Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Coronary artery disease wikipedia , lookup
Heart failure wikipedia , lookup
Cardiac surgery wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Jatene procedure wikipedia , lookup
Congenital heart defect wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
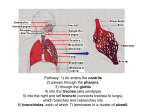
Fetus – birth • During delivery "asphyxia“ is certain The postpartum adaptation • Compensatory mechanisms: – Higher affinity of hemoglobin to oxygen – Shunting of oxygenated blood to the vital organs (heart and brain) – Fast tissue perfusion (high HR) Childbirth: changes of an environment • Water • • • • Quiet Darkness Optimally warm Protected → Air → Loud → Lightened → Cold → Unprotected • Gravitation ⇒ effect on the locomotor system • Stress reaction ⇒ epinephrine, norepinephrine, ACTH, cortisol The postpartum changes • Immediate: – first breath – circulatory changes • Slower changes: – liver – hemoglobin – kidneys Catecholamines • Potentiate the absorption of fluid from the bronchi • Potentiate secretion and release of surfactant • Mobilize of endogenous energy sources and their utilization • Activate thermogenesis to protect against cold • Regulation of circulation in the brain and heart • Support vigilance – "arousal" Respiratory system • Fetal respiratory system: – 3rd – 16th weeks = terminal bronchioles – 20th – 22nd weeks = pneumocytes of the 1st and 2nd types – 24th week = surfactant (secretion can be increased by betamethasone) • Development of alveoli continues after birth • 5th – 6th year = number of alveoli as in adult – 300 millions (5 times more than at birth) 1 Fetal lungs • For normal development require the presence of pulmonary fluid and fetal breathing movements • During 22nd – 24th fetal weeks ⇒ adequate circulation and alveolar gas exchange is also required Fetal breathing • For the development of lungs the following is necessary: – Mild contractions of diaphragm – Sign of abnormal development is presents of chest and abdominal wall movements that are (more than 30% of time) fast and uncoordinated (oligohydramnion, hydrothorax, musculoskeletal disorders, diaphragmatic hernia) • Gasping during asphyxia (meconium aspiration hazard) Fetal pulmonary fluid Secreted by 1st type pneumocytes – 135-180 ml/kg /day Fills the airways and alveoli 30 ml/kg Secreted only before birth → postpartum resorption (adrenaline) Resorption of fluid : – Is induced by chest compressions (passage via birth canal) – Is to lymphatic vessels First breath Chest compressions during passage via the birth canal squeezes fluid from the fetal lung • Stimuli for the first breath: – – – – hypoxia hypercapnia arousal sensory inputs from surrounding • sounds, touch, cold, pain • Energy demanding due to: – Resistance in the airways – Fluid in the lungs – Surface tension in the alveoli (air / water) NB: Role of NE and Cortisol!!! First breath • Opens alveoli ⇒ decreases tension in the wall (La Place: P = 2T / R) • Creates TLC, FRC, TV • The first exhalation is active ⇒ pushes out the amniotic fluid from the bronchi • Lung expansion and increased PAO2 ⇒ changes in the pulmonary circulation ⇒ changes in the systemic circulation Respiration in newborns and infants • Breathing through the nose mainly, its resistance is about 40% of the total airway resistance, – Dangers of swelling!!! – Hyperemia!! • Atresia of choans!! – Hypoxia is observed already in the delivery room 2 Respiratory changes • Energy demanding because they are very intensive Fetal circulation • Pulmonary circulation has high resistance (↓↓pO2) • Breathing is periodic – apnea is less than 5 seconds followed by tachypnoea • Beware of mother anesthesia! • Important: lung expansion and increased PAO2 leads to changes in the pulmonary circulation, which initiate changes in the systemic circulation Factors decreasing pulmonary vascular resistance • • • • Mechanical factors Increase of paO2 and rise of pH Decrease in paCO2 Increase levels of prostaglandins PGE2, PGI2 • Placenta has the lowest resistance in the fetal circulation • Both heart chambers are equally strong and pump blood in parallel rather than in series • Foramen ovale closes completely at the age of 5 years in 50% of children • In 30% of the population it remains open • Functional closure of the ductus arteriosus occurs within 60 hours in 93% of healthy newborns • Within 4-8 weeks closes completely Congenital heart defects ECG • Fetal circulation: – Right-sided dominance – 65% of CO • After the birth: – During 3rd – 6th months establishes classical left-sided dominance • Each year in the Czech Republic about 500 children are born with a heart defect : The most common congenital heart defects: • • • • • ventricular septal defect (VSD) atrial defect counter (ASD) aortic stenosis pulmonary artery stenosis transposition of the great arteries (TGA) •coarctation of the aorta (CoA) •patent ductus arteriosus (PDA) •atrioventricular septal defect •hypoplastic left heart •Tetralogy of Fallot • There are number of genetic disorder (chromosome aberrations) and environmental factors responsible for the formation of congenital heart defects • The critical period of heart development influenced external factors is 2nd to 8th weeks of pregnancy http://www.kardiochirurgie.cz/vrozene-vady 3 Congenital heart defects • Without shunt – coarctation of the aorta, valvular defects • Shunts with possible cyanosis – some of left-toright shunts • Cyanotic shunts – right-to-left • Factors determining the size of the shunt and direction of flow: pressure gradient, the exact location • The consequences of left-right circuit => response of pulmonary circulation and shunt redirection • The consequences of right-left shunt Hematologic changes HbF: α2γ2 HbA: α2β2 • At birth: HbF 70 – 80% • At 6 months, there is no HbF present • However, HbA production is not as fast (not enough Epo) • Physiological anemia during 8th-10th week http://pf.lf2.cuni.cz/vyuka/repetitoriumobeh/vrozene_srdecni_vady.html Liver • Enzymatic pathways are fully active after 3rd month • Conjugation of bilirubin is fully active after 2nd week Hyperbilirubinemia • Hyperbilirubinemia (regardless the age) defined as more than 25 umol/l of bilirubin in the blood • In newborns clinical manifestation of jaundice occur when the levels of bilirubin raise to 6885 umol/l. Icterus neonati (physiological neonatal jaundice, physiological hyperbilirubinemia) occurs in 45-65% of healthy newborns by the 5th day • It never occurs within the first 24 hours after birth • Physiological deficiency of vitamin K • The rate of increase of total bilirubin in physiologic jaundice should not exceed 85 umol/l/24hr Hyperbilirubinemia • Free, fat-soluble unconjugated bilirubin easily crosses the blood-brain barrier • Bilirubin is mostly bounded to albumin, however, during various pathological conditions (as asphyxia, acidosis, hypoperfusion, hyperosmolality, sepsis), the complex freely moves to the central nervous system • The exact concentration of bilirubin, which leads to the development of kernicterus is unknown Neonatal hyperbilirubinemia (jaundice pathological) classified on the basis of the pathophysiological mechanisms that lead to the accumulation of bilirubin in the tissues into three groups: 1. increased production of bilirubin, 2. decreased conjugation of bilirubin and 3. pathological excretion of bilirubin Autor: www.zdn.cz 4 Skin Termed newborn: • functionally immature skin vernix caseosa – waxy substance coating skin of newborn • Increased vulnerability - physical, chemical • Increased water loss • Decreased anti-infective barrier ⇒ eczema Temperature regulation in newborns Temperature after birth = maternal core temperature Thermoneutral environment for newborn during the first week after birth is: – for naked full-term 32 to 34 º C – for dressed full-term 24 to 27 º C • Reaction to cold – non-shivering thermogenesis (brown fat), vasoconstriction, restlessness, flexion posture • Reaction to heat - vasodilatation, sweating(?), hypoactivity, extension of posture Thermoregulation Newborn has 2.5 - 3 times higher body surface relatively to the body weight than adults – Radiation (39%) – Convection (34%) – Evaporation (24%) – Conduction (3%) – Sweating matures after 26 weeks Thermogenesis • Non - shivering thermogenesis Brown fat is about 6% of weight, located interscapular but also in mediastinum, axilla, etc. • Beware of maternal medication • Premature child Tubular function Glomerular filtration • Starts functioning between 9th to 12th gestational weeks • GFR increases with gestational age and during postnatal age systemic blood pressure, ↓ vascular resistance in splanchnic organs – ↑ • Complete maturation between 5th – 8th week of life (in immature infants later) • Activation of cortical glomeruli • GFR after birth = 1 – 2 ml/min/m2 • At the age of 1 month – 50 ml/min/m2 • Functional immaturity of tubules – juxtamedullar glomerulus - a shorter loop of Henle Properties: ⇒ Reduced efficiency countercurrent system ⇒ Reduced sensitivity to regulating hormones ⇒ Reduced concentration and dilution capacity ⇒ ↓ production of calcitriol (Vit D3) ↓ ability to maintain volume and composition of body fluids ↓ ability to quickly eliminate ionic charge and water to keep ABB Tubules maturate during 3rd – 5th month 5 Nota Bene • Immediate changes: – First breath, changes in circulation and Hgb – Apgar score – Closing of fetal shunts starts immediately after birth and continues through month-years – Cyanosis develops easily Thank you for your attention • All organs have low functional reserve (capacity), thus evry newborn is vulnerable to disturbances which in addition arise quickly and easily • Keep in mind critical periods of fetal and development 6