Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Behçet's disease wikipedia , lookup
Traveler's diarrhea wikipedia , lookup
Urinary tract infection wikipedia , lookup
Childhood immunizations in the United States wikipedia , lookup
Infection control wikipedia , lookup
Multiple sclerosis signs and symptoms wikipedia , lookup
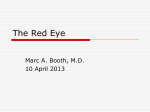
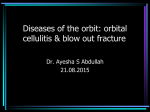
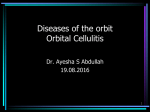
Blow out fracture of the orbit (BOF) Ayesha S Abdullah 14.09.2012 Learning objectives 1. Differentiate between preseptal and true orbital cellulitis (OC) & explain why it is considered to be an ocular emergency 2. Describe the causes, clinical presentation, complications & line of management of orbital cellulitis 3. Explain the mechanism of BOF of the orbit, describe its clinical presentation, complications & outline the management. Review Case #1 A one-year old baby presented to the OPD of the department of Ophthalmology with the complaint of a red swollen left lower lid for the last two days. On examination the lid was red, warm & mildly tender to touch. His vision was normal, the eye had mild conjunctival redness, pupils were normal and the ocular movements were also normal. Watch the photograph…. Some questions 1. 2. 3. 4. 5. What kind of orbital condition is this? What structures are affected? What more information should we ask for to? What possible causes can you think of? Is the condition confined to the lids or has it involved the eyeball? 6. Why do you think so? 7. Would you like to have more information? Some more information……… • The child had a history of insect bite on the lid two days ago, the swelling increased thereafter. The insect bite mark was visible • There was no history of trauma or symptoms suggestive of flu or URTI • His temperature was normal Some more questions • What should be the management, keeping in mind the nature of the problem? • What could be the complications of such a case? • Is there any role of health education in this case? Don’t’ forget simple things can get complicated • Let us see an other case…….. Case #2 • A 12 year old child was brought to the OPD of the department of ophthalmology with a history of red swollen left upper lid for the last 5 days. He also had fever for the last two days along with headache. On examination the child had a grossly swollen lid. His visual acuity was 6/18 OD & 6/6 OS. The lid was warm and tender. The eye was moderately proptosed with conjunctival chemosis. The pupil was slow to react to light and the ocular movements were painful & limited. The temperature was 1010 F & the child generally looked unwell…….. Ocular signs Some questions…. 1. What kind of orbital condition is this? 2. What structures are affected? 3. What more information should we ask for to get an idea about the cause of the problem? 4. Is the condition confined to the lids or has it involved the eyeball? 5. Why do you think so? 6. What possible causes can you think of? 7. Would you like to have more information? Some more information……. • The child had a history of recurrent flu and upper respiratory tract infections. He had history of blocked nose and thick greenish nasal discharge was noted on examination. • The child was put on intravenous antibiotics but didn’t get better • A subsequent CT scan was done which showed……. The antibiotics were changed to intravenous ampicillin/sulbactam and after 5 days were changed to oral amoxicillin/clavulanic acid for a total of 14 days of antibiotics. Orbital abscess Some more questions • What should be the management, keeping in mind the nature of the problem? • What do you think can be done with the abscess? • Is there any role of health education in this case? Conclusion about the two cases • What is the difference between the two cases? • We consider the second case an ocular emergency, why? • How did the subperiosteal abscess form in the second case? • What other complications could happen in the second case? Ocular/intracranial/orbital • What could be included in the differential diagnosis?.... Differential diagnosis of red swollen lids 1. 2. 3. 4. Prespetal cellulitis Orbital cellulitis Contact dermatitis Focal lesions like stye, chalazion ( especially if infected) 5. Allergic reaction ( angioedema) 6. Tumours ( specifically Rhabdomyosarcoma in children & malignant lid tumours, primary or secondary in adults) Management Preseptal cellulitis 1. Symptomatic; analgesics & NSAIDS 2. Specific: 3. For mild infection oral antibiotics with antihistamines in case of dual pathology like in insect bite 4. Very severe infections may require intravenous penicillins to avoid true orbital cellulitis 5. Lid abscesses should be drained 6. Third generation cephalosporins in penicillin allergy 7. In general practice it requires oral antibiotics and referral to an ophthalmologist especially when more severe and in children Management Orbital Cellulitis • • • • Admit Requires care by an ophthalmologist Symptomatic; antipyretic, NSAIDS Specific ; hospitalization & antibiotic therapy – – – – Braod spectrum antibiotic (I/V); Ceftazidime or cefotaxime Ampicillin for H Influenzae infection Cloxacillin for Staphylococcus aureus infection Metronidazole 500mg tds, PO when anaerobic infection is suspected especially in adults – Vancomycin in case of allergy to the above mentioned Management Orbital Cellulitis • Surgical intervention in case of local abscess or unresponsive cases • Consultation with ENT specialist, neurosurgeon & paediatrician if required Let us summarize • Preseptal orbital cellulitis & orbital cellulitis are both infections. • It is more common in children • The route of infection could be from the nearby infectious focus like infected sinuses, skin wound or spread of infection via blood • The most common cause especially in children is ethmoidal sinusitis • Both preseptal and orbital cellulitis may have: – Fever – Eyelid edema – Pain – Red eye – Child is ill-appearing • Orbital cellulitis signifies spread of inflammation to the posterior orbital contents that is the eyeball, extraocular muscles: helpful signs to distinguish it are:– Proptosis – Decreased visual acuity ( may be normal in the beginning) – Red eye with conjunctival chemosis of moderate to intense congestion – Painful limited eye movements – Afferent pupillary defect Why is OC an emergency • Prior to the availability of antibiotics, patients with orbital cellulitis had a mortality rate of 17%, and 20% of survivors were blind in the affected eye. However, with prompt diagnosis and appropriate use of antibiotics, this rate has been reduced significantly • blindness can still occur in up to 11% of cases. Orbital cellulitis due to methicillin-resistant Staphylococcus aureus can lead to blindness despite antibiotic treatment. • The infection can spread to the meninges and brain & may cause death • That is why it is an emergency Ocular & orbital complications of OC • Corneal scarring from exposure Extraocular muscle palsies Optic nerve damage • Central retinal artery and central retinal vein occlusion • Orbital abscess • Visual loss and blindness Extraocular complications of OC • • • • Brain abscess Meningitis Cavernous sinus thrombosis Osteomyelitis of skull and orbit bones Cavernous sinus thrombosis Brain abscess Lets us see this case • A 45 year old umpire of cricket while standing at the wickets got hit by a close throw on his left eye a day earlier. He suddenly felt excruciating pain in and around the eye. As he opened his eyes he noticed double vision especially as he looked up. On examination he had a black eye (bruised) with limited upward movement of the left eye. • • • • What happened? Why was he having diplopia? Why did it get worse while looking up? What investigations would you like to do for confirming your diagnosis? • What complications can you expect in such a case? • How could it be managed? What happened? What investigation would you like to do to confirm the diagnosis? For confirmation of fracture • CT scan / X ray orbit For confirmation of muscle entrapment • CT scan & forced duction test, differential intraocular pressure assessment ( primary position and up-gaze) What complications can you expect in such a case? • EOM problems • Visual loss : Hyphaema, RD, Damage to the angle of the anterior chamber— glaucoma, Vitreous haemorrhage, Orbital hematoma,Damage to the optic nerve • Cosmetic , small eye, asymmetry in face • Secondary infection from the sinuses- orbital cellulitis & spread of the infected contents of the sinuses to the vital tissues like the eyeball & the brain How could it be managed? Is it an emergency? Should we admit? • Symptomatic/ conservative: NSAID for relief of pain & reduction of inflammation ( discourage blowing of the nose to prevent forcing of the infected sinus contents into the orbit), antibiotics • If the diplopia persist beyond 2 weeks/ enophthamos is significant then surgical repair of the fracture with release of entrapped muscles may be required Summary Blowout fracture is not a common disorder but is common in sports & violence related trauma, it can mostly be managed conservatively but in case of a large fracture or persistent ocular movement problems & enophthalmos requires surgical repair. References • Orbit, eyelids & lacrimal system. American Academy of Ophthalmology; 1997-98 • Jack J Kanski. Clinical ophthalmology a systematic approach. 5th ed;2003:557-89 • Parsons’ diseases of the eye. Diseases of the adnexadiseases of the orbit. 19th ed. 2004; 505-524 • Newell F W. The orbit. In Ophthalmology principles & concepts.7th ed; 1992:259-69 WEB RESOURCES • http://www.emedicine.com/oph/topic758.ht m. • http://www.emedicine.com/oph/orbit/exopht halmos • http://www.ccmcresidents.com/wpcontent/uploads/2011/08/242.full_.pdf