment has become the preferred method in cases of partial or total edentulism, the use of CT has increased mainly due to its high diagnostic accuracy [1,2]. It has been well documented that CT produces reliable data that facilitate the assessment of bone dimensions (both height and width) and/or the localization of important anatomical landmarks such as the mandibular canal, the mental foramen, ∗ Corresponding author. Tel.: +30 210 7461179. E-mail address: [email protected] (K. Tsiklakis). 0720-048X/$ – see front matter © 2005 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.ejrad.2005.05.011 the nasopalatal duct and the maxillary sinus [3]. Presently, CT is being widely used for the examination of temporomandibular joint and sinus pathology, trauma in the maxillofacial region and, routinely, in oncology [1,4–7]. However, the increasing use of CT technique in dentistry carries the risk of patient overexposure to radiation, which must be one of the dentist’s greatest concerns [8]. It is critical that radiation exposure be reduced to a minimum without any loss of diagnostic information [9,10]. Eventually, exposure minimization is more important for children and young adults [11,12]. The development of Cone Beam CT (CBCT) reduces exposure by using lower radiation dose, compared to conventional CT [13,14]. Cone Beam CT utilizes a cone shaped X-ray beam instead of the collimated fan beam in the spiral and conventional CT [15]. 414 K. Tsiklakis et al. / European Journal of Radiology 56 (2005) 413–417 The purpose of this study was: (a) to measure the absorbed radiation dose at 14 anatomical sites in a RANDO phantom and to estimate the effective dose in the radiographic examination of the jaws using CBCT and (b) to compare the absorbed and the effective doses between thyroid and cervical spine shielding and non-shielding techniques. 2. Materials and methods Seventy-five thermoluminescent dosimeter chips (TLD100) fabricated by Harshaw Chemical Co., Solon, USA, in the form of lithium fluoride, were placed in an adult male tissue-equivalent RANDO human phantom (Alderson Research Laboratories, Stanford, CN, USA). Although RANDO phantom is designed for radiotherapy purposes, the differences in (µab /ρ) coefficient for tissue equivalent materials allow the use of this phantom in diagnostic radiology energies with an uncertainty (error estimation) less than 15% depending on the anatomical sites [16]. This is due to the differences between a cadaver head and the phantom in relation to soft/hard tissues between the tube and the measured organs [17]. Before radiation exposure, TLD dosimeters were calibrated in X-ray beams with qualities similar to those used in dental radiography. Thus, the relation between TLD signal and X-ray doses for such beam qualities was established and used for the estimation of tissue/organ doses in the phantom. In order to avoid contamination from dust, moisture or grease, the TLDs were placed in sealed polyethylene bags and fixed at the anatomical locations of the tissues/organs of interest. These anatomical locations were defined using the manufactured canals within the slices of the phantom. The tissues/organs in which the absorbed radiation dose was measured were: the brain, the eyes, the parotid and the submandibular salivary glands, the thyroid gland, the bone marrow of the mandible, the bone marrow of the cervical spine (second, fourth and sixth cervical vertebra), the stomach, the lungs, the breasts, the oesophagus and the skin. In each exposure, 25 dosimeters were used. The anatomical regions and the phantom level, where the TLDs were put, are shown in Table 1. Two TLDs were used to measure background radiation, which was estimated 0.4 nC. The lowest TLD signal used to provide dosimetric data was three times higher than background. Background values were subtracted from TLD readings. CBCT (Newtom Model QR-DVT 9000, Verona, Italy) was used with an automatic exposure depending on bone volume and density. The milliamperage was 3.4 mA, the tube rotation time was 72 s, the mean exposure time was 17 s, the tube voltage was kept constant at 110 kV and the total filtration was 8 mm Al. The parameters used for the phantom correspond to an average weight 45-year-old male. Two techniques were applied during the study, using the same parameters. They differed in that during the second technique a lead shield device (EUREKA!) fabricated by TRIX especially for Newtom, was applied for the protection of the thyroid gland and the cervical spine (Fig. 1). Additionally, the use of this device facilitates the stabilization of the head during the examination. This shield device is composed of a base structure, a chin support combined with a front lead protection, a pillow, two support stirrups and a back lead protection. The two support stirrups were fixed on the base structure. This assemblage was put on CT patient’s couch nearby the scanning area. The chin support and the lead protection were fixed after the placement of the phantom, since their level depends on the size of the head and neck. Each technique was repeated three times to ensure reliability. All TLDs were annealed before irradiation in a PTWTLDO oven, for 1 h at 400 ◦ C followed by 2 h at 100 ◦ C. After irradiation TLDs were annealed for 10 min at 100 ◦ C. The thermoluminescent reader was a Harshaw, Model 4500. The type of X-rays used for the calibration was RQR Narrow (according to ISO 4037-1, 1996), of different energies. The findings were assessed statistically using a Wilcoxon Signed Ranks Test. Table 1 Mean absorbed doses in mGy at pre-selected anatomical regions of the phantom for non-shielding and shielding techniques Anatomical region Phantom level Mean absorbed dose (mGy) non-shielding S.D. Mean absorbed dose (mGy) shielding S.D. p-Value Thyroid Bone marrow (mandible) Bone marrow (cervical spine second, fourth, sixth vertebra) Skin (zygomatic area) Lens of eyes Submandibular salivary glands Parotid salivary glands Brain Lung Breast Stomach Oesophagus 10 7 6, 7, 9 0.32 1.67 1.28 0.07 0.09 0.04 0.18 1.64 0.95 0.04 0.12 0.07 0.04* 0.88 0.04* 4 4 8 5 3 17 15 17 10 0.77 0.61 1.28 1.12 0.32 0 0 0 0.16 0.12 0.09 0.09 0.07 0.12 – – – 0.10 0.76 0.62 1.25 1.10 0.30 0 0 0 0.09 0.07 0.05 0.09 0.12 0.08 – – – 0.06 0.89 0.98 0.79 0.82 0.98 – – – 0.07 p-Value is demonstrated according to Wilcoxon Signed Ranks test. * p < 0.05. K. Tsiklakis et al. / European Journal of Radiology 56 (2005) 413–417 415 calculated as: Average salivary gland dose × 0.025 + remainder (brain) / 10 × 0.025 [22]. 3. Results Fig. 1. RANDO phantom with thyroid and cervical spine shielding placed in Cone Beam CT device. Effective dose, EICRP , has been estimated, according to the ICRP60 [18]. The tissues/organs considered to contribute to the effective dose were the thyroid, the bone marrow, the oesophagus, the bone surface and the skin. The contribution of the whole body active bone marrow was estimated as 0.8% for the mandible and 3.9% for the cervical spine. These proportions depend on the age and gender and correspond to 40-year-old male [19]. Likewise, concerning the fractional contribution of the skin it was calculated that only 5% of the skin was present in the primary beam [22]. The bone surface was estimated, according to Frederiksen et al., by multiplying the mean absorbed dose of the bone marrow with a factor of 4.64, which is the ratio of f-factors (the factors of conversion of exposure to absorbed dose) for bone and soft tissue [20]. The respective proportions of the mandible and cervical spine in relation to the whole body bone surface are 1.33% [21] and 1.4% [20]. In our study, absorbed doses were measured also in the submandibular and the parotid salivary glands. These tissues are not referred to as “remainder” in the ICRP60 report, because they are not radiosensitive enough in order to contribute to the effective dose [18]. Nevertheless, in our study the salivary glands were considered as “remainder”, since the doses, which were received by these organs were high in order of magnitude as the other radiosensitive tissues. In this way there is an overestimation of the effective dose. Since the salivary glands are not included in the ICRP60 list of individually weighted tissues or remainder organs, an additional calculation of effective dose has been performed [8,22]. Particularly, ESAL was calculated as EICRP with an addition of the salivary glands as part of the remainder organs. Since the absorbed doses of the salivary glands were found among the highest of the measured weighted organs, a weighting factor of 0.025 should be applied to the average dose of the salivary glands and a weighting factor of 0.025 to the average dose of the 10 remainder organs and was Table 1 shows the mean organ dose (left and right) (D), the standard deviation (S.D.) and the p-value for the statistical analysis in the non-shielding and the shielding techniques. In the non-shielding technique, the doses ranged from 0.16 mGy in oesophagus to 1.67 mGy in bone marrow of the mandible. It is noteworthy that the absorbed doses of bone marrow of the mandible, bone marrow of the cervical spine and salivary glands are the highest among the tissues of interest. In the shielding technique the absorbed radiation doses ranged from 0.09 mGy in oesophagus to 1.64 mGy in the bone marrow of the mandible. It is obvious that radiation doses of bone marrow of the mandible and salivary glands are the highest among the tissues of interest. The other organs (stomach, lungs and breasts), which are not included in Table 1, received no dose or negligible dose, which was accepted as zero, in both shielding and nonshielding technique. In the non-shielding technique, the thyroid gland received 0.32 mGy, while in the shielding technique the respective value was 0.18 mGy. Additionally, the cervical spine received 1.28 mGy as an average of the three vertebrae in the non-shielding technique and 0.95 mGy in the shielding technique. The p-value for both thyroid and cervical spine absorbed doses was 0.04, statistically significant (p < 0.05). In contrast, there was no statistically significant difference (p > 0.05) between the two techniques in the doses received by the other organs (Table 1). Table 2 shows the effective dose calculations according to ICRP60 [18]. In the non-shielding technique, the EICRP value was 0.035 mSv. Adding the average dose of the salivary glands in the remainder organs, the ESAL value was 0.064 mSv. Furthermore the EICRP value in the shielding technique was 0.023 mSv and the ESAL was 0.052 mSv. 4. Discussion In this study, using CBCT, the average absorbed radiation doses have been estimated at certain anatomical areas of the head, neck and upper body of a RANDO Alderson phantom. The findings have shown that the absorbed doses were low compared to the doses received during a conventional CT [23,24]. High-resolution CT can provide diagnostic information about bone structure and soft tissues as well. Additionally, there are CT dose reduction protocols by using lower mA and increasing pitch. The dose reduction leads to an image noise increase, which results to a lower image quality [6,10]. In this study, the bone marrow in the body of the mandible at molar area and in the cervical spine, as well as the salivary glands, received the highest doses bilaterally, probably 416 K. Tsiklakis et al. / European Journal of Radiology 56 (2005) 413–417 Table 2 Effective dose according to ICRP Publication 60 guidelines (EICRP ) and including salivary glands as remainder organs (ESAL ) Anatomical region Weighting factor (WT ) Percentage irradiated (%) Effective dose (mSv) non-shielding Effective dose (mSv) shielding Thyroid Bone marrow (mandible) Bone marrow (cervical spine) Skin Oesophagus Bone surface (mandible) Bone surface (cervical spine) Remainder (brain) Total EICRP 0.05 0.12 0.12 0.01 0.05 0.01 0.01 0.050 100 0.8 3.9 5 100 1.33 1.4 100 0.016 0.001 0.006 0 0.008 0.001 0.001 0.002 0.035 0.009 0.001 0.005 0 0.005 0.001 0.001 0.001 0.023 Remainder (brain) Remainder (salivary glands) Total ESAL 0.025 0.025 100 100 0.001 0.030 0.064 0.001 0.029 0.052 because these areas are directly irradiated by the X-ray beam. The findings resulting from the study are in agreement with other investigations, which have identified the highest absorbed radiation doses in these areas [10,15,22,24]. Contrary, the thyroid gland and the eyes received the lowest radiation dose during tomography, probably because these areas are located out of the primary beam. The irradiation of organs outside the primary beam is mainly due to X-rays scattered within the patient. Additionally, the extension of the scout view caudally, beyond the mandibular symphysis, contributes to the total thyroid dose by doubling it [11]. If the region under examination lies in the trunk, the shape of the patient makes it difficult to shield adjacent organs from this scattered radiation [11]. Therefore, we considered that the shielding of radiosensitive organs, wherever possible, would improve patient protection, since it leads to an overall dose reduction. At this point, it is important to mention that, using the shielding, there was no difference in the image quality and no artifacts were observed, since the shielding device was placed out of the irradiation beam. We evaluated the two techniques and a statistically significant difference was found between the values of the absorbed doses received by the thyroid gland and the cervical spine (p < 0.05). Specifically, the absorbed doses measured at these organs in the shielding technique have been proved to be lower than the respective values in the non-shielding technique (Table 1). Contrary, comparing the absorbed doses received by the other organs and tissues examined, no statistically significant difference was found between the two techniques (p > 0.05) (Table 1). Although the doses were low, it is our responsibility to assure that the patients do not receive any unnecessary dose of radiation, especially in the thyroid gland of the young individuals. It is noteworthy that in many cases the use of thyroid shielding may lead to a dose reduction by one half [25,26]. Concerning the salivary glands absorbed radiation doses, the authors’ argument is about including these glands in the remainder organ calculations [22]. This is considered as being consistent with the ICRP60 position that other tissues or organs either selectively irradiated or later identified as having a significant risk of induced cancer will be included either with a specific weighting factor or in the list constituting remainder organs [18]. It has been suggested that the lymphoid component may be more susceptible to low dose radiation damage than the parenchyma of the salivary glands [27]. As it concerns the calculation of the effective dose (E), the authors estimated E according to the ICRP60 report, but they also used the salivary glands as remainder organs, because the reported probability of fatal cancer induction in the salivary glands is of the order of 5 × 10−4 Sv−1 [22]; thus, this probability is equal to the likelihood of cancer induction from irradiation of the bone surface, which is included as a weighted organ in ICRP60 effective dose calculations. Other investigators have reached the same conclusions concerning our point in achieving low radiation dose during radiographic examination using CBCT. In one study, the authors estimated the effective dose using CBCT and the E value, which was calculated for the central dose profile, ranged from 0.05 to 0.06 mSv [15]. In a recent study, while accomplishing a maxilla/mandible scan using CBCT, the EICRP value was 0.04 mSv and the ESAL was 0.08 mSv [22]. Using new software in the same study, the EICRP was 0.04 mSv and the ESAL was 0.09 mSv [22]. The purpose of using a new version of software was to increase the signal-to-noise ratio. The thyroid and the cervical spine absorbed doses were found 0.37 and 1.45 mGy, respectively. Using new software, the thyroid and the cervical spine absorbed doses were 0.44 and 1.73 mGy, respectively [22]. The variability of the results of these studies can be explained as the interaction of many factors. Inexact vertical positioning of the TLDs inside the phantom may influence the results [22]. Variation in the accuracy of TLDs and the TLD reader also contribute to interexamination variation [22]. Generally, from the stand point of radiation risk, CBCT in maxillofacial imaging produces 8- to 10-fold lower effective dose than a conventional CT examination using standard protocol [6,8,20]. If a low dose protocol is used for conventional CT, the effective dose may be reduced with an increase of image noise [15]. According to published effective doses K. Tsiklakis et al. / European Journal of Radiology 56 (2005) 413–417 from panoramic radiography, CBCT appears to have a three to seven times higher risk compared to a panoramic examination. These results depend on the absorbed radiation doses at certain anatomical areas, the degree of collimation and the acquisition software version [17,28,29]. In conclusion, the absorbed radiation doses and the effective doses with and without the salivary glands using CBCT could be considered low. Additionally, the use of lead shielding leads to a further reduction of the absorbed doses of thyroid and cervical spine, as well as the effective dose. References [1] Arai Y, Tammisalo E, Iwai K, Hashimoto K, Shinoda K. Development of a compact computed tomographic apparatus for dental use. Dentomaxillofac Radiol 1999;4:245–8. [2] Ekestubbe A, Gröndahl K, Gröndahl HG. The use of tomography for dental implant planning. Dentomaxillofac Radiol 1997;26:206–13. [3] Diederichs CG, Engelke WGH, Richter B, Hermann KP, Oestmann JW. Must radiation dose for CT of the maxilla and mandible be higher than that for conventional panoramic radiography? AJNR 1996;17:1758–60. [4] Ziegler CM, Woertche R, Brief J, Hassfeld S. Clinical indications for digital volume tomography in oral and maxillofacial surgery. Dentomaxillofac Radiol 2002;31:126–30. [5] Solar P, Gahleitner A. Dental CT in the planning of surgical procedures. Radiologe 1999;39:1051–63. [6] Dula K, Mini R, Van der Stelt PF, Buser D. The radiographic assessment of implant patients: decision-making criteria. Int J Oral Maxillofac Implants 2001;16:80–9. [7] Parks ET. Computed tomography applications for dentistry. Dent Clin North Am 2000;44:371–94. [8] Lecomber AR, Yoneyama Y, Lovelock DJ, Hosoi T, Adams AM. Comparison of patient dose from imaging protocols for dental implant planning using conventional radiography and computed tomography. Dentomaxillofac Radiol 2001;30:255–9. [9] Ekestubbe A, Thilander A, Gröndahl K, Gröndahl HG. Absorbed doses from computed tomography for dental implant surgery: comparison with conventional tomography. Dentomaxillofac Radiol 1993;22:13–7. [10] Cohnen M, Kemper J, Möbes O, Pawelzik J, Mödder M. Radiation dose in dental radiology. Eur Radiol 2002;12(3):634–7. [11] Beaconsfield T, Nicholson R, Thorton A, Al-Kutoubi A. Would thyroid and breast shielding be beneficial in CT of the head? Eur Radiol 1998;8:664–7. [12] Tsiklakis K, Donta-Bakoyanni C, Tassopoulou M, Kamenopoulou V. Absorbed radiation dose during lateral cephalometric radiography: comparison of screen-film systems and field-size combinations. J Clin Pediatr 2000;24:117–21. 417 [13] Siwerdsen JH, Jaffray DA. Cone-beam computed tomography with a flat-panel imager. Med Phys 1999;26:2635–47. [14] Tam KC, Samarasekeva S, Somer F. Exact cone beam CT with a spiral scan. Phys Med Biol 1998;43:1015–24. [15] Mozzo P, Procacci C, Tacconi A, Martini PT, Andreis IA. A new volumetric CT machine for dental imaging based on the cone-beam technique: pleliminary results. Eur Radiol 1998;8:1558–64. [16] Shrimpton PC, Wall BF, Fisher ES. The tissue-equivalence of the Alderson Rando anthropomorphic phantom for X-rays of diagnostic qualities. Phys Med Biol 1981;26(1):133–9. [17] Bou-Serhal C, Jacobs R, Gijbels F, et al. Absorbed doses from spiral CT and conventional spiral tomography: a phantom vs. cadaver study. Clin Oral Impl Res 2001;12:473–8. [18] ICRP Publication 60. Radiation protection. Recommendations of the International Commission on Radiological Protection. Pergamon Press; 1990. p. 68. [19] Cristy M. Active bone marrow distribution as a function of age in humans. Phys Med Biol 1981;26(3):389–400. [20] Frederiksen NL, Benson BW, Sokolowski TW. Effective dose and risk assessment from computed tomography of the maxillofacial complex. Dentomaxillofac Radiol 1995;24:55–8. [21] Pickering PT, Howden R. The surface form of the skull. Gray’s anatomy, descriptive and surgical. Philadelphia: Running Press; 1974. p. 118–22. [22] Ludlow JB, Davies-Ludlow LE, Brooks SL. Dosimetry of two extraoral direct digital imaging devices: Newtom cone beam CT and Orthophos Plus PS panoramic unit. Dentomaxillofac Radiol 2003;32:229–34. [23] Velders XL, Van der Stelt PF. Absorbed dose to the parotid glands: spiral CT versus conventional tomographic examinations. In: Farman AG, Ruprecht A, Gibbs SI, Scarfe WC, editors. Advances in maxillofacial imaging. Amsterdam: Elsevier Science B.V.; 1997. p. 407–12. [24] Christiansen EL, Moore RJ, Thompson JR, Hasso AN, Hinshaw Jr DB. Radiation dose in radiography, CT and arthrography of the temporomandibular joint. AJR Am J Roengenol 1987;148:107–9. [25] White SC, Pharoah MJ. Principles and interpretation. Oral radiology. 4th ed. St. Louis Mosby Co.; 2000. p. 48. [26] Bianchi J, Goggins W, Rudolph M. In vivo, thyroid and lens surface dose with spiral and conventional computed tomography in dental implant radiography. Oral Surg Oral Med Oral Path Oral Radiol Endod 2000;90:249–53. [27] Auclair PL, Ellis GL, Gnepp DR, Wenig BM, Janney CG. Salivary gland neoplasms: general considerations. In: Ellis GL, Auclair PL, Gnepp DR, editors. Surgical pathology of the salivary glands. Philadelphia: W.B. Saunders; 1991. p. 135–64. [28] White SC, Rose TC. Absorbed bone marrow dose in certain dental radiographic techniques. J Am Dent Assoc 1979;98:553–8. [29] Bou-Serhal C, Van Steenberghe D, Bosmans H, Sanderick GCH, Quivynen M, Jacobs R. Organ radiation dose assessment for conventional spiral tomography: a human cadaver study. Clin Oral Impl Res 2001;12:85–90.