Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
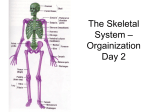
Textbook Topic Lab Manual Chapter 7 The Axial Skeleton Exercise 9 Chapter 8 The Appendicular Skeleton Exercise 10 Chapter 9 Articulations (Joints) Exercise 11 The Skull: Bones to Know Cranial Bones Facial Bones • Frontal bone • Palatine bones (2) • Parietal bones (2) • Zygomatic bones (2) • Occipital bone • Lacrimal bones (2) • Temporal bones (2) • Nasal bones (2) • Auditory ossicles (6): • Vomer bone malleus, incus, stapes • Maxillae (2) • Sphenoid bone • Inferior nasal conchae (2) • Ethmoid bone • Mandible Other axial bones to know • Vertebrae • Ribs • C1 to C7 • True (vertebrosternal) • C1: atlas • False • C2: axis • vertebrochondral • C7: vertebra prominens • vertebral (floating) • T1 to T12 • L1 to L5 • Sacrum • Coccyx Focus on structures unless lecture covered function as well. Other axial features to know: • Foramen magnum • Hard palate • Infraorbital foramen • Mastoid process • Mental foramen A final note on the axial skeleton • Lab manual, page 133: “The spinal cord ends at the superior edge of L2, but the outer covering of the cord, filled with cerebrospinal fluid, extends an appreciable distance beyond.” How might this info be useful clinically? 1. Lumbar puncture: get CSF to see about infection (meningitis) 2. Anaesthesia: straight into CSF (vs. epidural) L3-L4 is safer (avoids spinal cord) Transition between axial & appendicular Lab manual, Figure 10.6a skeleton: the pelvis! (again: sacrum & coccyx is axial; everything else = hip bones = pelvic girdle = coxal bones) Ilium, ischium, pubis, pubic symphysis, iliac crest. Know these! Male Pelvis versus Female Pelvis • What are the female’s unique “needs”? • Give birth! • Carry fetus while growing! Lab manual, Table 10.1 Anterior: Pubic arch (large angle in female), pelvic brim wider, more flared pelvic girdle (smaller acetatabula – smaller bones) From left side: More posterior coccyx Wider pelvic outlet, less protrusion of coccyx Tangent: How do males and females develop differently? (How do genetic differences lead to physiological differences?) Less-than-perfect accuracy: • Complex traits are not coded for by single genes (or clusters of genes in one area) • Male chromosome is not just a chromosome missing “girl genes” • Each chromosome stores hundreds to thousands of genes (in reality) • http://ivebecomemyparents.com/2011/09/18/ Testis-Determining Factor (TDF) immature gonad Y chromosome containing TDF gene Turns on expression of other genes that cause gonad to develop as testes Testes make testosterone Testosterone leads to male traits (such as male pelvis) Note: Y chromosome with mutated TDF => female! (beware, Olympic judges! No Y chromosome (no TDF gene) Gonad develops into ovaries Ovaries produce (mostly) estrogen, progesterone => “female” traits Bone projections revisited (textbook Chapter 6, lab manual Exercise 8) • 2 basic functions of projections? - Surfaces for muscle/ligament attachment - Help form joints (articulations) Vertebra: note “levers” where muscles attach! Lab manual: Review Sheet 9 and Figure 10.7 Appendicular Skeleton • Components that you need to know: • Pectoral girdle: clavicle, scapula • Upper limb: humerus, radius, ulna, carpals (8), metacarpals (5), phalanges (3 per digit except thumb) • Pelvic girdle: see previous slide: pubis, ilium, ischium • Lower limb: femur, petalla, tibia, fibula, tarsals (7: talus, calcaneus – know these specifically!), metatarsals, phalanges Other appendicular structures/markings to know • Acromion • Anterior border of tibia • Iliac crest • Lateral malleolus • Medial malleolus • Olecranon • Pubic arch • Pubic symphysis Bones of the arm and leg Bones of the arm and leg, from proximal to distal: Sing along with Doctor Greg, and shoot ‘em off like a pistol! An arm has 1 humerus, 1 ulna, and, thicker toward the wrist, 1 radius; 8 carpals, 5 metacarpals, 14 phalanges (these are not the weightiest!). Bones of the arm and leg, from proximal to distal: Sing along with Doctor Greg, and shoot ‘em off like a pistol! A leg has 1 femur, 1 patella, 1 fibula, and 1 larger tibia; 7 tarsals, 5 metatarsals, 14 phalanges (I’m not ribbin’ ya!). Bones of the arm and leg, from proximal to distal: Sing along with Doctor Greg, and shoot ‘em off like a pistol! [Bang!] Bones of the Arm and Leg Melody playback: http://www.noteflight.com/scores/view/f72a6c039c165051b09a049368bdf66e3f5fab2f Skeleton Worksheet What was hard here? Tibia/fibula Ischium Metatarsals vs. phalanges Articulations … also known as Joints (textbook Chapter 9 / lab manual Exercise 11) Why are joints useful? Flexibility – some parts of skeleton need to move relative to other parts. Independence – good to have some parts of skeleton isolated from others, at least partly. Developmentally, good to have separate bones (?) that can grow together. STRUCTURAL Classification of Joints • Cartilaginous: contain (fibro)cartilage! • Fibrous: contain fibrous (collagen-rich) material (e.g., ligament) • Synovial: see below! (contain synovial fluid in cavities) Recall Figure 4-16d from 10th Martini (type of tissue membranes): Hyaline cartilage Synovial fluid Capsule Capillary Adipocytes Areolar connective tissue Synovial membrane Epithelial cells (simple squamous) STRUCTURAL Classification of Joints: Cartilaginous, Fibrous, or Synovial? Elbow = synovial sternum = cartilaginous fibrous Intervertebral discs and pubic symph. = (fibro)cartilaginous Lab manual, Figure 11.1 synovial fibrous FUNCTIONAL Classification of joints (How much can they move?) • Synarthroses: can’t move! • Cartilaginous, Fibrous • Amphiarthroses: can move a little! • Cartilaginous, Fibrous • Diarthroses: can move more than a little! • All synovial joints are here! Simple Model of Joint Motion 10th Martini: Figure 9-2 angular linear rotation circumduction Joint Movement: 3 Axes of Motion Not all joints can move in all 3 axes, though….. 10th Martini: Figure 9-2 Classification of Synovial Joints Ball and socket: 3! Saddle: 2 Hinge: 1 Pivot: 1 10th Martini: Figure 9-2 Condylar: 2 Gliding/Plane: 0-2 (but not much movement) Animations of movement: http://faculty.stcc.edu/AandP/AP/AP1pages/Units5to9/joints/synovial.htm What are the differences? • Condylar versus Ball-and-Socket: • Condylar versus Saddle: Name that joint type! (HIP) Ball & socket Saddle joint (not synovial) Cartilaginous Synovial joints’ accessory structures 10th Martini: Figure 9-1b Tendon: joins bone to muscle Bursa: lubricating body (fluid-filled) Fat pad Meniscus: (C-shaped) fibrocartilage, lateral & meniscus) Extracapsular ligament (patellar) Intracapsular ligament (cruciate) (Anterior & Posterior) Synovial joint trade-off: mobility versus stability • What can make joints more stable (but less mobile?) • Cartilaginous or fibrous (not synovial) • Numerous and/or strong ligaments • Presence of other nearby bones, tendons, fat pads stabilizes/restricts the motion • Deep sockets (hip, vs. shoulder, which is shallow) • Thickness/strength of synovial capsule • Joint problems (from lab manual + textbook) Name Problem Treatment Sprain Tearing/stretching ligament (and tendon?) RICE (Rest*, Ice, Compression, Elevation) / MICE Bone out of place Put it back! (have a pro do this) Dislocation Wear and tear, loss of Osteoarthritis cartilage protecting bones Arthritis = joint Rheumatoid arthritis inflam mation Gouty arthritis Autoimmune – joints are attacked by immune system Crystals (of uric acid) build up in synovial fluid Anti-inflammatory meds; Joint replacement surgery (e.g, James’ femuracetabulum problem … steel ball into steel cup!) Exercise??? (see next slide) Worksheet: Exercise for arthritis? • Reasons against? • Don’t want to make inflammation worse. • Reasons for? • Don’t sit and get rusty like an old car! (Use it or lose it!) Muscles will lose fitness, etc. • Stimulate more blood flow to damaged area. • Can still exercise without stressing the joint much (e.g., swimming). • Keep weight down to reduce stress on weight-bearing joints. Bulging disc vs. herniated disc? (worksheet) • (Clinical Case from Martini textbook) • Hernia = protrusion outside of normal area; here, nucleus pulposus penetrates annulus fibrosis (harder outer covering) • Bulging disc = no rupture • BOTH can impinge upon nerves (pain, numbness, etc.) • most often a problem at lumbar level • POSTERIOR protrusions will affect spinal nerves Synovial joints: Triaxial, Biaxial, Monoaxial, or Nonaxial Students rap the red underlined words. Tri, bi, mono, non! How many axes of movement are in this joint? Tri, bi, mono, non! Synovial classification is this song’s point! There’s pivot, hinge, and plane: their movement’s quite constrained! There’s condylar and saddle: two axes now are straddled! And last, there’s ball and socket: three axes in its pocket! Whoa-oh-oh-oh... Three, two, one, zero! Tri, bi, mono, non! How many axes of movement are in this joint? Tri, bi, mono, non! Synovial classification is this song’s point! It’s this song’s point! [etc.] Melody playback: http://www.noteflight.com/scores/view/7f332978abe76d46b31078f06a6718f66270b152 Lab Exercise 11: key points • Reasons for relative stability of hip, knee, and shoulder joints (see Review Sheet) • Movements: • flexion/extension • abduction/adduction • rotation vs. circumduction • pronation/supination • dorsiflexion/plantar flexion • inversion/eversion Lab Exercise 11: key points (continued) • Joint names to recognize (most should be straightforward) • Temporomandibular • Intercarpal • Atlantooccipital • Carpometacarpal • Atlantoaxial • Metacarpophalangeal • Intervertebral • Interphalangeal • Costovertebral • Sacroiliac • Sternoclavicular • Tibiofemoral • Sternocostal • Femoropatellar • Acromioclavicular • Tibiofibular (superior and inferior) • Glenohumeral • Intertarsal • Tarsometatarsal • Metatarsophalangeal • Radioulnar (proximal and distal)