Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
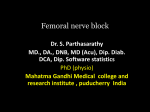
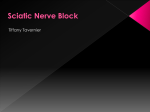
Femoral Nerve GOAL The goal is to place the needle tip immediately adjacent to the lateral aspect of the femoral nerve, either below the fascia iliaca or between the two layers of the fascia iliaca, into the wedge-shaped tissue space lateral to the femoral artery. Proper deposition of local anesthetic is confirmed by observation of the femoral nerve being lifted off of the surface of the iliopsoas muscle or of the spread of the local anesthetic above in the wedged-shaped space lateral to the artery. Technique With the patient in the supine position, the skin over the femoral crease is disinfected and the transducer is positioned to identify the femoral artery and/or nerve (Figure 4). If the nerve is not immediately apparent lateral to the artery, Figure 7: A simulated needle path (1) and spread of the local anesthetic (blue shaded area) to block the femoral nerve (FN). FA, femoral artery. Figure 6: An ultrasound tilting the transducer proximally or distally often helps to image and highlight the nerve from the rest of the iliopsoas muscle and the more superficial adipose tissue. In doing so, an effort should be made to identify the iliopsoas muscle and its fascia as well as the fascia lata because injection underneath a wrong fascial sheath may not result in spread of the local anesthetic in the desired plane. Once the femoral nerve is identified, a skin wheal of local anesthetic is made on the lateral aspect of the thigh 1 cm away from the lateral edge of the transducer. The needle is inserted in-plane in a lateral-to-medial orientation and advanced toward the femoral nerve (Figure 5). If nerve stimulation is used (0.5 mA, 0.1 msec), the passage of the needle through the fascia iliaca and contact of the needle tip with the femoral nerve usually is associated with a motor response of the quadriceps muscle group. In addition, a needle passage through the fascia iliaca is often felt as a "pop" sensation. Once the needle tip is witnessed adjacent (either above, below, or lateral) to the nerve (Figure 6), and after careful aspiration, 1 to 2 mL of local anesthetic is injected to confirm the proper needle placement (Figure 7). When injection of the local anesthetic does not appear to result in a spread close to the femoral nerve, additional needle repositions and injections may be necessary. In an adult patient, 10 to 20 mL of local anesthetic is adequate for a successful block (Figure 8A and B). image of the needle path (1,2) to block the femoral nerve. Both needle positions are underneath fascia iliaca, one superficial to the femoral nerve (1) and one deeper to it (2). Either path is acceptable as long as the local anesthetic spreads within the fascia iliaca (white line) to get in contact with the femoral nerve. Continuous Ultrasound-Guided Femoral Nerve Block The goal of the continuous femoral nerve block is similar to that of the non-ultrasound-based techniques: placement of the catheter in the vicinity of the femoral nerve just deep to the fascia iliaca. The procedure consists of three phases: needle placement, catheter advancement, and securing the catheter. For the first two phases of the procedure, ultrasound can be used to ensure accuracy in most patients. The needle typically is inserted in-plane from the lateralto-medial direction and underneath the nerve. Some clinicians prefer inserting the catheter in the longitudinal plane (inferior-to-superior), analogous to the nerve stimulation-guided technique. No data exist on whether or not one technique is superior to the other. However, the in-line approach from the lateral-to-medial has worked very well in our practice, and it is our preference because it is simpler when using ultrasound guidance. Figure 8: (A) An actual needle path to block the femoral nerve (FN). (B) Spread of the local anesthetic (LA) within two layers of the fascia iliaca to encircle the femoral nerve (FN). FA, femoral artery. The needle is advanced until the tip is adjacent to the nerve. Proper placement of the needle can be confirmed by obtaining a motor response of the quadriceps/patella, at which point 5 mL of local anesthetic is injected. This small dose of local anesthetic serves to ensure adequate distribution of the local anesthetic, as well as to make the advancement of the catheter easier. This first phase of the procedure does not significantly differ from the single-injection technique.