Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
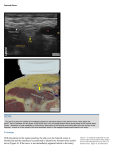
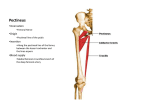
Femoral nerve block Dr. S. Parthasarathy MD., DA., DNB, MD (Acu), Dip. Diab. DCA, Dip. Software statistics PhD (physio) Mahatma Gandhi Medical college and research institute , puducherry India Indications procedures carried out on the anterior thigh Combined with other blocks – lower leg and foot surgeries femoral fracture analgesia With catheter technique – post op analgesia of knee Anatomy • largest nerve of the lumbar plexus ( L2- L4) • supplies the muscles and the skin of the anterior compartment of the thigh • passes downwards in the groove between psoas and iliacus • enters the thigh beneath the inguinal ligament • nerve lies on iliacus, a finger’s breadth lateral to the femoral artery Anatomy Technique • A line is drawn connecting the anterior superior iliac spine and the pubic tubercle. • The femoral artery is palpated on this line, and a 22-gauge, 4-cm needle is inserted 0.5 to 1 cm both below the inguinal ligament and lateral to the femoral artery. • The initial insertion should abut the femoral artery in a perpendicular fashion. • wall” of local anaesthetic is developed by redirecting the needle in a fanlike manner Line marked Needle insertion Injection of LA spanning out Drugs • 20 mL of local anaesthetic 0.25 to 0.5 % bupivacaine • 0.25% bupivacaine or 0.2% ropivacaine for catheter techniques • 8- 10 ml / hour is enough Nerve stimulator • The femoral artery should be palpated and marked. The site of introduction of the needle is vertically, 0.5 to 1 cm both below the inguinal ligament and lateral to the femoral artery. • Set the nerve stimulator at a frequency of 2 Hz and a current of 2.5 mA. • Go anteroposterior and get motor response of the femoral nerve (contraction of the quadriceps muscle with the phenomenon of the “dancing patella”). • Reduce to 1 Hz and 0.5 mA - same response - and inject. technique • Needle positioned, • 20 mL of preservative-free NS injected appropriate-size catheter is inserted approximately 10 cm past the needle tip. • Once the catheter has been secured with a plastic occlusive dressing, the initial bolus injection of drug is carried out and the infusion is started. Continuous catheter USG probe USG guided femoral nerve block Tips • The femoral artery and femoral nerve are not in the same anatomic compartment. • Therefore, if solution spreads perivascularly, the needle should be repositioned to produce local anesthetic spread below the fascia iliaca. Anatomy • The obturator nerve emerges from the medial border of the psoas muscle at the pelvic brim and travels along the lateral aspect of the pelvis anterior to the obturator internus muscle and posterior to the iliac vessels and ureter. It enters the obturator canal cephalad and anterior to the obturator vessels, which are branches from the internal iliac vessels. Obturator nerve block adductor muscles, hip and knee joint • In the obturator canal, the obturator nerve divides into anterior and posterior branches The anterior branch supplies the anterior adductor muscles ,articular branch to the hip joint , cutaneous area on the medial aspect of the thigh. • The posterior branch innervates the deep adductor muscles and sends an articular branch to the knee joint.. Technique • The pubic tubercle should be located and an “X” marked 1.5 cm caudad and 1.5 cm lateral to the tubercle • The needle is inserted at this point, and at a depth of approximately 2 to 4 cm it contacts the horizontal ramus of the pubis. • The needle is then withdrawn, redirected laterally in a horizontal plane, and inserted 2 to 3 cm deeper than the depth of the initial contact with bone. • The needle tip now lies within the obturator canal • With the needle in this position, 10 to 15 mL of local anesthetic solution is injected Technique Complications • The obturator canal is a vascular location; thus, the potential exists for intravascular injection or hematoma formation, • more theoretical than clinical concerns. • Volume determines success. Probe position USG Lateral femoral cutaneous N block why ? Technique Technique • The anterior superior iliac spine is marked in the supine patient, • and a 22-gauge, 4-cm needle is inserted at a site 2 cm medial and 2 cm caudal to the mark, the needle is advanced until a “pop” is felt as the needle passes through the fascia lata. Local anesthetic is then injected in a fanlike manner above and below the fascia lata, from medial to lateral. Technique Three in one block • The perivascular approach to the psoas compartment is based on the premise that injection of a large volume of local anesthetic within the femoral canal while maintaining distal pressure will result in proximal spread of the solution into the psoas compartment and consequent lumbar plexus block Technique • The femoral artery is marked. A 22- gauge, 5- cm needle is advanced lateral to the artery in a cephalad direction Paraesthesia – 30 ml given Distal pressure applied Success - ? Thank you all