Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
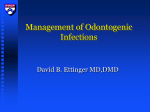
About Face! – Causes of Non-traumatic Facial Swelling Ari J. Spiro, MD Judah Burns, MD Andrew Friedman, MD Matthew H. Neimark, MD, PhD Meir H. Scheinfeld, MD, PhD R. Joshua Dym, MD eEdE-150 Disclosure Nothing to disclose Introduction ▪ ▪ ▪ ▪ Facial swelling is a common presenting scenario in the UrgiCare or ED setting. Inflammatory causes are common, particularly with rapid onset of swelling; malignancy and acquired etiologies must also be considered. Imaging helps to narrow the differential diagnosis. The purpose of this exhibit is: › To present a space-based diagnostic approach to the differential diagnosis of facial swelling › To review both common and rare conditions that may present with this clinical complaint Topic Outline ▪ Orbit/Periorbital Space ▪ ➢ Odontogenic Abscess ➢ Periorbital cellulitis ➢ Orbital Pseudotumor ▪ ➢ Pott’s puffy tumor ▪ Submandibular Space ➢ Sialolithiasis ➢ Sialoadenitis Sublingual Space / Potential airway compromise ➢ Ludwig’s angina ➢ Angioedema ▪ Superficial/Subcutaneous ➢ Facial Cellulitis ➢ SCC Masticator Space ▪ Parotid Space ➢ Infected branchial cleft cyst ▪ Mastoid related disease ➢ Bezold’s Abscess Suprahyoid Neck Anatomy Credit: Statdx: ( see suggested reading) Axial graphic depicting the spaces of the suprahyoid neck. Surrounding the paired fat-filled parapharyngeal spaces are the four critical paired spaces of this region, the pharyngeal mucosal, masticator, parotid and carotid spaces. The retropharyngeal and perivertebral spaces are the midline non-paired spaces. Credit: Statdx: ( see suggested reading) Coronal graphic of suprahyoid neck spaces as they interact with the skull base. The masticator space has the largest area of abutment with the skull base, including CNV3. The pharyngeal mucosal space abuts the basisphenoid and foramen lacerum. Suprahyoid/Infrahyoid Neck Credit: Statdx: ( see suggested reading) Credit: Statdx: ( see suggested reading) Axial graphic of the suprahyoid neck spaces at the level of the oropharynx. The superficial (yellow line), middle (pink line) and deep (turquoise line) layers of deep cervical fascia outline the suprahyoid neck spaces. Notice the lateral borders of the retropharyngeal & danger spaces are called the alar fascia and represents a slip of the deep layer of deep cervical fascia. Axial graphic depicting the fascia and spaces of the infrahyoid neck. The three layers of deep cervical fascia are present in the suprahyoid and infrahyoid neck. The carotid sheath is made up of all 3 layers of deep cervical fascia (tri-color line around carotid space). Case1 and Companion 2 different patients presenting to the Emergency Department with recent onset of periorbital swelling. Periorbital/Orbital Cellulitis ▪ Preseptal cellulitis – Periorbital soft tissues anterior to orbital septum ▪ Postseptal cellulitis – Intraconal or extraconal. › ▪ Subperiosteal Abscess: Between medial periosteum & lamina papyracea. › ▪ CECT: Enhancing, edematous orbital fatty reticulum. Occasional myositis with enhancement of rectus muscles. NECT: Left periorbital swelling, with lowdensity phlegmon in the superior orbit, obscuring the superior rectus muscle Progression from phlegmon → subperiosteal abscess Treatment: Cellulitis/phlegmon – ABX; Abscess – Surgical drainage NECT: Right ethmoid sinus disease, orbital swelling, subperiosteal abscess Case 2 46 year old female with history of left upper lid retraction and swelling, mild proptosis, and left inferior rectus restriction. Orbital Pseudotumor ▪ Idiopathic Orbital Inflammatory Disease Top Differential Diagnosis: ▪ Diagnosis of exclusion ▪ ▪ ▪ ▪ ▪ ➢ 3rd most common primary lesion of the orbit ▪ May involve any orbital structure ➢ Frequency of involvement: EOM>lacrimal gland > globe or retrobulbar > diffuse > apex ▪ 25% Bilateral T2W MRI: Left preseptal soft tissue swelling. Enlarged left lacrimal gland and superior rectus muscle. Lymphoproliferative lesions Thyroid ophthalmopathy Sarcoidosis Wegener granulomatosis Orbital cellulitis Case 3 and Companion 56 year old male with history of chronic sinusitis presents with 3 days of progressive facial pain, and left periorbital / scalp swelling. 13 year old male with history of sinusitis presents with 5 days of fever, facial pain, and periorbital / scalp swelling. “Pott’s Puffy Tumor” 56 yo male: CECT: Left frontal sinusitis extending through frontal cortex with periorbital and subperiosteal extension 13 yo male: MRI: CE-T1W: Left frontal sinusitis with subgaleal phlegmon/abscess involving the left scalp. Intracranial extension with epidural abscess is also noted. “Pott’s Puffy Tumor” Sinusitis is a common disorder that can rarely result in serious complications including: Periorbital or orbital cellulitis Intracranial abscess or meningitis Subperiosteal scalp abscess – “Pott’s puffy tumor” Osteomyelitis Cavernous venous thrombosis Diagnosis of “Pott’s puffy tumor” can be made with CECT or MRI. CECT is preferred over MRI due to finer bony detail Treatment includes intravenous antibiotics and surgical intervention. Early intervention significantly contributes to favorable outcome and decreases the risk of further complications. Case 4 50 year old male presents to the Emergency Department with left facial swelling and erythema. Facial/Superficial Cellulitis ▪ Acute infection of the dermis and subcutaneous tissues ▪ ▪ CT utilized to differentiate between superficial cellulitis and cellulitis associated with deep-seated infection ▪ ▪ ▪ Patients with diabetes melitis or peripheral vascular disease are more susceptible CT findings: Skin thickening, septation of the subcutaneous fat, thickening of underlying fascia Deep-seated infection can lead to abscess, myositis, necrotizing fasciitis Treatment: ▪ ▪ Superficial- ABX Deep - may require surgical intervention CECT: Skin thickening, infiltration of subcutaneous soft tissues and platysma of the left face. Case 5 60 year old female history of submandibular gland swelling presents to the Emergency Department complaining of 2 days of acute right submandibular pain. Sialadenitis and Sialolithiasis ▪ Acute sialadenitis is an infectious or inflammatory disorder of the salivary glands Patients present with swelling exacerbated by eating ➢ Bacterial, viral, and autoimmune processes are the most common etiologies ▪ CECT: Enlarged enhancing submandibular gland with ductal dilatation secondary to an obstructive calculus or stenosis ➢ Myositis or cellulitis often present in sublingual or submandibular spaces. ▪ 80-90% of submandibular sialadenitis cases are associated with ductal calculi (sialoliths), while sialoliths are identified in 10-20% of cases of parotid sialadenitis. ▪ Sialoliths occur more often in submandibular duct (Wharton’s duct) due to large diameter, ascending course, more mucinous salivary content, and salivary stasis. CECT: Enlargement of bilateral submandibular glands and ducts containing calculi (sialoliths). Inflammatory stranding adjacent to the right submandibular gland c/w sialadenitis. Case 6 35 year old male presents to Emergency Department with jaw pain and left cheek swelling. Odontogenic Abscess ▪ ▪ ▪ ▪ ▪ Lower facial swelling should be evaluated for potential infection arising from pre-existing dental disease CECT is the preferred modality for evaluation of oral cavity infections and suspected odontogenic abscess Bone window settings may reveal lucency surrounding dental roots “floating roots”, cortical dehiscence, and osteomyelitis. 2nd or 3rd molar tooth infection likely involves the submandibular space, infections of the more anterior teeth are confined to the sublingual space Treatment: tooth extraction, abscess drainage, and ABX CECT: Lucency surrounding the root of the left 3rd mandibular molar with cortical dehiscence adjacent to a superficial facial abscess with associated cellulitis. Case 7 44 year old male smoker and heroin user status post hospitalization for mouth abscess after tooth extraction. Ludwig’s Angina ▪ Infection of the floor of the mouth that extends bilaterally to soft tissues of oral cavity ➢ Rapid extension-potentially life- threatening ➢ Establishing a secure airway is a priority as soft tissue swelling displaces the tongue into the pharyngeal airway ▪ ▪ ▪ Termed “Ludwig’s angina” to account for the experience of pain described by patients Most often caused by infection of 3rd mandibular molar tooth or pericoronitis CECT to assess airway patency, presence of gas-forming organisms, underlying dental infection, or drainable abscess CECT: Floor of mouth abscess. Edema of the bilateral submandibular space, right parapharyngeal space, and aryepiglottic fold. Case 8 45 year old female presents to the Emergency Department with mandibular swelling after recent increase in dosage of her ACE inhibitor. Rule out abscess. Angioedema ▪ ▪ ▪ Transient swelling Primarily affects the face, tongue, lips and larynx, possible airway compromise ACE inhibitor most common cause ➢ Can develop shortly after starting therapy, however reaction can occur months or even years later. ▪ ▪ Treatment includes cessation of ACE inhibitor, initiation of steroid and antihistamine therapy, and airway support. CECT: infiltrative edema with circumferential mucosal thickening, however unilateral mass like areas have also been described CECT: Enlarged lower lip with heterogeneous enhancement consistent with angioedema in the setting of recent ACE inhibitor dose increase. Lat XR: Soft tissue swelling of the epiglottis, and upper and lower lips in this patient 1 day after starting ACE-I therapy. Case 9 33 year old male presents to Emergency Department with left neck pain. Branchial Cleft Cyst ▪ Best diagnostic clue: Cystic neck mass posterolateral to submandibular gland, lateral to carotid space, anterior (or anteromedial) to SCM ▪ If infected, wall is thicker & enhances with surrounding soft tissue cellulitis ▪ Differential diagnosis: ➢ ➢ ➢ ➢ ➢ Lymphatic malformation Cervical thymic cyst Lymphadenopathy/abscess Cystic metastatic nodes Carotid space schwannoma Rim enhancing cystic structure posterior to the submandibular gland and anterior to the sternocleidomastoid muscle. DDX infected 2nd branchial cleft cyst vs necrotic lymph node Case 10 11 year old male presents to the emergency department with posterior auricular edema. Bezold’s Abscess ▪ Rare complication of mastoiditis with necrosis of the mastoid tip, infectious spread into the adjacent soft tissues, and abscess formation - “Bezold’s abscess” ▪ The abscess may lie deep relative to the superficial planes that surround the sternocleidomastoid muscle and trapezius muscles, and may therefore not be palpable ▪ Infection may spread as far inferiorly as the larynx and mediastinum if untreated ➢ Involvement of the mastoid process in the presence of a neck abscess may require surgical exploration of the neck and temporal bone CECT: Coalescent mastoiditis with a subperiosteal abscess just posterior to the pinna Case 11 37 year old female with no PMH presents to the Emergency Department with 3 days of fever and right face/neck swelling/mass. Infectious Cervical Lymphadenopathy ▪ Broad differential diagnosis depending on demographics, underlying systemic disease, and presentation ▪ Increased prevalence of Tuberculous lymphadenopathy (scrofula) in HIV patients ▪ Bilateral cervical lymphadenitis common; however, may involve single lymph node ▪ CT or MRI may demonstrate enhancing and necrotic lymph nodes ➢ DDX includes metastatic disease from entities such as squamous cell or thyroid cancer. CECT: Marked levels II-V necrotic lymphadenopathy. Edematous enlargement of the right SCM. Biopsy proven TB adenitis. Case 12 61 year old male with history of Stage IV lung squamous cell carcinoma (SCC) and SCC of nasal tip presents with left facial swelling. Post-treatment SCC ▪ Imaging overlap of post-treatment change and tumor recurrence can make post-treatment head and neck cancer imaging challenging to interpret ▪ Acute inflammatory reaction interstitial edema progressive connective tissue thickening further interstitial edema progressive fibrosis is the expected sequence of events after radiotherapy ▪ Knowledge of surgical dissection/resection and surgical reconstruction is paramount to differentiate post-operative complications from typical post-procedural change ▪ Research has shown that tumor recurrence can be detected earlier by systematic follow-up imaging NECT: ST mass overlying the nasal bone c/w known SCC. Additional mass in the left premaxillary soft tissues with adjacent soft tissue swelling. Findings c/w biopsy proven metastatic disease Conclusion ▪ ▪ ▪ ▪ Although a relatively small in size, the face is a complex anatomical region. Various types of pathology can lead to facial swelling, some of which can lead to airway compromise. Most of these abnormalities require imaging assessment. Radiologists should be familiar with the diverse entities and imaging findings in patients with facial swelling to recognize expected and unexpected findings in order to improve patient care. Suggested Reading ▪ Castillo M, Albernaz VS, Mukherji SK, Smith MM, Weissman JL. Imaging of Bezold’s Abscess. AJR 1998;171:1491-1495 ▪ LeBedis CA, Sakai O. Nontraumatic orbital conditions: diagnosis with CT and MR imaging in the emergent setting. Radiographics. Oct 2008; 28(6):1741-1753. ▪ Tailor TD, Gupta D, Dalley RW, Keene CD, Anzai Y. Orbital neoplasms in adults: clinical, radiologic, and pathologic review. Radiographics. Oct 2013;33(6):1739-1758. ▪ Rahmouni A, Chosidow O, Mathieu D et-al. MR imaging in acute infectious cellulitis. Radiology. 1994;192 (2): 493-6. ▪ Capps EF, Kinsella JJ, Gupta M, Bhatki AM, Opatowsky MJ. Emergency imaging assessment of acute, non-traumatic conditions of the head and neck. Radiographics 2010 Sep;30(5):1335-52. ▪ ReBannon PD, McCormack RF. Potts’ puffy tumor and epidural abscess arising from pansinusitis. The Journal of Emergency Medicine, Vol. 41, No. 6, pp. 616–622, 2011 ▪ Kubal WS, Face and neck infections: What the emergency radiologist needs to know. Radiol Clin N Am 53 (2015) 827-846 ▪ Zurlo A, Sancesario G, Bernardi G, Loasses A. Orbital Pseudotumor: Case report and literature review. Tumori. 85: 6870, July 1998. ▪ StatDx, Koch BL, 2nd branchial cleft cyst. https://app.statdx.com/document/2nd-branchial-cleft-cyst/417aa034-e152-4c67b1fa-a25c03a8c83d?searchTerm=branchial%20cleft%20cyst ▪ Hermans R. Post-treatment imaging of head and neck cancer. Cancer Imaging (2004) 4, S6-S15 ▪ Images on slides 4-5: Statdx, Elsevier, inc, Suprahyoid and Infrahyoid Neck Overview. Graphics. https://app.statdx.com/document/suprahyoid-and-infrahyoid-neck-ove-/002dc4b8-c8b8-438a-82f4-d3fb5e5a8b15, 4/27/16.