Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Saturated fat and cardiovascular disease wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Turner syndrome wikipedia , lookup
Cardiovascular disease wikipedia , lookup
Coronary artery disease wikipedia , lookup
Aortic stenosis wikipedia , lookup
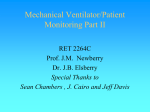
Relation Between Renal Function Within the Normal Range and Central and Peripheral Arterial Stiffness in Hypertension Giuseppe Schillaci, Matteo Pirro, Massimo R. Mannarino, Giacomo Pucci, Gianluca Savarese, Stanley S. Franklin, Elmo Mannarino Downloaded from http://hyper.ahajournals.org/ by guest on April 28, 2017 Abstract—Chronic kidney disease is accompanied by increased large-artery stiffness, but the relation between glomerular filtration rate within the reference range and central or peripheral arterial stiffness has been understudied. The link between renal function and arterial stiffness was assessed in 305 patients with never-treated essential hypertension (men: 58%; age: 48⫾11 years, blood pressure: 151/95⫾20/11 mm Hg), free from overt cardiovascular disease and with serum creatinine values ⬍1.4 mg/dL (men) and ⬍1.2 mg/dL (women), who underwent noninvasive aortic and upper-limb pulse wave velocity (PWV) determination. Aortic PWV was strongly related to age (r⫽0.55; P⬍0.001), whereas upper-limb PWV had a weaker nonlinear relation with age (⫽1.392; P⬍0.001 for age; ⫽⫺1.312; P⬍0.001 for age squared) and a weak relation with aortic PWV (r⫽0.22; P⬍0.001). Glomerular filtration rate (GFR), estimated according to the Mayo clinic equation for healthy subjects, was inversely correlated with large-artery stiffness, as assessed by aortic PWV (r⫽⫺0.34; P⬍0.001), and with peripheral artery stiffness, as assessed by upper-limb PWV (r⫽⫺0.25; P⬍0.001). In a multivariate linear regression, aortic PWV was independently predicted by age (⫽0.48; P⬍0.001), mean arterial pressure (⫽0.14; P⫽0.013), and GFR (⫽⫺0.13, P⫽0.029). Upper-limb PWV was predicted by GFR (⫽⫺0.24; P⬍0.001) and mean arterial pressure (⫽0.20; P⬍0.001). We conclude that, in hypertensive patients with normal renal function, an inverse relationship exists between GFR and stiffness of both central elastic and peripheral muscular arteries. These relations are in part independent from the effect of several confounders, including age, sex, and blood pressure values. (Hypertension. 2006;48:616-621.) Key Words: hypertension 䡲 glomerular filtration rate 䡲 pulse wave velocity 䡲 arterial stiffness 䡲 artery C transit time and, therefore, an estimate of arterial compliance, and that study suggests a relation between arterial stiffness and reduced GFR even in uncomplicated patients with essential hypertension. However, several questions remain unanswered in this regard. First, it is unknown whether kidney function is related to arterial stiffness within the reference range of estimated GFR. Second, it is currently not clear whether a reduced GFR is not only a correlate of arterial stiffness at the aortic level but also at the level of the peripheral arteries. QKD interval is a combination of transit time along the elastic ascending aorta and the predominantly muscular upper-limb arteries. Aorta and muscular upperlimb arteries are affected to a different extent by age and cardiovascular risk factors; unlike aortic PWV, upper-limb PWV is not affected by age significantly.13 The present investigation tested the hypothesis that in subjects with uncomplicated essential hypertension, changes ardiovascular disease is the leading cause of death in chronic kidney disease,1 and the development of premature and accelerated atherosclerosis in these patients is accounted for only in part by traditional risk factors.2 One possible mechanism for this association might be represented by increased arterial stiffness, which is both a predictor of cardiovascular disease3–5 and a correlate of reduced glomerular filtration rate (GFR).6 – 8 In patients with end-stage renal disease, a number of structural alterations of the arterial system occur, including stiffening of the aorta9 and of the radial artery, a muscular artery free of atherosclerosis.10 Among people with mild renal failure, arterial stiffness is directly related to GFR.11 In hypertensive patients, Gosse and Safar12 have observed that the time interval between the R wave on the ECG and the last Korotkoff sound heard over the brachial artery when measuring blood pressure ([BP] named the QKD interval) is directly related to estimated GFR. QKD interval is considered an approximate measure of arterial Received May 31, 2006; first decision June 20, 2006; revision accepted August 2, 2006. From the Unit of Internal Medicine (G. Schillaci, M.P., M.R.M., G.P., G. Savarese, E.M.), Angiology and Arteriosclerosis, University of Perugia, Perugia, Italy; and the Heart Disease Prevention Program (S.S.F.), University of California, Irvine, Calif. This paper was presented in part on November 14, 2005. at the American Heart Association Scientific Sessions, Dallas, TX. See Abstract: Schillaci G, Pirro M, Mannarino MR, Savarese G, Pucci G, Gemelli F, Vaudo G, Mannarino E. Renal dysfunction as an independent predictor of arterial stiffness in essential hypertension. Circulation. 2005;112:II-607. Correspondence to Giuseppe Schillaci, Unit of Internal Medicine, Angiology and Arteriosclerosis, University of Perugia Medical School, Hospital “S. Maria della Misericordia,” piazzale Menghini, 1, IT-06132 Perugia, Italy. E-mail [email protected] © 2006 American Heart Association, Inc. Hypertension is available at http://www.hypertensionaha.org DOI: 10.1161/01.HYP.0000240346.42873.f6 616 Schillaci et al in GFR may be related to changes in pulse wave velocity (PWV) at the level of the aorta and/or peripheral arteries. To investigate this hypothesis, we estimated GFR and determined aortic and upper-limb PWV in a consecutive series of hypertensive patients. To exclude the confounding effects of drug treatment, concomitant diseases, and overt chronic kidney disease, we examined a group of untreated, nondiabetic patients with essential hypertension who had normal serum creatinine levels. Methods Downloaded from http://hyper.ahajournals.org/ by guest on April 28, 2017 We examined 305 consecutive patients with essential hypertension (men: 58%; age: 48⫾11 years; BP: 151/95⫾20/11 mm Hg) who had been referred to our outpatient hypertension clinic between January 2003 and May 2005. Patients with uncomplicated essential hypertension were included in the study if they had been diagnosed with hypertension within the previous 3 years and had never received antihypertensive drug treatment. Exclusion criteria were clinical or laboratory evidence of heart failure, coronary heart disease, cerebrovascular disease, valvular defects, secondary causes of hypertension, serum creatinine ⱖ120 mol/L (1.4 mg/dL) in men and ⱖ106 mol/L (1.2 mg/dL) in women, proteinuria on the standard dipstick test, major noncardiovascular disease, dyslipidemia requiring pharmacological treatment, known diabetes or fasting glycemia ⱖ126 mg/dL, and treatment with any cardiovascular drug, including nitrates. Written informed consent was obtained from each patient, and the study protocol was reviewed and approved by the institutional ethics committee. All of the subjects underwent a careful clinical examination. Serum creatinine concentration was measured in an autoanalyzer (Technicon) by means of an automated technique measuring dialyzable Jaffe chromogen. This assay was calibrated daily by using the uncompensated method during the study period. Given that the abbreviated Modification of Diet in Renal Disease equation14 systematically underestimates GFR in high-GFR populations, and also the Cockcroft– Gault equation15 has insufficient precision in persons without chronic kidney disease,16 GFR was calculated according to the following formula, which has been developed and validated in a population of predominantly white adult subjects with normal renal function17: GFR (mL/min per 1.73 m2)⫽224⫻serum creatine⫺0.490⫻age⫺0.192⫻0.923 (if female), where serum creatinine is in milligrams per deciliter, and age is in years. Fasting blood samples were taken to perform routine blood chemistry. Waist circumference was measured with a soft tape on standing subjects at the iliac crest at the end of a normal expiration. After the subject had been resting in a supine position for 5 minutes, 3 consecutive measurements of BP and heart rate were obtained and averaged. Ambulatory BP was recorded with a validated oscillometric device (model 90207; SpaceLabs).18 After measuring BP, aortic and upper-limb PWV and pulse wave analysis were determined noninvasively with the commercially available SphygmoCor system (AtCor Medical), as described previously.19,20 Aortic (carotid-to-femoral) PWV was calculated from measurements of common carotid and femoral artery waveforms, and upper-limb (carotid-to-radial) PWV from common carotid and radial artery waveforms. Central artery waveforms were derived from the radial artery waveform, calibrated to brachial BP, by using a transfer function validated previously.21,22 Aortic augmentation was expressed either in absolute term or as a percentage of aortic pulse pressure (aortic augmentation index). Given the known dependence of aortic augmentation on heart rate (in the present population, ⫽⫺0.45 in women and ⫽⫺0.26 in men; both P⬍0.001), augmentation index was adjusted by heart rate on the basis of sex-specific regression equations. The same observer, unaware of the patient’s clinical and biochemical data, carried out all of the measurements. Statistical Analysis Continuous variables were tested to detect substantial deviations from normality by computing the Kolmogorov–Smirnov Z. The assumption of satisfactory normal distribution was met for all of the examined Glomerular Filtration Rate and Arterial Stiffness 617 variables, except for serum triglyceride concentration, which, because of its skewed distribution, was log-transformed before statistical analysis. Patients were grouped by tertile of estimated GFR. Differences among groups were tested using ANOVA and 2 test where appropriate, with post hoc Tukey’s honestly significant differences. Pearson’s correlation coefficients examined the bivariate associations between examined variables. Stepwise multiple regression analyses were used to evaluate which factors were independently associated with aortic and upper-limb PWV in the whole population. We investigated potential nonlinearity of relations of age and PWV by fitting multivariable models incorporating age and a quadratic term of age. Age, age squared, sex, smoking habits, body height, body mass index, physical activity, brachial mean arterial pressure, heart rate, duration of hypertension, and serum cholesterol concentration were included as independent variables in the multivariate models together with estimated GFR. The linear regression assumptions were confirmed by verifying normality of the distribution of residuals. Graphical inspection of scatter plots between predicted values of the dependent variable and regression-standardized residuals excluded any heteroscedasticity of distribution (data not shown). The final models were evaluated for other linear relationships among variables in the model (collinearity), which have the potential of rendering significance testing unreliable. Using standard diagnostic techniques, all of the models presented were found to be free from collinearity (tolerance: 0.76 to 0.97). Results Selected clinical and demographic characteristics of the 305 study patients are given in Table 1. Patients were grouped by tertiles according to their estimated GFR; partition values among tertiles were 106 and 117 mL/min per 1.73 m2. Patients in the bottom GFR tertile were older and more frequently men and had higher serum creatinine and cholesterol values. Moreover, brachial and synthesized aortic systolic and pulse pressures increased with decreasing GFR. In contrast, diastolic and mean BP values were not significantly different in the 3 groups. The groups did not differ by body mass index, waist circumference, smoking habits, and hypertension duration. As reported in Table 1, aortic PWV increased progressively with decreasing GFR. Also, upper-limb PWV increased ongoing from the top to the bottom GFR tertile. As depicted in the Figure, estimated GFR had a significant inverse relation with aortic PWV (r⫽⫺0.34; P⬍0.001), as well as with upper-limb PWV (r⫽⫺0.25; P⬍0.001). Aortic and upper-limb PWV correlated weakly each other (r⫽0.22; P⬍0.001). Both showed a direct association with brachial mean arterial pressure. As expected, aortic PWV increased steeply with age and had a significant relation with waist circumference and low body height (Table 2). No significant relationship was found between the square of age and aortic PWV. Upper-limb PWV had a significant nonlinear relation with age (⫽1.392, P⬍0.001 for age; ⫽⫺1.312, P⬍0.001 for age squared) and no significant associations with either waist circumference or body height. In a stepwise multiple regression model in which GFR was included as an explanatory variable together with age, age squared, sex, smoking habits, body height, body mass index, physical activity, brachial mean arterial pressure, heart rate, duration of hypertension, and serum cholesterol concentration, GFR was independently associated with aortic PWV along with age and office mean arterial pressure (Table 3). 618 Hypertension October 2006 TABLE 1. Selected Demographic and Clinical Characteristics of 305 Hypertensive Subjects by Tertile of Estimated GFR Estimated GFR, mL/min per 1.73 m2 Data ⱖ117 (n⫽101) Age, y 44 (10) Men, % 72 27.1 (4) 27.8 (4) Body mass index, kg⫻m⫺2 ⬍106 (n⫽101) P (F) 49 (9)* 54 (10)*† ⬍0.001 46* 48* 0.002 27.6 (4) 0.50 106 –117 (n⫽103) Waist, cm 94 (10) 95 (11) 95 (13) 0.73 Hypertension duration, y 1.4 (2) 1.5 (2) 1.3 (2) 0.37 Current smokers, % 26% 29% 27% 0.78 Serum cholesterol, mg/dL 197 (33) 208 (36) 214 (36)* Serum creatinine, mg/dL 0.87 (0.1) 0.91 (0.1) 1.03 (0.1)*† Brachial systolic BP, mm Hg 147 (16) 152 (21)* 155 (22)* 0.008 Brachial diastolic BP, mm Hg 94 (9) 95 (11) 95 (13) 0.79 111 (10) 114 (13) 115 (14) 0.08 Brachial mean BP, mm Hg Downloaded from http://hyper.ahajournals.org/ by guest on April 28, 2017 Brachial PP, mm Hg 0.002 ⬍0.001 53 (13) 56 (16)* 60 (17)* 0.003 Aortic systolic BP, mm Hg 135 (15) 141 (20)* 145 (20)* ⬍0.001 Aortic diastolic BP, mm Hg 96 (9) 96 (11) 95 (13) 0.83 109 (10) 111 (13) 112 (14) 0.10 Aortic mean BP, mm Hg Aortic PP, mm Hg 39 (12) 45 (14)* 50 (15)* ⬍0.001 24-h systolic BP, mm Hg 130 (10) 130 (11) 133 (14) 0.24 24-h diastolic BP, mm Hg 83 (10) 84 (8) 82 (10) 0.47 24-h mean BP, mm Hg 99 (9) 99 (9) 99 (10) 0.89 24-h PP, mm Hg 47 (7) 46 (7) 50 (11)*† 0.002 Aortic PWV, m/s 8.4 (1.8) 8.8 (1.8) 10.0 (2.7)*† ⬍0.001 Upper-limb PWV, m/s 8.7 (1.6) 9.4 (1.5)* 9.6 (1.6)* ⬍0.001 Aortic augmentation, mm Hg 10 (7) 14 (8)* 16 (9)* ⬍0.001 0.25 (0.12) 0.30 (0.13)* 0.31 (0.11)* ⬍0.001 Augmentation index Data are given as mean (SD). Augmentation index values are adjusted for heart rate. PP indicates pulse pressure. *P⬍0.05 vs I tertile; †P⬍0.05 vs II tertile. Low GFR, mean arterial pressure, and low body mass index were independent predictors of upper-limb PWV. Discussion This is the first study to demonstrate that GFR within the reference rang in patients with uncomplicated, untreated essential hypertension has a strong, independent inverse association with both central and peripheral arterial stiffness, as reflected by increased carotid-to-femoral and carotid-toradial PWV, respectively; in addition, the finding of an inverse relation between GFR and aortic augmentation index provided further support for increased central artery stiffness. Furthermore, the association between GFR and arterial stiffness remained significant after adjusting for the potential confounding influences of age, sex, distending pressure, and other major cardiovascular risk factors. The relation was also independent of average 24-hour ambulatory BP, which is a stronger predictor of cardiovascular risk than office BP in hypertension.23 Because aortic stiffness has been identified as an independent predictor of cardiovascular mortality in the specific setting of essential hypertension,4,5 we hypothesize that changes in arterial stiffness may, in part, mediate the well- known association between even mild reductions in GFR and cardiovascular risk in patients with hypertension.24,25 Kidney Disease and Peripheral Muscular Artery Stiffness Both central elastic and peripheral muscular arteries have been shown to be stiffer in end-stage renal disease. These findings were obtained measuring elastic modulus by the technique of high-resolution echo tracking,9,26 as well as measuring stiffness under isobaric conditions at the level of the radial artery.10 Among people with nondialysis-dependent renal insufficiency, a significant inverse relationship was found between GFR and aortic PWV.6 – 8 Previous studies on the relation between GFR within the reference range and arterial stiffness have been inconclusive. In 112 hypertensive subjects with normal or mildly reduced GFR, Mourad et al11 showed that reduced creatinine clearance was associated with increased stiffness of the musculoelastic carotid artery but not of the muscular radial artery. However, given the relatively weak association between GFR and upper-limb PWV, small sample size may have precluded the demonstration of a significant association in that study. In 263 hypertensive subjects with normal or mildly reduced GFR, Gosse and Safar12 found a positive relation between plasma Schillaci et al Glomerular Filtration Rate and Arterial Stiffness 619 TABLE 3. Independent Determinants of Aortic and Upper-Limb PWV in a Stepwise Multiple Linear Regression Analysis Variable Standardized Regression Coefficient Multiple R2 P Aortic PWV Age, y 0.48 0.30 ⬍0.001 Brachial mean pressure, mm Hg 0.14 0.32 ⬍0.001 ⫺0.13 0.34 0.029 ⫺0.24 0.07 ⬍0.001 0.20 0.11 ⬍0.001 ⫺0.12 0.12 0.034 GFR, mL/min per 1.73 m2 Upper-limb PWV GFR, mL/min per 1.73 m2 Brachial mean pressure, mm Hg Body mass index, kg⫻m⫺2 Age squared, sex, smoking habits, body height, physical activity, heart rate, duration of hypertension, and serum cholesterol concentration were included as explanatory variables but failed to enter the final models. Constant was 3.52 in the aortic PWV model and 10.47 in the upper-limb PWV model. Downloaded from http://hyper.ahajournals.org/ by guest on April 28, 2017 Scatterplots illustrating the relation of estimated GFR with aortic (top) and upper-limb (bottom) PWV. creatinine and QKD interval. Although correlated with more direct measures of arterial stiffness,27 the QKD interval depends on several other variables, including ventricular activation and body height, and represents a cumulative measure of aortic and upper-limb PWV velocity, so the effects of renal function on central and peripheral stiffness could not be distinguished in that article. Our study identifies for the first time a strong inverse association between GFR and arterial stiffness at both the aortic and peripheral level in a group of newly diagnosed, never-treated nondiabetic hypertensive subjects. These data demonstrate that significant alterations of the elastic properties of both elastic and muscular arteries appear at a very early stage of the disease, that is, in patients with normal estimated GFR. How Does Arterial Stiffness Affect Renal Function? Our cross-sectional study cannot establish causality relations, and it should be remembered that several cardiovascular risk factors, including aging, diabetes, and high BP, are known to TABLE 2. Bivariate Correlates of Aortic and Upper-Limb PWVs and of Estimated GFR Variable Upper-Limb PWV GFR Age 0.55* 0.09 ⫺0.42* Brachial mean pressure 0.23* 0.23* ⫺0.11 Body height Aortic PWV ⫺0.20* Body mass index Waist circumference GFR 0.03 0.11 0.02 ⫺0.11 ⫺0.05 0.19† ⫺0.05 ⫺0.04 ⫺0.34* *P⬍0.001; †0.05⬍P⬍0.001. ⫺0.25* increase, per se, the levels of arterial stiffness and plasma creatinine.28 However, we show that the association between GFR and arterial stiffness is independent of the confounding effect of age and other major risk factors. The possibility cannot be excluded that aortic stiffness might be responsible for a reduced GFR through an increase in aortic pulse pressure.29 Glomerular capillaries are exposed to relatively high mean and pulse pressures, approximating 60% of the arterial values. While ensuring a high filtration fraction, these high levels of pressure expose glomerular capillaries to potentially damaging pulse pressure. A hemodynamic effect of pulse pressure on the myogenic tone of afferent arterioles has been demonstrated in vitro in a perfused hydronephrotic rat kidney model.30 The glomerulus is selectively exposed to pulsatile forces affecting capillary pressure,31 and these mechanisms may contribute to glomerulosclerosis. However, our data show that GFR has an independent impact not only on aortic PWV, but also on peripheral PWV. This might have pathogenetic implications. In fact, different arterial segments respond differently to aging. Aorta, an elastic artery, loses its compliance with advancing age, whereas compliance in the peripheral, predominantly muscular arteries seems less closely related to age.13 The common link of 2 unrelated measures of arterial stiffness with GFR might suggest a direct, age-independent implication of kidney function in arterial stiffness. Interestingly, Bahous et al32 demonstrated recently that healthy kidney donors develop increased aortic PWV. The possibility cannot be ruled out, however, that increased peripheral muscular artery stiffness might increase early wave reflection by shortening the sites of wave reflection, thus increasing arterial pulsatility and cardiac afterload, as well indirectly affecting renal function. In the present study, an inverse relationship was also found between GFR and aortic augmentation index. Augmentation index, a composite parameter that depends on the reflective properties of the distal arterial bed, as well as on elastic properties of the large arteries, is a measure of the extra hemodynamic burden imposed on the heart and a predictor of cardiovascular events in patients with ischemic heart disease.33 This finding highlights the adverse potential cardiac 620 Hypertension October 2006 consequences of even minor changes in renal function in hypertension. Can Chronic Kidney Disease Cause Arterial Stiffness? Downloaded from http://hyper.ahajournals.org/ by guest on April 28, 2017 Our results are in agreement with the hypothesis that a mildly reduced kidney function might be responsible for increased arterial stiffness. Interestingly, in a large longitudinal study of patients with essential hypertension, Benetos et al34 found that serum creatinine level was a major determinant of accelerated progression of arterial stiffness. Mechanisms causing increased arterial stiffness in renal patients are not fully understood: over and above the effects of age and standard cardiovascular risk factors, an increase in the calcium content of the arterial wall has been demonstrated in hemodialysis patients35,36 and also in patients with moderate chronic renal failure.37 Several other mechanisms could be involved, including endothelial dysfunction,38 activation of the renin–angiotensin–aldosterone system,39 and qualitative and quantitative changes in the arterial wall, such as advanced glycation end products, lipid peroxidation, elastin fragmentation, vascular smooth muscle cell hyperplasia, increased collagen content, and reduced amount of elastic fibers.40,41 Limitations Some limitations of this study should be acknowledged. Our results were obtained in a middle-aged, white, uncomplicated, untreated hypertensive population, and inferences with regard to other ethnicities, older individuals, treated subjects, and high-risk populations should be made with caution. The Mayo clinic formula represents only an approximation of true creatinine clearance, and it is well known that any formula for estimating GFR tends to be less accurate in subjects with normal renal function than in patients with chronic kidney disease.17 However, in comparison with other widely used formulas for the estimation of GFR, it has been shown to be more accurate and less subject to systematic bias, at least in populations with normal GFR.17 This being a cross-sectional study, causations discussed above should be considered as hypothetical. Perspectives By showing that GFR influences arterial functional properties that are related to cardiovascular risk, our findings provide a pathophysiological background for understanding the associations between renal function and arterial stiffness–related cardiovascular morbidity and mortality. The fact that a relation between GFR and significant changes in the elastic properties of central and peripheral arteries is present in hypertensive subjects with fully normal renal function suggests a role of even minimally impaired renal function in affecting arterial stiffness and may give an explanation for the strong link between creatinine values within the reference range and cardiovascular complications in hypertensive subjects.24,25 Clearly, further studies are needed to elucidate the pathophysiological implications of these findings. Source of Funding This work was supported in part by the grant 2004060902 from the Italian Ministry for University and Scientific Research. Disclosures None. References 1. Muntner P, He J, Hamm L, Loria C, Whelton PK. Renal insufficiency and subsequent death resulting from cardiovascular disease in the United States. J Am Soc Nephrol. 2002;13:745–753. 2. Baigent C, Burbury K, Wheeler D. Premature cardiovascular disease in chronic renal failure. Lancet. 2000;356:147–152. 3. Blacher J, Safar ME, Guerin AP, Pannier B, Marchais SJ, London GM. Aortic pulse wave velocity index and mortality in end-stage renal disease. Kidney Int. 2003;63:1852–1860. 4. Laurent S, Boutouyrie P, Asmar R, Gautier I, Laloux B, Guize L, Ducimetiere P, Benetos A. Aortic stiffness is an independent predictor of all-cause and cardiovascular mortality in hypertensive patients. Hypertension. 2001;37:1236 –1241. 5. Laurent S, Katsahian S, Fassot C, Tropeano AI, Gautier I, Laloux B, Boutouyrie P. Aortic stiffness is an independent predictor of fatal stroke in essential hypertension. Stroke. 2003;34:1203–1206. 6. Wang MC, Tsai WC, Chen JY, Huang JJ. Stepwise increase in arterial stiffness corresponding with the stages of chronic kidney disease. Am J Kidney Dis. 2005;45:494 –501. 7. Lacy P, Carr SJ, O’Brien D, Fentum B, Williams B, Paul SK, Robinson TG. Reduced glomerular filtration rate in pre-dialysis non-diabetic chronic kidney disease patients is associated with impaired baroreceptor sensitivity and reduced vascular compliance. Clin Sci (Lond). 2006;110: 101–108. 8. Briet M, Bozec E, Laurent S, Fassot C, London GM, Jacquot C, Froissart M, Houillier P, Boutouyrie P. Arterial stiffness and enlargement in mildto-moderate chronic kidney disease. Kidney Int. 2006;69:350 –357. 9. London GM, Guérin AP, Marchais SJ, Pannier B, Safar ME, Day M, Metivier F. Cardiac and arterial interactions in end-stage renal disease. Kidney Int. 1996;50:600 – 608. 10. Mourad JJ, Girerd X, Boutouyrie P, Laurent S, Safar ME, London GM. Increased stiffness of radial artery wall material in end-stage renal disease. Hypertension. 1997;30:1425–1430. 11. Mourad JJ, Pannier B, Blacher J, Rudnichi A, Benetos A, London GM, Safar ME. Creatinine clearance, pulse wave velocity, carotid compliance and essential hypertension. Kidney Int. 2001;59:1834 –1841. 12. Gosse P, Safar ME. Arterial stiffness and plasma creatinine in untreated hypertensive patients. Am J Hypertens. 2005;18:1140 –1145. 13. van der Heijden-Spek JJ, Staessen JA, Fagard RH, Hoeks AP, Boudier HA, van Bortel LM. Effect of age on brachial artery wall properties differs from the aorta and is gender dependent: a population study. Hypertension. 2000;35:637– 642. 14. Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of Diet in Renal Disease Study Group. Ann Intern Med. 1999;130:461– 470. 15. Cockcroft DW, Gault MH. Prediction of creatinine clearance from serum creatinine. Nephron. 1976;16:31– 41. 16. Coresh J, Stevens LA. Kidney function estimating equations: where do we stand? Curr Opin Nephrol Hypertens. 2006;15:276 –284. 17. Rule AD, Larson TS, Bergstralh EJ, Slezak JM, Jacobsen SJ, Cosio FG. Using serum creatinine to estimate glomerular filtration rate: accuracy in good health and in chronic kidney disease. Ann Intern Med. 2004;141: 929 –937. 18. Schillaci G, Verdecchia P, Borgioni C, Ciucci A, Gattobigio R, Sacchi N, Benemio G, Porcellati C. Predictors of diurnal blood pressure changes in 2042 subjects with essential hypertension. J Hypertens. 1996;14: 1167–1173. 19. Schillaci G, Pirro M, Vaudo G, Mannarino MR, Savarese G, Pucci G, Franklin SS, Mannarino E. Metabolic syndrome is associated with aortic stiffness in untreated essential hypertension. Hypertension. 2005;45: 1078 –1082. 20. Schillaci G, De Socio GV, Pirro M, Savarese G, Mannarino MR, Baldelli F, Stagni G, Mannarino E. Impact of treatment with protease inhibitors on aortic stiffness in adult patients with human immunodeficiency virus infection. Arterioscler Thromb Vasc Biol. 2005;25:2381–2385. 21. Pauca AL, O’Rourke MF, Kon ND. Prospective evaluation of a method for estimating ascending aortic pressure from the radial artery pressure waveform. Hypertension. 2001;38:932–937. 22. Chen CH, Nevo E, Fetics B, Pak PH, Yin FC, Maughan WL, Kass DA. Estimation of central aortic pressure waveform by mathematical trans- Schillaci et al 23. 24. 25. 26. 27. 28. Downloaded from http://hyper.ahajournals.org/ by guest on April 28, 2017 29. 30. 31. 32. formation of radial tonometry pressure: Validation of generalized transfer function. Circulation. 1997;95:1827–1836. Verdecchia P. Prognostic value of ambulatory blood pressure: current evidence and clinical implications. Hypertension. 2000;35:844 – 851. Schillaci G, Reboldi G, Verdecchia P. High-normal serum creatinine concentration is a predictor of cardiovascular risk in essential hypertension. Arch Intern Med. 2001;161:886 – 891. De Leeuw PW, Thijs L, Birkenhager WH, Voyaki SM, Efstratopoulos AD, Fagard RH, Leonetti G, Nachev C, Petrie JC, Rodicio JL, Rosenfeld JJ, Sarti C, Staessen JA; Systolic Hypertension in Europe (Syst-Eur) Trial Investigators. Prognostic significance of renal function in elderly patients with isolated systolic hypertension: Results from the Syst-Eur trial. J Am Soc Nephrol. 2002;13:2213–2222. London GM, Guerin AP, Pannier B, Marchais SJ, Safar ME. Large artery structure and function in hypertension and end-stage renal disease. J Hypertens. 1998;16:1931–1938. Abassade P, Baudouy PY, Gobet L, Lhosmot JP. Comparison of two indices of arterial distensibility: temporal apparitions of Korotkoff sounds and pulse wave velocity. A Doppler echocardiography and ambulatory blood pressure monitoring study (in French). Arch Mal Coeur Vaiss. 2001;94:23–30. Oliver JJ, Webb DJ. Noninvasive assessment of arterial stiffness and risk of atherosclerotic events. Arterioscler Thromb Vasc Biol. 2003;23:554–566. Mitchell GF. Increased aortic stiffness: an unfavorable cardiorenal connection. Hypertension. 2004;43:151–153. Loutzenhiser R, Bidani A, Chilton L. Renal myogenic response: kinetic attributes and physiological role. Circ Res. 2002;90:1316 –1324. Cortes P, Zhao X, Riser BL, Narins RG. Regulation of glomerular volume in normal and partially nephrectomized rats. Am J Physiol. 1996;270: F356 –F370. Bahous SA, Stephan A, Blacher J, Safar ME. Aortic stiffness, living donors, and renal transplantation. Hypertension. 2006;47:216 –221. Glomerular Filtration Rate and Arterial Stiffness 621 33. Weber T, Auer J, O’Rourke MF, Kvas E, Lassnig E, Lamm G, Stark N, Rammer M, Eber B. Increased arterial wave reflections predict severe cardiovascular events in patients undergoing percutaneous coronary interventions. Eur Heart J. 2005;26:2657–2663. 34. Benetos A, Adamopoulos C, Bureau JM, Temmar M, Labat C, Bean K, Thomas F, Pannier B, Asmar R, Zureik M, Safar M, Guize L. Determinants of accelerated progression of arterial stiffness in normotensive subjects and in treated hypertensive subjects over a 6 –year period. Circulation. 2002;105:1202–1207. 35. Blacher J, Guerin AP, Pannier B, Marchais SJ, London GM. Arterial calcifications, arterial stiffness, and cardiovascular risk in end-stage renal disease. Hypertension. 2001;38:938 –942. 36. Haydar AA, Covic A, Colhoun H, Rubens M, Goldsmith DJ. Coronary artery calcification and aortic pulse wave velocity in chronic kidney disease patients. Kidney Int. 2004;65:1790 –1794. 37. Russo D, Palmiero G, De Blasio AP, Balletta MM, Andreucci VE. Coronary artery calcification in patients with CRF not undergoing dialysis. Am J Kidney Dis. 2004;44:1024 –1030. 38. Perticone F, Maio R, Tripepi G, Zoccali C. Endothelial dysfunction and mild renal insufficiency in essential hypertension. Circulation. 2004;110: 821– 825. 39. Safar ME, Benetos A. Factors influencing arterial stiffness in systolic hypertension in the elderly: role of sodium and the renin-angiotensin system. Am J Hypertens. 2003;16:249 –258. 40. Yamamoto Y, Sakata N, Meng J, Sakamoto M, Noma A, Maeda I, Okamoto K, Takebayashi S. Possible involvement of increased glycoxidation and lipid peroxidation of elastin in atherogenesis in haemodialysis patients. Nephrol Dial Transplant. 2002;17:630 – 636. 41. Amann K, Wolf B, Nichols C, Tornig J, Schwarz U, Zeier M, Mall G, Ritz E. Aortic changes in experimental renal failure: hyperplasia or hypertrophy of smooth muscle cells? Hypertension. 1997;29:770 –775. Relation Between Renal Function Within the Normal Range and Central and Peripheral Arterial Stiffness in Hypertension Giuseppe Schillaci, Matteo Pirro, Massimo R. Mannarino, Giacomo Pucci, Gianluca Savarese, Stanley S. Franklin and Elmo Mannarino Downloaded from http://hyper.ahajournals.org/ by guest on April 28, 2017 Hypertension. 2006;48:616-621; originally published online September 4, 2006; doi: 10.1161/01.HYP.0000240346.42873.f6 Hypertension is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2006 American Heart Association, Inc. All rights reserved. Print ISSN: 0194-911X. Online ISSN: 1524-4563 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://hyper.ahajournals.org/content/48/4/616 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Hypertension can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Hypertension is online at: http://hyper.ahajournals.org//subscriptions/