Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Coronary artery disease wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Cardiac surgery wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
DiGeorge syndrome wikipedia , lookup
Marfan syndrome wikipedia , lookup
Williams syndrome wikipedia , lookup
Turner syndrome wikipedia , lookup
Electrocardiography wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Heart arrhythmia wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
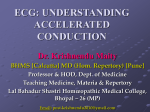
Europace (2005) 7, 28e33 REVIEW ARTICLE Early history of the pre-excitation syndrome Sam Hanon, Michael Shapiro, Paul Schweitzer) Submitted 16 July 2003, and accepted after revision 15 September 2004 KEYWORDS WPW syndrome; pre-excitation syndrome; early history; accessory connections Abstract This brief review discusses the interesting early history of the preexcitation syndrome. In 1913 Cohn and Fraser published the first patient with a short P-R interval, wide QRS complexes, and paroxysmal tachycardia. This was followed by other cases of pre-excitation syndrome, all of which were considered to be due to bundle branch blocks. In 1930 Wolff, Parkinson, and White reported 11 patients with the syndrome, which came to bear their name. Two years later, Holzmann and Scherf suggested bypass tracts as the most likely mechanism of preexcitation syndrome. In 1942, Wood et al. documented the first accessory connection at autopsy. Despite these early studies supporting the bypass theory, the quest for alternative mechanisms continued until the 1970s when electrophysiological studies and surgical therapy confirmed accessory connections as the mechanism of pre-excitation syndrome. ª 2004 The European Society of Cardiology. Published by Elsevier Ltd. All rights reserved. Introduction Pre-excitation syndrome has an interesting and remarkable history. Early descriptions of this phenomenon date back more than 80 years to the first isolated cases reported by Wilson [1], Wedd [2], and Hamburger [3]. The more comprehensive description by Wolff, Parkinson, and White in 1930 brought this syndrome to prominence. Wolff and coworkers [4] reported 11 mostly young, healthy ) Corresponding author. Tel.: C1 212 420 2416; fax: C1 212 420 2406. E-mail address: [email protected] (P. Schweitzer). subjects with a short P-R interval, wide QRS complexes, and paroxysms of tachycardia. This pattern, which later came to be known as the WolffeParkinsoneWhite (WPW) syndrome, was the first characterized pre-excitation syndrome. In 1944, Ohnell [5] introduced the term preexcitation syndrome for an electrocardiogram (ECG) manifested by a short P-R interval and a wide QRS complex, regardless of the presence or absence of tachycardia. That same year, Segers and coworkers proposed the term delta wave for the initial slurred component of the QRS complex [6]. The aim of this review is to discuss some of the notable historical aspects of pre-excitation 1099-5129/$30 ª 2004 The European Society of Cardiology. Published by Elsevier Ltd. All rights reserved. doi:10.1016/j.eupc.2004.09.005 Downloaded from http://europace.oxfordjournals.org/ by guest on April 16, 2014 The Heart Institute, Beth Israel Medical Center, University Hospital and Manhattan Campus for the Albert Einstein College of Medicine, Department of Cardiology, 1st Avenue at 16th Street, Dazian Building, 11th Floor, NY 10003, USA Early history of the pre-excitation syndrome syndrome, specifically the early misconceptions regarding the basis of the electrocardiographic abnormalities and arrhythmias associated with this condition [1,2,7,8]. Early reports of pre-excitation syndrome Anatomical substrate of pre-excitation syndrome Kent dramatically advanced the understanding of intracardiac conduction with his study of auriculoventricular (A-V) muscular connections. Kent proposed that there were multiple muscular links, which crossed the A-V groove. Specifically, he focused attention on a muscular connection between the right auricle and right ventricle at the lateral right border of the heart [9]. Thomas Lewis, who in 1925 did not find adequate anatomical or physiological evidence to support this hypothesis [10], questioned the role of ‘‘Kent’s bundle’’ in A-V conduction. Despite this scepticism, the notion that these bundles might play a role in A-V conduction continued to be studied [11,12]. Fifty years after Kent’s first work on the subject was published, Mahaim stated, ‘‘If conduction by Kent’s fibres is accepted (and it has still not been proved that these fibres regularly exist, and one can even doubt it), it should be regarded as an accessory form of conduction: para-specific conduction’’ [13]. A significant development occurred in 1942 when Wood and coworkers [14] reported the first histological proof of muscular connections between the right auricle and the right ventricle in a human autopsy specimen. The patient was a 16year-old boy with episodes of paroxysmal tachycardia. Three years after the initial presentation, he presented with palpitations, severe substernal distress, and a heart rate over 150 beats per minute (bpm). The patient died 2 h later after drinking cold water. Autopsy revealed a normal heart with three muscular A-V connections between the right atrium and ventricle. In the subsequent years, accessory connections were documented in series of patients with preexcitation syndromes [15e18]. Despite these findings, Lev [15] in 1966 stated, ‘‘the anatomical base of the WPW syndrome is today unknown’’ and seven years later, ‘‘one must not overlook, however, the concept of Sherf and James of a physiological bypass within the conduction system’’ [16]. In other words, according to Lev, accessory connections were not the only means of pre-excitation. The mechanism of pre-excitation syndrome Interestingly, two groups working independently in the early 1930s proposed that the muscular connections described by Kent might be used to conduct an auricular impulse to the ventricle. Holzmann and Scherf [11], in 1932, were the first Figure 1 Rhythm strip showing three pre-excited beats followed by a ventricular premature, which initiates a run of narrow complex tachycardia (from Cohn and Fraser [7] with permission). Downloaded from http://europace.oxfordjournals.org/ by guest on April 16, 2014 Cohn and Fraser [7] in essence reported the first case of pre-excitation syndrome in 1913. These authors presented two patients with paroxysmal tachycardia, terminated by vagal stimulation. In the first patient, the resting ECG showed right bundle branch block (RBBB) and the second patient’s ECG revealed a slurring of the initial portion of the QRS complex (Fig. 1). In 1915, Wilson [1] published a patient with pre-excitation and episodes of supraventricular tachycardia, which were terminated by the Valsalva manoeuver. This patient also had spontaneous and atropine induced AV junctional rhythm. These two reports [1,7] were followed by additional cases of pre-excitation syndrome in 1921 and 1926, all of which were classified as bundle branch block (BBB) [2,8]. 29 30 Figure 2 Early, accurate hypothesis on the mechanism of pre-excitation (from Wolferth and Wood [12] with permission). Holzmann and Scherf, in addition to their pioneering theory on the mechanism of pre-excitation, also discussed the possibility of an ‘‘excitable centre’’ [11]. A properly timed atrial contraction could initiate a ventricular impulse from an excitable ventricular centre, thereby causing a short P-R interval and a delta wave. Sodi-Palares offered a similar mechanism in which electrotonus from the depolarized atrium triggers a ventricular impulse [20]. Further, according to Prinzmetal et al., a short P-R interval and a delta wave could be due to an accelerated atrial impulse stimulating the summit of the intraventricular septum [21]. The initial slurring of the QRS complex during stimulation of the intraventricular septum in patients undergoing right heart catheterization supported this concept [22]. Finally Sherf and James developed the ‘‘synchronized sino-ventricular conduction’’ theory [23]. According to these authors, an impulse originating in the posterior intranodal bundle preferentially activates the ventricle and causes pre-excitation. Substantial support for the accessory pathway theorists arrived in 1942 when Butterworth and Poindexter published the first experimental animal study using an ‘‘electric bypass between the atrium and ventricle’’ [24]. The investigators were able experimentally to generate tracings similar to the previously described WPW syndrome. Thus, A-V bypass tracts as the mechanism of pre-excitation was not generally accepted until the 1970s. A major advance was achieved when Durrer and Roos performed epicardial excitation mapping on a patient with the WPW syndrome [25]. Mapping was performed on a 21-year-old woman during surgery for a large atrial septal defect. The right ventricle was activated earliest as a result of conduction of the atrial impulse through a connection near the right lateral atrioventricular sulcus. This finding laid the foundation for later invasive electrophysiological studies [26e29], which not only clarified the underlying abnormality but also confirmed reentry as the mechanism of paroxysmal tachycardias in the WPW syndrome. These studies also became the basis for the surgical and catheter ablation therapy of the pre-excitation syndrome. It is most likely that James, in 1976, more than 80 years after Kent’s original publications, wrote the last article challenging accessory connection as the mechanism of pre-excitation syndrome [30]. Another interesting aspect of the history of preexcitation syndrome is the role of accessory connections within the specialized conduction system (nodoventricular, nodofascicular, and fasciculoventricular connections). According to Ferrer, Downloaded from http://europace.oxfordjournals.org/ by guest on April 16, 2014 to publish this theory. They expounded on the likelihood that an accessory A-V connection was the most likely mechanism of pre-excitation in the syndrome described by Wolff, Parkinson, and White. Wolferth and Wood [12], whose article was in press at the time of the Holzmann and Scherf publication, also put forward this theory and further, speculated that the electrocardiographic findings were due to conduction over the ‘‘bundle of Kent’’ as well as the bundle of His (Fig. 2). Wolferth and Wood further detailed the abnormal ECG features of this syndrome. They pointed out that the interval from the beginning of the P wave to the end of the QRS was within normal limits. Thus, though the P-R interval was shortened, the QRS was widened to a degree that allows the total P-QRS segment to remain of normal duration. Moreover, if the P-R lengthens, the QRS can be expected to shorten to the same extent. For this reason, the authors disputed the idea that the QRS abnormality represented a bundle branch block. They stated that ‘‘the abnormality of the QRS complex consists, not of a block or delay, but of an actual early arrival in the ventricular muscle of the impulse from the auricle’’ [12]. Despite anatomical and electrophysiological evidence of accessory connections, search for alternative mechanisms continued. In 1964, Scherf and Cohen [19] reviewed the literature and found more than 60 possible mechanisms of pre-excitation ‘‘most of [which] have no support and some are fantastic’’. In addition to the BBB mechanism initially suspected by Wolff, Parkinson, and White and challenged from the beginning, the more common suggestions were the ‘‘excitable centre’’ theory and the concept of accelerated conduction [19]. S. Hanon et al. Early history of the pre-excitation syndrome WPW syndrome could either be due to a Kent bundle or a combination of James’ posterior intranodal tract with Mahaim fibres [31]. Lev et al. documented this combination in a patient with pre-excitation syndrome who subsequently developed complete A-V block [32]. The role of the Mahaim fibres was also considered in patients with accessory pathways and decremental conduction properties. However, electrophysiological studies and surgical results in the 1980s and 1990s challenged the participation of Mahaim fibres in the pre-excitation syndrome [33,34]. Wide QRS complex tachycardia in WolffeParkinsoneWhite syndrome case was of a 4-year-old boy with palpitations and difficulty breathing. The electrocardiogram revealed paroxysms of wide QRS complex tachycardia with a short P-R interval. Dr. Hamburger made a presumptive diagnosis of auricular tachycardia with right bundle branch block due to a respiratory infection [3]. In 1941, Levine and Beeson reported three patients with paroxysms of tachycardia classified by the authors as ‘‘ventricular tachycardia’’ [35]. All of their patients had pre-excitation and irregular wide QRS complex tachycardia, most likely due to atrial fibrillation. The most notable patient was a 36-year-old steamfitter who ‘‘while lifting a heavy box, suddenly became conscious of a ‘‘knock’’ in the centre of his chest’’. The initial ECG showed ‘‘ventricular tachycardia,’’ which was treated with 0.8 mg of oral digitalis (Fig. 3). After restoration of sinus rhythm the ECG showed a short P-R interval and bundle branch block, with an infarct pattern. The patient was hospitalized for six weeks with the diagnosis of acute myocardial infarction. However, according to Levine, who saw the patient two months later, the diagnosis of Figure 3 Four leads showing irregular rhythm with wide and narrow QRS complexes classified as ‘‘ventricular tachycardia’’ and inferior pseudoinfarct (from Levine and Beeson [35] with permission). Downloaded from http://europace.oxfordjournals.org/ by guest on April 16, 2014 Studies have repeatedly shown that wide QRS tachycardias are seen in patients with the WPW syndrome. Early reports diagnosed these rhythms as ventricular tachycardia. In 1929, Hamburger reviewed four cases of ‘‘Intraventricular block showing some interesting and unusual features’’ [3]. The ‘‘most interesting’’ 31 32 [7] [8] [9] [10] [11] [12] [13] [14] Conclusion In summary, pre-excitation syndrome has a long and interesting history. This ECG abnormality was originally classified as BBB. Two years after Wolff and coworker’s classic article, Holzmann and Scherf and then Wolferth and Wood suggested accessory connection as its cause. In 1942, Wood et al. first reported the human anatomical substrate of the pre-excitation syndrome. However, even after documentation of accessory pathways, the search for alternative mechanisms continued. Finally, electrophysiological studies and ablative surgical therapy confirmed accessory A-V connections as the underlying mechanism of pre-excitation syndrome and put the debate to rest. [15] [16] [17] [18] [19] [20] [21] References [22] [1] Wilson FN. A case in which the vagus influenced the form of the ventricular complex of the electrocardiogram. Arch Intern Med 1915;16:1008e27. [2] Wedd AM. Paroxysmal tachycardia with reference to nomotopic tachycardia and the role of the extrinsic cardiac nerves. Arch Intern Med 1921;27:571e90. [3] Hamburger WW. Bundle branch block. Four cases of intraventricular block showing some interesting and unusual clinical features. Med Clin North Am 1929;13: 343e62. [4] Wolff L, Parkinson J, White PD. Bundle-branch block with short P-R interval in healthy young people prone to paroxysmal tachycardia. Am Heart J 1930;5:685e704. [5] Ohnell RF. Pre-excitation, a cardiac abnormality. Acta Med Scand 1944;52(Suppl.):1e167. [6] Segers M, Lequime J, Denolin H. L’activation ventriculaire precoce de certain coeurs hyperexcitables. Etude de [23] [24] [25] [26] [27] l’onde de l’electrocardiogramme. Cardiologia 1944;8: 113e67. Cohn AE, Fraser FR. Paroxysmal tachycardia and the effect of stimulation of the vagus nerve by pressure. Heart 1913e14;5:93e105. Curtis CW, Hamilton CK. Electrocardiographic changes in rheumatic fever. Lancet 1926;807e9. Kent AFS. Researches on the structure and function of the mammalian heart. J Physiol 1893;14:233e54. Lewis T. The mechanism and graphic registration of the heart beat. London: Shaw and Sons Ltd; 1925. p. 13. Holzmann M, Scherf D. Uber Elektrokardiogramme mit verkurzter Vorhof-Kammerdiztanz und positiven P-Zacken. Z Klin Med 1932;121:404e23. Wolferth CC, Wood FC. The mechanism of production of short P-R interval and prolonged QRS complexes in patients with presumably undamaged hearts; hypothesis of an accessory pathway of auriculo-ventricular conduction (bundle of Kent). Am Heart J 1933;8:297e311. Mahaim I. Kent’s fibers and the A-V paraspecific conduction through the upper connections of the bundle of HisTawara. Am Heart J 1947;33:651e3. Wood FC, Wolferth CC, Geckeler GD. Histologic demonstration of accessory muscular connections between auricle and ventricle in a case of short P-R interval and prolonged QRS complex. Am Heart J 1943;25:454e62. Lev M. Anatomic consideration of anomalous AV pathways. In: Dreifus LS, Likoff W, editors. Mechanisms and therapy of cardiac arrhythmias. New York: Grune & Stratton; 1966. p. 665e70. Lev M. Anatomic considerations of anomalous AV pathways. In: Dreyfus LS, Likoff W, editors. Cardiac arrhythmias. New York: Grune & Stratton; 1973. p. 417e9. Becker AE. Morphologic characteristics of arrhythmias. In: Brugada P, Wellens HJJ, editors. Cardiac arrhythmias. Where to go from here? Futura Publishing Co: Mount Kisco; 1987. p. 1e26. James TN. Morphology of the human atrioventricular node with remarks pertinent to its electrophysiology. Am Heart J 1961;62:756e71. Scherf D, Cohen J. The atrioventricular node and selected cardiac arrhythmias. New York: Grune & Stratton; 1964. p. 372e447. Sodi-Palares D, Calder RM. New bases of electrocardiography. St Louis: Mosby; 1956. p. 596e616. Prinzmetal M, Kennamer R, Corday E, et al. Accelerated conduction. The WolffeParkinsoneWhite syndrome and related conditions. New York: Grune & Stratton; 1952. Kossman C, Berger AR, Rader B, et al. Anomalous atrioventricular excitation produced by catheterization of normal human hearts. Circulation 1950;1:902e9. Sherf L, James TN. New electrocardiographic concept: synchronized sinoventricular conduction. Chest 1969;55: 127e40. Butterworth JS, Poindexter CA. Short P-R interval associated with a prolonged QRS complex. A clinical and experimental study. Arch Intern Med 69:437e45. Durrer D, Roos JP. Epicardial excitation of the ventricles in a patient with the WolffeParkinsoneWhite Syndrome (type B). Circulation 1967;35:15e21. Durrer D, Schuilenburg RM, Wellens HJJ. Pre-excitation revisited. Am J Cardiol 1970;25:690e7. Burchell HB, Frye RL, Anderson MW, et al. Atrioventricular and ventriculo-atrial excitation in WolffeParkinsoneWhite syndrome (type B): temporary ablation at surgery. Circulation 1967;36:663e72. Downloaded from http://europace.oxfordjournals.org/ by guest on April 16, 2014 myocardial infarction was erroneous. He still believed however, that the clinical syndrome could be attributed to ‘‘an attack of ventricular tachycardia’’ [35]. The case was recognized for its similarity to those described by Wolff, Parkinson, and White, in that the young steamfitter was free of organic heart disease, yet a ventricular origin for the arrhythmias was assumed. These wide complex rhythms initially thought to be ventricular in origin are in fact, the result of a supraventricular rhythm inducing a ventricular complex that is broad and slurred. Additional reports detailing ventricular tachycardia and fibrillation in WPW syndrome abound [3,35e41]. However, as understanding of the condition advanced, retrospective review of the rhythms reported as ventricular in origin called these diagnoses into question [42]. S. Hanon et al. Early history of the pre-excitation syndrome [35] Levine SA, Beeson PB. The WolffeParkinsoneWhite syndrome with paroxysms of ventricular tachycardia. Am Heart J 1941;22:401e9. [36] Gilchrist AR. Paroxysmal ventricular tachycardia. A report of five cases. Am Heart J 1926;1:546e63. [37] Schiebler GL, Wood RS, Johnson WS. Paroxysmal pseudoventricular tachycardia in an infant with the Wolff Parkinson White syndrome. J Florida Med Ass 1963;49:805. [38] Yahini JH, Zahavi I, Neufeld HN. Paroxysmal atrial fibrillation in the Wolff Parkinson White syndrome simulating ventricular tachycardia. Am J Cardiol 1964;14:248. [39] Herrmann GR, Aotes JR, Runge TM, Hejtmancik MR. Paroxysmal pseudoventricular tachycardia and pseudoventricular fibrillation in patients with accelerated A-V conduction. Am Heart J 1957;53:254. [40] Lown B, Ganong WF, Levine SA. The syndrome of short P-R interval, normal QRS complexes and paroxysmal rapid heart action. Circulation 1952;5:693. [41] Hejtmancik MR, Herrmann GR. The electrocardiographic syndrome of short P-R interval and broad QRS complexes. Am Heart J 1957;54:708e21. [42] Langendorf R, Lev M, Pick R. Auricular fibrillation with anomalous A-V excitation (WPW syndrome) imitating ventricular paroxysmal tachycardia. Acta Cardiol 1952; 7:241. Downloaded from http://europace.oxfordjournals.org/ by guest on April 16, 2014 [28] Cobb FR, Blumenschein SD, Sealy WC, Boineau JP, Wagner GS, Wallace AG. Successful surgical interruption of the bundle of Kent in a patient with WolffeParkinsone White syndrome type A. Circulation 1968;38:1018e29. [29] Castellanos Jr A, Agha AS, Castillo CS, et al. Ventricular activation in the presence of WolffeParkinsoneWhite syndrome. In: Dreifus LS, Likoff, editors. Cardiac arrhythmias. New York: Grune & Stratton; 1973. p. 457e74. [30] James TN. Heuristic thoughts on the WolffeParkinsone White syndrome. In: Schlant RC, Hurst JW, editors. Advances in electrocardiography. New York: Grune & Stratton; 1976. p. 199e217. [31] Ferrer IM. New concept relating to pre-excitation. JAMA 1967;201:162e3. [32] Lev M, Leffler WB, Langendorf R, et al. Anatomic finding in a case of ventricular pre-excitation (WePeW). Circulation 1966;34:718e33. [33] Tchou P, Lehmann MH, Jazayeri M, et al. Atriofascicular connection or a nodoventricular Mahaim fiber? Electrophysiologic elucidation of the pathway and associated reentrant circuit. Circulation 1988;77:837e48. [34] Klein GJ, Guiraudon GM, Kerr CR, et al. Nodoventricular accessory pathway: evidence for a distinct accessory atrioventricular pathway with atrioventricular node-like properties. J Am Coll Cardiol 1988;11:1035e40. 33